Abstract
Objective: To compare the
efficacy and safety of intravenous iron with blood transfusion in post partum
women with symptomatic iron deficiency anaemia.
Methods: Ninety women were
included in the study. The inclusion criteria were: hemoglobin <9g/dl and/or
haematocrit <28%, mean corpuscular volume <80fl, ferritin level
<15ng/ml, and symptoms of anaemia within 48 hours of delivery. Women with
postpartum haemorrhage and haemodynamic instability were excluded. Women were
divided into two groups, group B received blood transfusion and group I received intravenous iron sucrose (400mg infusion in
250ml Normal Saline over half an hour) (Venofer, Vifor St Gallen's, Switzerland).
The outcome measures were relief of symptoms of anaemia. Hemoglobin, haematocrit,
mean corpuscular volume and ferritin levels were measured before and one week
after the treatment.
Results: The two
groups were comparable in terms of age, mode of delivery and symptoms. Group B
had a mean age of 31.1 years (22-39) vs. 32.3 years (20-43). Twenty four
women from group B had C/S vs. 23 women in group I. However, women in
group B had a lower baseline mean hemoglobin (6.8 g/dl (4-8) vs. 7.7g/dl
(6.1-9 g/dl) and lower haematocrit (23.2 %( 18-26) vs. 25.3 %( 18-28). At
one week post treatment the mean rise in hemoglobin was 2.35 g/dl (34%) in group
B vs. 2.15g/dl (27%) in group I. The mean rise in haematocrit was 7.0 %
and 6.3% respectively. The mean rise in ferritin level was higher in group I
(220%) vs. 150% in group B. Symptoms
relief occurred in 29 cases in group B and in 28 cases in group I. No serious
side effects occurred in either group.
Conclusion: Intravenous iron sucrose
is an effective and safe treatment for postpartum iron deficiency anaemia. It
is hoped that this treatment will reduce the need for blood transfusion.
Key words: Blood transfusion,
Intravenous iron, Iron deficiency anaemia, Postpartum anaemia
JRMS March 2011; 18(1): 15-19
Introduction
Post partum anaemia
complicates 10% of deliveries.(1) Milder forms of anaemia,
defined as Haemoglobin (Hb) less than 10g/dl, still occurs in 30% of cases. Worldwide, iron deficiency is the most common
cause of pathological anaemia in pregnancy.
The prevalence is 18% in the developed world,
but reaches up to 56% in the developing world.(2) The
negative iron balance in pregnancy is aggravated by blood loss around the time of
delivery, especially after Caesarean section (C/S).(3)
Severe anaemia may cause
cardiovascular strain and dyspnoea. More commonly it causes tiredness, headache
and dizziness. This can be debilitating especially when caring for the newborn.
Women may also have an increased risk of post partum depression.(4)
Blood transfusion in the
postpartum period is not uncommon ranging from 2-10%.(5,6) It
is more common after C/S than vaginal delivery.(7) The
transfusion trigger is clinician dependant and varies between institutions. A
significant proportion of transfusions are thought to be given inappropriately.(8)
Blood transfusion may be necessary, but it is not without risk. Recipients
may develop allogenic reactions, and more rarely, transfusion transmitted
infections, as well as suffering immunological sequels such as red cell
alloimmunisation. Additionally, there are the problems of incompatible
transfusions, availability and rising costs. Unfortunately, information from
randomised clinical trials to inform best practice is largely unavailable in
the discipline of blood transfusion.(9) Therefore, blood
transfusion should be given only when absolutely necessary.
Parenteral iron has been
traditionally used in women intolerant to oral iron.(10) More
recently, it has been shown to achieve a faster correction of haemoglobin
levels and iron stores.(11,12) Previous preparations, namely
iron dextran had a poor reputation of anaphylactoid reactions. However, iron
sucrose has been safely administered in cases where previous intolerance to
iron dextran has been encountered.(13) Iron sucrose has been used in a series of 500
patients with not a single reported anaphylactic reaction.(14)
In our study women with
symptomatic post partum anaemia who would have had a blood transfusion, were
given a trial of intravenous iron sucrose.
Methods
The
study was a prospective controlled non- randomized study. Ninety women with
symptomatic post partum anaemia were recruited from the postnatal ward within
48 hours of delivery. Patients were assigned to two groups. Group B received
blood transfusion and group I received a total dose of 400mg of
intravenous iron sucrose (Venofer Vifor St Gallen's, Switzerland). In our unit,
Hb is checked at the time of presentation to labour ward. It is repeated 24
hours after C/S or if otherwise clinically indicated. Blood transfusion is
rarely indicated in the stable patient when Hb is greater than 10g/dl and is
almost always indicated when less than 6g/dl.(15) Therefore,
our inclusion criteria were: Hb level between 6 and 9g/dl and or Haemotocrit
(Hct) level between 20% and 28%, Mean corpuscular volume (MCV) < 80fl and
ferritin level <15ug/l.
Symptoms
and signs of anaemia included tiredness, dizziness and pallor. More severe
symptoms, namely fainting and evidence of cardiovascular strain were excluded
from the study as these patients
should receive blood transfusion. However, all patients
recruited into the study, would have received blood transfusion according to
our local practice of managing post partum anaemia. Other exclusion criteria
were haemodynamic instability, intolerance to iron therapy, asthma, hepatorenal
disease, anaemia from causes other than iron deficiency and blood transfusion
in the peripartum period.
The
assigned treatment was started 24-48 hours after delivery on the post natal
ward. Intravenous iron (Venofer) was given in two divided doses 200mg on day 1
and 200 mg on day 2 after delivery. Venofer was diluted in 250 ml of normal
saline and given over half an hour. Pulse and Blood pressure were checked
before, during and after each infusion. Facilities for cardiopulmonary
resuscitation were available on the ward.
In group B, blood transfusion was carried out on the post natal ward. Packed
RBC’s were used as women were haemodynamically stable. On average women
received 2.3 units of blood (range 1-4). Each unit was given over two hours.
Blood pressure, pulse and temperature were measured half hourly during the
transfusion.
The primary outcome measures
were: Hb level and relief of symptoms of anaemia one week after treatment.
Secondary outcome measures included Haematocrit and ferritin levels one week
after the treatment, and reported adverse events encountered during and after
both treatments.
Complete blood counts were
measured by Haematology analyzer (Sysmex K-1000, Japan). Ferritin level was measured
by new fully Automated Assay (Immulite 2000, Siemens, Germany).
Statistical analysis was conducted
using the two tail t-test for equality of variances. Statistical significance
was confirmed when P was < 0.05.
Results
All women received the
treatment they were assigned (n = 90). The two groups were similar in baseline clinical characteristics (Table I) and symptoms profile. Most cases (80%) of anaemia in both groups followed C/S. This is compatible with previous studies.(5,7)
Table I. Baseline
clinical characteristics
|
Characteristics
|
Group B (n=45)
|
Group I (n=45)
|
P
value
|
|
Age
|
31.2
(6.5)
|
30.72
(5.5)
|
0.624
|
|
Caesarean section
|
38(84%)
|
36(80%)
|
0.581
|
|
Hb
(before treatment) (g/dl)
|
7.7
(0.85)
|
7.9
(0.76)
|
0.146
|
|
Haematocrit (%)
|
24.5
(1.85)
|
25.0
(1.77)
|
0.208
|
|
Ferritin (ng/ml)
|
7.1
(3.9)
|
7.4
(4.72)
|
0.673
|
|
MCV
|
71
(4.81)
|
69.3
(4.92)
|
0.233
|
Data are given as mean (SD)
Table II. Laboratory
data 7 days after treatment
|
|
Group B (n=45)
|
Group I (n=45)
|
|
Hb (g/dl)
|
10.05
(8.9-11.8)
|
10.1(8.8-11.5)
|
|
Haematocrit (%)
|
32.3(29-36)
|
31.8(29-35)
|
|
Ferritin
(ng/ml)
|
17.6(2.4-28)
|
22.6(4.3-40)
|
Data are given as
mean(range)
Table III. Laboratory parameters differences after treatment
|
|
Group B
|
Group I
|
P
value
|
|
Hb day7 - Hb baseline
|
2.35
|
2.15
|
<0.05
|
|
Hct day7-Hct baseline
|
7.0
|
6.3
|
<
0.05
|
|
Ferritin day7- Ferritin baseline
|
10.5
|
15.2
|
0.10
|
Hemoglobin(Hb) g/dl. Haematocrit (Hct) %. Ferritin
ng/ml
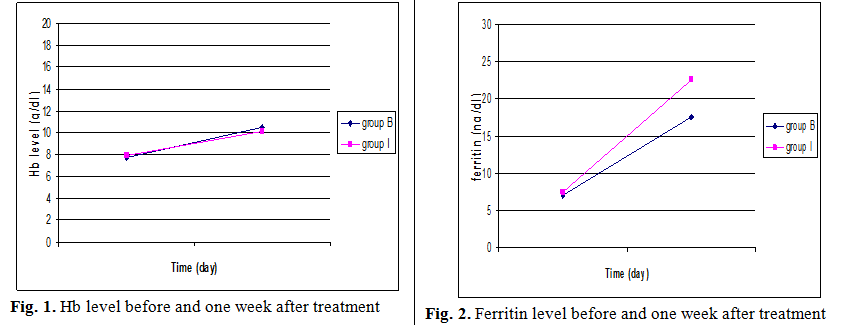
Both treatments significantly
increased Hb (2.35g/dl for group B vs. 2.15g/dl for group I) and Hct (7.0%
vs. 6.3%) levels 7 days after treatment (see Table II and Fig. 1).
This increase was higher in group B than group I. The difference was
statistically significant regarding both parameters, (t=38.2 and 27.2
respectively, P < 0.05 for both). Patients in group I increased their
ferritin level by 220% compared to 150% in group B (see Table III and Fig. 2). This
difference was also statistically significant, but in favour of group I (t=18.6
(P < 0.05).
Symptoms
relief occurred in 29 cases in group B and in 28 cases in group I. In those cases where symptoms persisted, a
repeat course of treatment was performed.
No anaphylaxis or other serious side effects were encountered with Iron
Sucrose. However, two patients reported facial flushing and three patients
described a metallic taste. Neither of these necessitated stopping the
infusion.
In the blood transfusion group, two cases developed pruritis, two cases
developed pyrexia, one case of rash, and one case of jaundice secondary to
haemolysis, that resolved after four days. Women, who developed mild symptoms,
were treated and re-transfused. There were no severe side effects as to
completely abandon the transfusion. One woman developed jaundice one day after
completion of 4 units of blood transfusion. She was managed conservatively and
jaundice gradually resolved.
Discussion
The study was performed to
ascertain whether intravenous iron sucrose can be used in women with
symptomatic iron deficiency anaemia, who otherwise would receive blood
transfusion.
In an audit of three obstetric
units (total of 13,000 deliveries per annum) prior to this study, we found the
transfusion rate to be 15% following C/S and 4% following vaginal delivery.
This mounts to 728 blood transfusions per year (6.2% of all deliveries).(6) Transfusion rate was estimated to be lower in
other studies (0.3% to 1.7% for vaginal delivery and 0.7% to 6.8% for C/S).(16,7) The higher
transfusion rate in our audit was due to the high incidence of
pre-existing anaemia, but also possibly due to lower physician's threshold for initiating a transfusion.
Anaemia in our population is more common due to grand multiparity, nutritional
deficiency and poor compliance with antenatal oral iron supplementation.
Indeed, a significant proportion (15%) of women, in our audit enter labour with
Hb level<10g/dl and 5% of cases have Hb<8 g/dl.
Oral iron, parenteral iron and
erythropoietin are all treatments that have been used in postpartum iron
deficiency anaemia. The use of oral iron is limited by its side effects, poor
compliance and the fact that it takes a long time to correct low Hb and iron
stores, taking 40 days in one study, before a satisfactory maximum effect was
reached.(11)
It is generally accepted that
intravenous iron induces a similar or slightly more rapid erythropoietic
response than oral iron. However, this statement applies to iron dextran,
sorbitol and gluconate treatment but may not be generalized to iron sucrose.(17) The latter seems to be
effective within few days of administration. This is due to its rapid removal
from plasma and incorporation into the bone marrow for eryhtropoiesis.
Therefore, when a rapid effect is required parenteral iron is indicated, and
iron sucrose seems to be the most appropriate. Both iron dextran and iron
gluconate cause unpredictable anaphylactic reactions and require test dose
before administration. However, iron sucrose is reported to be safe and
effective and can be administered without a test dose.(18,14)
Intravenous iron sucrose has
also been compared to intramuscular iron sorbitol. Not only was it more
effective, but also 20% of patients in the Sorbitol group dropped out of the
study due to intolerance.(19)
Despite widespread use of iron
sucrose in dialysis patients, its use is not common in obstetrics, as many
physicians are not familiar or comfortable with the use of this medication.(18) However, the
safety of iron sucrose, demonstrated in previous studies,(18,13)
somewhat reduced the anxiety associated with other parenteral iron
preparations, namely iron dextran and gluconate.
Intravenous iron has also been
shown not to interfere with lactation, emphasizing previous reports of active
biological mammary gland regulation of milk iron concentration.(20)
Intravenous iron sucrose avoids the risks associated with blood transfusion and
is more cost effective.(21) In our study, we have shown that intravenous
iron sucrose can be used safely and effectively in acute postpartum anaemia.
Recombinant Human
Erythropoietin (rhEPO) is mostly used in the treatment of anaemia of end stage
renal disease. However, it has also been used both antenatally and postpartum
in women.(22) In one
study, it has been shown to safely enhance the efficacy of intravenous iron
sucrose in gestational iron-deficiency anaemia.(23) However,
in a randomized controlled trial of 60 patients, the addition of rhEPO to iron
sucrose did not further increase Hb levels one and two weeks after treatment of
postpartum iron deficiency anaemia. Additionally, rhEPO is much more expensive.(24)
We performed a Medline search
on anaemia and pregnancy. Although intravenous iron was compared to oral iron
in the management of antenatal(25,12)
and postpartum(11) anaemia, no studies where cited comparing
blood transfusion to intravenous iron in symptomatic iron deficiency anaemia.
However, a retrospective study observed the influence of the availability of intravenous
iron for post partum anaemia. It demonstrated a reduction in blood transfusion
(15 vs. 5) after the introduction of Venofer. The inclusion criteria did
not refer to symptoms of anaemia.(21) In another retrospective study, it was shown that
blood transfusion would be avoided by the use of IV iron in women with Hb<8g/dl.
The study was not controlled, and intravenous iron was reserved for
asymptomatic patients.(26)
Since the introduction of intravenous
iron in our units the number of blood transfusions has been reduced by half
without many negative effects on maternal well being.
In general, once haemostasis
and haemodynamic stability around delivery has been achieved, the residual
anaemia may be treated by intravenous iron. Iron sucrose seems to be the
preferred choice.
The significant rise in Hb level (around 2g) in
one week after IV iron is more than expected for non pregnant patients. This
could be explained by the fact that haemodilution, a particular feature of pregnancy
resolves after delivery and causes a higher than expected Hb level.
With the limited number of patients and power
of the study, the study demonstrated that intravenous iron is almost as effective as
blood transfusion in our cohort of patients. The statistically significant finfings
demonstrating a better rise in Hb at 7 days, may not be clinically significant
considering the minimal difference between the two Hb values achieved (2.35 vs.
2.15) and the overlapping confidence intervals of Hb post delivery( Group B Hb
10.05 (8.9-11.8) g/dl and group I Hb
10.1 (8.8-11.5) g/dl ).
Limitation
of the Study
Our study extended to one week
after the treatment. However, further studies should be performed to assess the
influence of both blood transfusion and intravenous iron over a longer period
of time.
Conclusion
Intravenous
iron sucrose is an effective and safe treatment for postpartum iron deficiency
anaemia. It is hoped that this treatment will reduce the need for blood
transfusion.
References
1.Agent P. Iron and women in
the reproductive years in: The British nutrition foundation’s task force. First
edition London:
Chapman and Hall 1995; P 110-118
2.Allen LH. Pregnancy and Iron
deficiency. Unresolved issue. Nutrition Reviews 1997; 55: 91-101.
3. Letsky EA. Eryhtropoiesis in
pregnancy. J of Perinatal Medicine 1995; 23: 39-45
4.Corwin E, Murray-Kolb L, Beard
J. Low
haemoglobin is a risk factor for postpartum depression. J Nutr 2003;
133:4139-4142.
5.Klapholz H. Blood transfusion
in contemporary obstetric practice. Obstet Gynecol 1990; 75: 940-943
6. Khamaiseh K, Tahat Y, et al. Incidence of
postpartum anaemia and blood transfusion in two busy obstetric hospitals in
Jordan 2008. Unpublished date.
7.Dickason LA, Dinsmoor MJ. Red blood cell
transfusion and caesarean section. Am J Obstet Gynecol 1992; 167:327-332
8.Silverman JA, Barret J, Callum
TL.
The appropriateness of red cell transfusion in the preripartum patient. Obstet
Gynecol 2004; 104:1000-1004
9.Royal college of Obstetricians
& Gynaecologists. Blood transfusion in obstetrics. RCOG guideline No
47, Dec 2007; page 1-10
10.Singh K, Fong Y. Intravenous iron polymaltose complex for treatment of
iron deficiency anaemia in pregnancy resistant to oral iron therapy. Eur J
Haematol 2000; 64: 272-274.
11.Bhandal N, Russel R. Intravenous vs. Oral iron therapy for postpartum anaemia. BJOG
2006:113:1248-1252.
12.Al RA, Unlubilgin E, Kandemir
O, et al. Intravenous vs. Oral iron for treatment of anaemia in
pregnancy. Obstet Gynecol 2005; 106(6):1335-1340.
13. Bastani B, Rahman S, Gellens M, et al. Lack of reaction to
ferric gluconate in hemodialysis patients with a severe reaction to iron
dextran. ASAIO J 2002; 8(4): 404- 406.
14.Perewunsayk G, Hurch R, Hurch A, et al. Pareneteral iron
therapy in Obstetrics, eight years experience with iron sucrose complex. Br
J Nutr 2002; 88: 3-10
15.British Committee for standards in Haematology; Blood Transfusion Task force. Guidelines for the
clinical use of red cell transfusions. Br J Haematol 2001; 113: 24-31
16.Andres R, Piacquadio K, Resnik R, et al. A reappraisal of the
need for autologous blood donation in the obstetric patient. Am J Obstet
Gynecol 1990; 163:1551-1553
17.Seid M, Derman R, Baker J, et al. Ferric carboxymaltose injection
in the treatment of postpartum iron deficiency anaemia: A randomized controlled
clinical trial. Am J Obstet Gynecol 2008; 199: 435-438.
18. Silverstein SB, Rodgers GM. Parenteral iron therapy options. Am J
Hematol 2004; 76:74-81
19. Wali A, Mushtaq A. Comparative study-Efficacy, safety and compliance of
intravenous iron sucrose and intramuscular sorbitol in iron deficiency anaemia
in pregnancy. J Pak Med Assoc Sep 2002; 52(9): 392-395
20.Breymann C, Von Seefried B, Stahel M et al. Milk iron content
in breast-feeding mothers after administration of IV iron sucrose complex. J
Perinat Med 2007; 35(2): 115-118
21.Bozhinova S, Ivanova I, Lukanova M. How to avoid a
haemotransfusion which is not life saving? Our experience with administration
of IV Iron to pregnant women and young mothers. Akush Ginekol Sofiia
2004; 43(6): 13- 17
22.Breymann C, Richter R, Hunter C, et al. Effectiveness of RH
EPO and Iron sucrose therapy alone in patients with postpartum anaemia and blunted
erythropoiesis. Eur J Clin Invest
2000; 30:156-161
23. Breymann C, Visca E, Huch R, et al. Efficacy and safety of
intravenously administered iron sucrose with and without adjuvant recombinant
human erythropoietin for the treatment of resistant iron-deficiency anaemia
during pregnancy. Am J Obstet Gynecol 2001; 184: 662-667
24.Wagstrom E, Akesson A, Van-Rooijen M, et al. Erythropoietin and
intravenous iron therapy in post partum anaemia. Acta Obstet Gynecol Scand
2007; 86(8): 957-962
25. Al-Momen K, Al-Mishari A, et al. Intravenous iron sucrose
complex in the treatment of iron deficiency anaemia during pregnancy. Eur J
Obstet Gynecol Reprod Biol 1996; 69:121-124
26. Broche DE, Gay C. Acute postpartum
anaemia. Clinical practice and interest of intravenous iron. Gyecologie,
Obstetrique & Fertilite 2003; 32:613-619.