Abstract
Objective:
To study suture related complications after penetrating Keratoplasty and
their role in the success of corneal graft surgery, and to define postoperative
management outlines.
Methods: The descriptive study was conducted on
patients who underwent penetrating Keratoplasty at King
Hussein Medical
Center in Amman, Jordan
between March 2005 and February 2009. It
included 75 patients, they were followed for suture related complications
during their routine visits, the clinical findings recorded at follow up visits
included epithelial erosions around sutures, sterile infiltrates, infectious
keratitis, loose or broken sutures, and wound dehiscence after suture removal.
Results: Spontaneous loosening or breakage of sutures
occurred in 12 patients (16%), at an average of 7 months post surgery. Suture
related abscesses were seen in 4 patients (5.3%) at an average of 14 months.
Sterile infiltrates were seen in 10 patients (13.3%) at an average of 6 months.
Suture erosions over the nylon sutures were found in 6 patients (8 %) at an
average of 10 months, while four patients (5.3%) presented with broken sutures
and leaking wound at an average of 10 months.
Conclusion:Proper postoperative care is important for a
successful penetrating keratoplasty. Suture related complications frequently
occur after penetrating keratoplasty. Prompt
and proper management is essential and will result in earlier visual
rehabilitation and greater long-term graft survival.
Key
words:
Penetrating, Keratoplasty, Suture-related complications
JRMS March 2011;
18(1): 30-33
Introduction
The outcome of corneal transplantation
depends on skilled long term care.(1) The postoperative
course of Penetrating Keratoplasty (PKP) is often complicated by suture-related
problems.(2) Sutures play an important role in wound
stability,(3) and their disruption can lead to significant
and often unpredictable increase in corneal astigmatism.(4,5)
Corneal ulcers, graft rejection and even
endophthalmitis had all been reported following suture removal. On the other hand
sutures can loosen, become exposed, and serve as nidus for infection. Retained
monofilament sutures can cause foreign body sensation, corneal ulcer, tarsal
and graft rejection.(6)
Our aim is to study suture related
complications following PKP and their effect on success of corneal graft
surgery, and to define postoperative management outlines.
Methods
This
descriptive study was conducted on patients who underwent PKP at King Hussein
Medical Center
(Royal Medical Services) in Amman,
Jordan between March 2005 and February 2009. It included 75 patients, who were followed up for suture related complications during their routine visits. All surgeries were performed by three expert surgeons using the same procedure and there were no intra-operative complications. All sutures were well buried, with a minimum follow up period of 15 months.
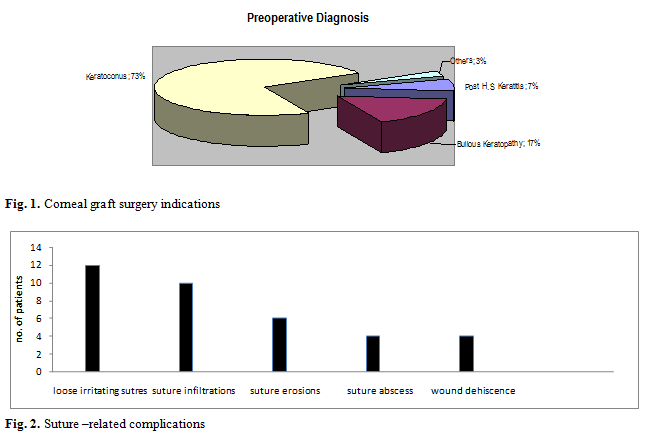
The
main indications for grafting were keratoconus followed by psuedophakic bullous
keratopathy, herpes simplex keratitis, and corneal dystrophies (Fig. 1).
Patient’s
pre-operative information included age, sex, systemic disease, lid
abnormalities, pre-existing ocular surface disease and corneal vascularization,
surgical indications and preoperative medications. Patients were followed up
for a minimum of 2 years and the follow-up protocol normally included 12
scheduled examinations in the first year, and 4
examinations in the second year and 6 monthly thereafter.
The
clinical findings recorded at follow up visits included epithelial defects
around sutures, sterile infiltrates, infectious keratitis, loose or broken
sutures, and wound dehiscence after suture removal.
Sutures
were not normally removed before 12 months unless they were loose, causing
irritation or severe astigmatism by topography.
Results
Eighty-three
eyes of 75 patients were followed up for a minimum of two years. In three patients the PKP was a redo
procedure, in four patients cataract extraction was done with Intra Ocular Lens
insertion in two of these patients.
An
allograft reaction occurred in four patients, two of them presented with sub
epithelial dots, the third had Khodadoust endothelial rejection line, while in
the fourth patient the rejection was suture related; it was associated with
irritating loose suture and early vascularization around the suture, however
reversal of the graft rejection was possible in all four patients by increasing
the regimen of topical steroid medications as well as a short course of
systemic steroids.
The
main indication for PKP was keratoconus (n=55), followed by psuedophakic
bullous keratopathy (n=13), herpes simplex corneal opacity (n=5), and other
causes (n=2) as shown in Fig. 2.
Table
1.
Post-operative time interval of suture related complication following keratoplasty
|
Complication
|
No.
|
%
|
Average time (months)
|
Range (months)
|
|
Loose irritating sutures
|
12
|
16
|
7± 5.16
|
1-15
|
|
Sterile infiltrates
|
10
|
13.3
|
6± 2.58
|
2-9
|
|
Erosions
|
6
|
8
|
10± 4.69
|
2-15
|
|
Suture Abscess
|
4
|
5.33
|
14± 10.73
|
7-30
|
|
Traumatic wound dehiscence
|
4
|
5.33
|
10± 5.56
|
9-15
|
Spontaneous
loosening or breakage of sutures occurred in 12 patients, two of them required
re-suturing due to early wound dehiscence or manifest leakage from the wound. The
average time interval between PKP and the occurrence of breakage was seven
months (SD±5.16, range 1-15 months) (see Table I).
Suture
related abscesses were also seen in four patients, they came complaining of
pain and injected eyes. Two of them had ulcerative epithelial defects with
stromal infiltrates adjacent to loose irritating sutures while the other two
presented with infiltrates and hypopyon one week following selective suture
removal. All patients were cultured, the results revealed Streptococcus pneumoniae
in two patients, Staphylococcus aureus in one patient, and no growth in the
fourth patient; this however was considered infectious because of the presence
of hypopyon and good response to fortified topical antibiotic treatment. The average
time between surgery and occurrence of abscesses was 14 months (SD±10.73, range
7-30 months).
Three
of these patients were admitted to hospital; all were treated with daily
sub-conjunctival injection of antibiotics for four days and vigorous topical
fortified eye drops and responded well.
One
of the patients developed endophthalmitis and received intravitreal antibiotic
injection and also responded well but experienced a decrease of two lines of
visual acuity.
Sterile
infiltrates were found in 10 patients (13.3%), mostly as small sub-epithelial
infiltrates adjacent to sutures more often on the recipient side. All were symptom free and only were detected
at routine follow up visits. Close
observation was necessary and none of them progressed to ulcers or abscesses
and therefore no culture and sensitivity tests were performed.
These
infiltrates were encountered at an average of 6 months post PKP (SD±2.58, range
2-9 months), most of infiltrates disappeared over the follow up course.
Suture
erosions over the nylon sutures were also recorded in six patients (8%) throughout the post operative
follow-up period at an average of 10 months (SD±4.69, range 2-15 months). Patients
reported a foreign body sensation, the eroding sutures were removed and broad
spectrum topical antibiotics were prescribed with close follow up and symptoms
disappeared with no sequel on vision.
Three
patients presented with broken sutures and leaking wound following trauma, this
incidence occurred in keratoconus young patients with age range 13-18 years;
however one other patient with graft following psuedophakic bullous keratopathy
developed wound dehiscence following suture removal 12 months after surgery,
average time from surgery was 10 months (SD±5.56, range 5-8 months).
Discussion
In
our study, 6 patients developed suture erosions within an average time of 10
months (±4.69) post surgery, this finding was inconsistent with previous
studies published by Dana et al. who reported 33 months,(7)
and Siganos et al. who reported 31.6 months).(8) This finding
is probably related to our policy of removing all sutures between 12-18 months
post surgery; as the suture erosion tends to escalate with increased elapsed
time from surgery, especially beyond the two year postoperative period.(7)
Suture
abscesses occurred at an average of 10 months, this goes with average time
reported by Tseng et al.(9) of 10.4 months,
and 8.6 months according to Huang et al.; however suture related
abscesses were reported at 21.5 months post surgery according to Leahy et al.,(11)
and 27.1 months in the study conducted by Sanchez-Perez et al.(12)
The micro organisms reported in the studies performed by Leahy et al.(11)
and Christo et al.(2) were similar to species found in culture
results of our study.
Broken or loose sutures in need for repair occurred
only in one patient as it occurred in the early post-operative period; while
the patients who presented with loose irritating sutures did not need
intervention, because they occurred later in postoperative course, and the
tensile strength of the wound was good.
Wound
dehiscence after suture removal occurred in one patient (1.3%) while in his
study Christo et al.(2) reported nine cases (2.5%). Post
traumatic wound dehiscence occurred in three patients which was also reported
by Lam et al.(13) they were caused by assault in two
patients and due to accidental falling down in the third patient. Wound dehiscence is a cause for concern as corneal wounds almost never regain the
original strength of the original graft even several years after meticulous
repair.(13)
Corneal
infiltrates were found in 13.3% of patients at an average of six months, this
goes with Brady’s findings,(14) who described suture related
immune infiltrates in the early post-operative period. They were multiple,
mostly on host side of the graft-host interface with no overlying epithelial
defect, and so they were not cultured.
It
seems a good policy to remove the sutures between 12-18 months post PKP
surgery, as it helps quick rehabilitation and the use of contact lenses with
minimal suture related complications. The
frequency of keratoplasty suture erosions and the serious morbidity associated
with them dictates that the long term retention of these sutures should be
recognized as a risk factor for the development of postoperative infection.(7)
In
reviewing patients included in our study, loose irritating sutures
necessitating removal and suture related
infiltrates which need close follow up were the most common presenting suture
related complications. These clinical
conditions should not be ignored, as delay in management may result in sight
threatening complications.
Conclusion
Proper
postoperative care is critical for successful PKP. The anticipation of post
operative complication in patients is important, and preventative measures
should be taken. When complications do occur, prompt and proper management is
essential, this will ensure earlier visual rehabilitation and greater long-term
graft survival.
References
1.
McNeill JI. Indications and outcomes.
Cornea surgery of the cornea and conjunctiva, 2nd edition. Krachmer,
Mannis, Holland,
Elseviere Mosby. 2004; Volume II, Chapter117, pages1413, 1422.
2.
Christo CG, Van Rooij J, Geerards
AJM, Remeijer L, Beekhuis WH. Suture related complications following
Keratoplasty a 5- year retrospective study. Cornea 2001; 20(8): 816-819.
3.
Melles GRH, Binder PS. Acomparison of
wound healing in sutured and unsutured corneal wounds. Arch Ophthlmol
1990; 108:1460-1469.
4.
Frueh BE, Feldman ST, Feldman RM, et
al.
Running nylon suture dissolution after penetrating Keratoplasty. Am J
Ophthalmol 1992; 113:406-411.
5.
Shaw EL, Brightbill FS. Suture removal.
In: Corneal surgery, Theory, Technique, and Tissue. Brightbill FS ed. Boston, Mosby publication
1999; chap.19, 447-453.
6. Weiss JL, Nelson JD, Lindstrom RL,
Doughman DJ.
Bactterial endophthalmitis following penetrating Keratoplasty suture removal. Cornea
1984; 5(3): 278.
7. Dana MR, Goren MB,
Gomes JAP, et al. Suture erosion
after penetrating Keratoplasty. Cornea 1995; 14:243-248.
8.
Siganos CS, Solomon A, Frucht-Prey
J. Microbial
findings in suture erosion after penetrating Keratoplasty. Ophthalmology
1997; 104:513-516.
9.
Tseng SH, Ling KC. Late microbial
keratitis after corneal transplantation. Cornea 1995; 14(6): 591-594.
10.
Huang SC, Wu SC, Wu WC, Hong HL. Microbial
Keratitis- a late complication of penetrating Keratoplasty. Trans R Soc Trop Med Hyg 2000 May-Jun; 94(3):315-317.
11.
Leahy AB, Avery RL, Gottsch JD, Mallette RA,
Stark WJ.
Suture Abscesses after penetrating Keratoplasty. Cornea 1993; 12(6):489-492.
12.
Sanchez PA, Bueno LJ, Brito SC, et
al.
Study of infectious Keratitis in corneal graft.Arch Soc Esp Oftalmol. Oct; 75(10):659-663.
13.
Lam FC, Rahman MQ, Ramaesh K. Traumatic wound
dehiscence after penetrating keratoplasty- a cause for concern. Eye 2007;
21:1146-1150.
14. Brady SE, Rapuano CJ, Arentsen JJ, Cohen EJ, Laibson PR. Clinical Indications for and procedures associated with penetrating Keratoplasty, 1983-1988. Am J Ophthalmol 1989; 108:118-122.