ABSTRACT
Objectives:
Laparoscopic inguinal hernia repair has been promoted as having significant
advantages. The aim of this study is to evaluate the early results of total
extra peritoneal laparoscopic inguinal hernia repair at the Royal Medical
Services hospitals of Jordan Armed Forces.
Methods: During
the period between April 2004 to May 2006, 100 patients underwent total extra
peritoneal laparoscopic inguinal hernia repair, the following data were
collected; patient age, gender, side and type of hernia, intra-operative complications,
conversion of the procedure to other type of repair, operative time,
postoperative pain, hospital stay, postoperative complications, chronic pain
and recurrence.
Results: Out of the 100 patients, two patients (2%) were females
and 98 (98%) were males. Age ranged between 16 and 79 years with a mean of 44.8
years. According to body mass index 22 (22%) patients were moderately obese.
All of the patients were fit for general anesthesia. The 100 patients had 115
hernias, 53 (53%) on the right side, 32 (32%) on the left side and 15 (15%)
bilateral. Sixty five (56.5%) hernia
were indirect, 47 (40.9%) were direct and 3 (2.6%) were pantaloon hernia. Six (5.2%)
of the hernias were recurrent. Operative time ranged between 35 to 165 minutes
with a mean of 61.3 minutes, in the unilateral hernia the mean operative time
was 56 minutes while in the bilateral cases it was 88 minutes. The procedure was
converted to open repair in 2% of patients and to trans-abdominal preperitoneal
laparoscopic repair in other 2% of patients. Intra-operative complications occurred
in 5% of patients while post-operative complications occurred in 9% of patients
all of which were mild. Post operative pain was assessed by the visual analogue
scale twice; immediately after complete recovery from general anesthesia and in
the first post operative day. In the first; it was severe in 9%, moderate in
81% and mild in 10% of patients, while in the second it was severe in 2%,
moderate in 12% and mild in 86% of patients. Chronic pain occurred in 3% of
patients. Recurrence occurred in 8 (8%) patients, six of them were from the
first 50 cases.
Conclusion: Our results in total extra peritoneal laparoscopic
inguinal hernia repair were comparable to the results reported in literature
regarding complication rate and recurrence rate especially after passing the
first fifty cases indicating the effect of learning curve.
Key words: Inguinal hernia, Laparoscopic, Total Extra Peritoneal
repair.
JRMS
June 2011; 18(2): 5-10
Introduction
Within less than a
decade in the 1990s, laparoscopic surgeons described different forms of
laparoscopic inguinal hernia repairs, the most widely accepted of them nowadays
are the Total Extra Peritoneal repair (TEP) and the Transabdominal Periperitoneal
repair (TAPP). The TEP approach supposes an entirely parietal procedure that treats
the hernias by combining the concepts of Stoppa (preperitoneal repair with
giant mesh) and of Lichtenstein (hernioplasty with mesh without tension) but
can be carried out by using appropriate laparoscopic instruments that allow the
option of a minimally invasive procedure with its demonstrated benefit for the
patient.(1)
Laparoscopic hernia repair is now widely
performed and has been demonstrated to be safe and cost-effective, and is no
longer a substitute or modification of other open techniques, but it is a
separate therapeutic option for patients, and should not be considered a newer
experimental option to treat inguinal hernia, as it has been in use for many
years and is now well developed, with consolidated technological support. At the
time being there is general agreement that laparoscopic approach is the
approach of choice in case of recurrent or bilateral inguinal hernia.(2). This study was conducted to evaluate the
early results of total extra peritoneal laparoscopic inguinal hernia repair at
the Royal Medical Services hospitals of Jordan Armed Forces.
Methods
During the period between
April 2004 to May 2006, 100 patients underwent TEP laparoscopic inguinal hernia
repair, their data was collected and studied, only patients with urgent
obstructed hernia, and patients who were not fit for general anesthesia were
excluded from the study. The following data were collected; patient age, gender,
side and type of hernia, intra-operative complications, conversion of the
procedure to other type of repair, operative time, postoperative pain, hospital
stay, postoperative complications, chronic pain and recurrence.
Out of the 100 patients, two patients (2%) were
females and 98 (98%) were males. Age ranged between 16 and 79 years with a mean
of 44.8 years. According to body mass index 22 (22%) patients were moderately obese.
All of the patients were fit for general anesthesia. The 100 patients had 115
hernia, 53 (53%) on the right side, 32 (32%) on the left side and 15 (15%)
bilateral. Sixty five (56.5%) hernia were indirect, 47 (40.9%) were direct and
3 (2.6%) were pantaloon hernia. Six (5.2%) of the hernias were recurrent.
All patients were operated upon under general endotracheal
anesthesia. The patient is put in the supine position, the whole abdominal wall
and genitalia and thighs are scrubbed. The procedure is started by infra
umbilical incision at the same side of hernia deep down to the anterior rectus
sheath (Fig. 1). The anterior rectus sheath is then incised for one to two
centimeters (Fig. 2), blunt dissection is done behind the rectus muscle
dissecting the extra- peritoneal space using the surgeon’s index finger, and a
10 millimeters trocar is inserted through this wound into the extra-peritoneal
space which is inflated with carbon dioxide to a pressure up to 10-15
millimeter mercury. Two more infra umbilical 5 millimeter trocars are inserted
in the midline (Fig. 3). The extraperitoneal space is dissected both sharply
and bluntly identifying the anatomical landmarks mainly the inferior epigastric
vessels, pubic bone, rectus muscle, the linea alba in the midline, and the
spermatic cord. The henial sac is then identified and it’s relation to the
inferior epigastric vessels is visualized to determine whether the hernia is
direct or indirect one. Even with the presence of obvious direct hernia, the
cord is dissected gently looking for indirect sac or lipoma of the cord which
if present, should be reduced and excised as they can cause hernia-like
symptoms in the absence of a true hernia and this can lead to unsatisfactory
results, in this stage care should be taken in order not to injure the vas
deference and the spermatic vessels (Fig. 4). In case of inguino- scrotal
hernia of the sac is dissected for a short distance beyond the internal
inguinal ring and transected there with good hemostasis, the proximal part is
reduced leaving the distal part in place (Fig. 5). The space is dissected
laterally up to the anterior superior iliac spine and medially just beyond the
midline in case of unilateral hernia or extended to the contra lateral anterior
superior iliac spine in case of bilateral hernia.
A longitudinally rolled 10 x 15 cm polypropylene mesh
is introduced through the 10-12 mm trocar of the camera and unrolled inside as a curtain to cover the hernial orifices,
then it is fixed by three tissue tacker clips, one in the upper lateral angle,
second in the upper medial angle, and the third one over pubic bone. The space
is then deflated under vision taking care that the lower edge of the mesh does
not roll upward. The incision in the rectus sheath is closed and then the skin
wounds.
Patients were allowed to have regular diet after complete
recovery from general anesthesia. Post-operative pain is evaluated using the Visual
Analogue Scale (VAS) of pain upon immediate complete recovery from anesthesia
and in the first post operative day, patients were asked to rate their pain
with the VAS which consists of 100 millimeter
line, they were asked to mark on the line that represent their level
of perceived pain intensity.
Table I. Intra operative complications.
|
Inferior
epigastric vessels injury.
|
3%
|
|
External
iliac vein injury
|
1%
|
|
Small
intestine injury
|
1%
|
|
Total
|
5%
|
Table II.
Post operative complications
|
Scrotal
Hematoma.
|
6 (6%)
|
|
Infection.
|
1 (1%)
|
|
Milde
Epididimytis.
|
1 (1%)
|
|
Pain
from a subcutaneous migration of spiral titanium clip.
|
1 (1%)
|
|
Total
|
9 (9%)
|
Zero score represent no pain, scores from 1 to 30 were
defined as having mild pain, scores from 31 to 69 were defined as having
moderate pain, and those with scores of 70 or more were considered to have
severe pain. Patients were given 75 mg intramuscular Diclofinac Sodium as analgesic
according to the pain evaluation. They were discharged from the hospital on the
first post-operative day to be followed in the outpatient clinic at two weeks
interval for one month, then every three months for three years.
Results
Operative time ranged between 35 to 165 minutes with a
mean of 61.3 minutes, in the unilateral hernia the mean operative time was 56
minutes while in the bilateral cases it was 88 minutes. The procedure was converted
to open repair in two (2%) patients, the first due to bleeding from the
inferior epigastric vessels and injury of the small intestine during trying to
control this bleeding, the second was due to injury of iliac vein. On the other
hand the procedure was converted to trans-abdominal preperitoneal laparoscopic
repair (TAPP) in two (2%) patients because we could not enter the extra
peritoneal space due to previous mid line laparatomy incision.
Intra-operative complications occurred in 5% of
patients (Table I), they included; injury to the inferior epigastric vessels in
3 (3%) patients, injury to small intestine in one (1%) patient, and injury to
the iliac vein in one (1%) patient. The injury to the small intestine occurred
during re-insertion of the 5 millimeter trocar that slipped out during attempts
to stop bleeding from the inferior epigastric vessels. All of these intra
operative problems occurred in the first 50 cases of our experience.
Post-operative complications occurred in 9% of patients
(Table II). Scrotal hematoma occurred in 6 (6%) patients, all of them responded
to conservative treatment and the hematomas disappeared spontaneously in few
weeks. Infection occurred in 1 (1%) patient in whom we had to remove the mesh
to control the infection. Mild epididimytis happened in 1 (1%) patient and he responded to oral antibiotics and
anti inflammatory analgesic drugs. Pain from a subcutaneous migration of the spiral
titanium clip occurred in 1 (%) patient; pain disappeared after removal of the
clip under local anesthesia. Apart from two cases of scrotal hematomas, all
these complications occurred in the first 50 cases.
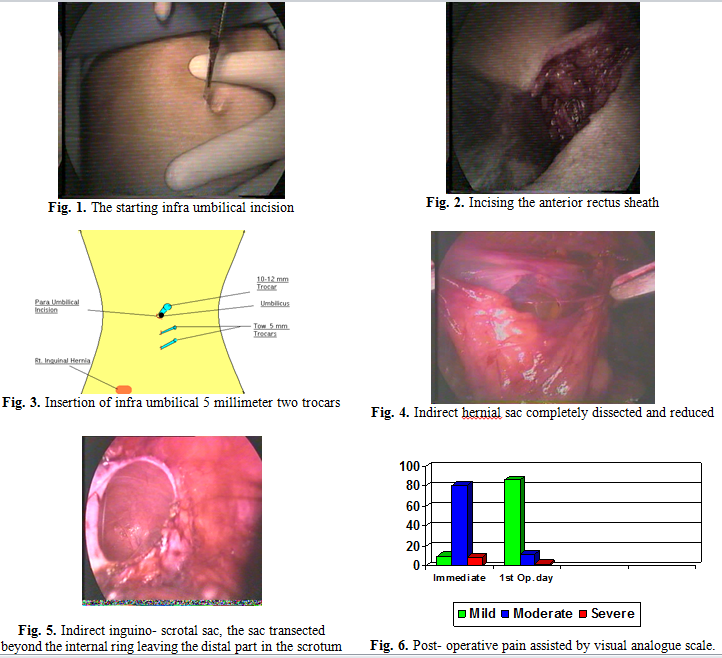
Post operative pain assessment using the (VAS) as
described above showed that; immediately after complete recovery from general
anesthesia; it was severe in 9%, moderate in 81% and mild in 10% of patients,
while in the first post operative day it was severe in 2%, moderate in 12% and
mild in 86% of patients, (Fig. 6). Chronic pain (pain that lasts for more than
six months) occurred in 3% of patients. Recurrence occurred in 8 (8%) patients,
six of them were in the first 50 cases.
Discussion
Inguinal hernia is the
most common hernia, and its repair is one of the most frequently performed operations
in general surgery.
Two revolutions in inguinal
hernia repair surgery have occurred during the last two decades. The first was
the introduction of tension-free hernia repair by Lichtenstein in 1989, which
significantly reduced recurrence rates. The second revolution was the
application of laparoscopic surgery to the treatment of inguinal hernia in the
early 1990s, which led to decrease in postoperative pain and faster recovery
along with low recurrence rates.(3)
Two laparoscopic
techniques have become the most common procedures to repair these hernias: the
TAPP and the TEP repair. Dulucq JL were the first to perform laparoscopic TEP
repair, in June 1990.(3)
In both methods mesh
prosthesis is implanted into the preperitoneal space dorsal to the
transversalis fascia. These techniques therefore represent minimally invasive
versions of open mesh implantation techniques. In TAPP the surgeon enters the
peritoneal cavity and places a mesh through a peritoneal incision over possible
hernia sites, while in TEP the peritoneal cavity is not entered and mesh is used to seal the hernia from
outside the peritoneum which is considered to be an advantage for TEP procedure
over TAPP.
TEP approach is
considered to be more difficult than TAPP but may result in fewer complications.
The TAPP approach has been advocated for complicated hernias.
The TEP repair affords
efficient access to both groins. It uses a posterior approach and avoids
anterior scar tissue in the case of recurrent hernias.(4)
The Royal College of
Surgeons' of England review of groin hernia surgery suggests that laparoscopic
repair gives less postoperative pain, a faster recovery, and similar recurrence
and complication rates to open repair .(5) The
recommendations of the UK National Institute for Clinical Excellence (NICE)
advised that laparoscopic hernia should be limited to the recurrent or
bilateral hernia and TEP approach is the preferred, and primary unilateral
hernia is preferred to be repaired by open tension free repair (Lichtenstein).(2)
our comment on these recommendations comes in two points: first; if the surgeon
is not trained to do laparoscopic repair for the easier unilateral primary
hernia, he will not be able to do laparoscopic repair for the more difficult
bilateral or recurrent cases, and second; patients who have bilateral or recurrent
hernias are the minority of cases, 10% bilateral and 6% recurrent.(6)
(in our study 15% and 5% respectively), while the majority of patients have
primary unilateral hernia, these patients have the right to benefit from the
advantages of laparoscopic surgery namely less post operative pain, faster
recovery, and early to return for normal activity.
The two most important
end points in inguinal hernia surgery are; chronic pain and recurrence.
Regarding our study the incidence of chronic pain (pain that lasts for more
than six months) was 3%. The reported incidence of chronic pain 6 months to 1
year after inguinal herniorrhaphy varies from 0% to 37%, with most reports
being in the range of 10%–20%. In a questionnaire study 1 year after inguinal herniorrhaphy,
Morten Bay-Nielsen et al found that 28.7% had groin pain with no difference in
the incidence of pain between laparoscopic and open repair.(7)
Another retrospective questionnaire study reported, however, a chronic pain
rate of 38.3% after open and 22.5% after laparoscopic repair (P, 0.01).(8)
In a recent Cochrane review including 41 published and unpublished reports involving
7161 patients, laparoscopic repair was also found to lead to a significantly
lower incidence of persisting pain compared with open herniorrhaphy.(9)
Emilie Øberg et al found that chronic groin pain incidence in their patients
(who had TAPP) is 4%, which is less than in most other studies.(10)
Taylor CJ found that although
ongoing chronic pain complicated 14% of there patients who had TEP repair, pain
was in almost all cases of a mild and occasional nature that allowed a full
return to pre-hernia activities .(6) These data are similar
to findings by other authors.(11) Randomized studies have
shown significant improvements in post operative pain and rehabilitation rates
in comparison to suture repair done by the Shouldice or Lichtenstein techniques.(12)
The second end point
in hernia repair surgery is recurrence; this complication became less with
introduction of tension free, mesh repair. Recurrence in laparoscopic inguinal
hernia repair occur usually early (within 6 months) and it is usually due to
technical error.(13)
Mike SL et al
compared recurrence rates between conventional anterior repair and laparoscopic
repair (TEP) Recurrences were diagnosed in 31 patients (6%) in the open-surgery
group and 17 (3%) in the laparoscopic-surgery group (P<0.05). With
prolonged follow-up, more recurrences may be expected in the open-surgery
group, and these late recurrences may be prevented only by reinforcing the
groin region with additional support. A late recurrence after laparoscopic
surgery may be uncommon because mesh is used routinely to reinforce the groin
region from inside. The rationale for covering the defect in the abdominal wall
with mesh from inside is that the repair can better withstand the pressure (which
originates inside the abdomen) to which it is subjected. The difference in
recurrence rates in the two groups can therefore be expected to increase over
time. Early recurrence in general may be caused by technical errors as missing
present lateral hernia, insufficient lateral preperitoneal dissection resulting
in curled mesh, using small size mesh, and leaving big lipoma of the cord not
dissected.(14)
In our study we reported 8% (8 hernias) incidence
of recurrence, 75% (6 out of 8 hernias) of them were in the first 50 patients
which reflects the effect of learning curve.
The European Hernia
Trials Group, found that the incidence of recurrence in laparoscopic and
Lichtenstein repair were similar (2.3% and 2.9%, respectively).(12)
The experience of the surgeon in laparoscopic hernia repair was found to play a major role in recurrence rate.
Surgeons who had done
more than 250 laparoscopic repairs had a 5% recurrence rate; this rate is half
that for “less experienced” surgeons.(15)
The patients returned
to work sooner after laparoscopic repair than after open repair, as reported in
several trials.(14,16) In Mike SL et al study, the
difference was appreciable (a median of seven days). This difference may be
explained by the absence of an inguinal incision, the absence of dissection of
muscle in the groin during laparoscopic repair, and the tension-free repair, as
well as the lower complication rate.(14)
As what happened to
our 8th patient, small bowel injury caused by trocar insertion was
reported in literature,(16) these injuries unless recognized and managed
early, fatal complications may be unpreventable.(17)
Recently single-incision
laparoscopic surgery (SILS) was used to repair inguinal hernia through the TEP
approach, the first case in which this technique was used was reported by
Filipovic-Cugura J et al.(18)
Conclusion
Our results in total
extra peritoneal laparoscopic inguinal hernia repair were comparable to the
results reported in literature regarding complication and recurrence rates
especially after passing the first 50 cases indicating the effect of learning
curve.
References
1.Moreno-Egea
A, Torralba-Martınez JA, et
al. Laparoscopic Approach in Inguinal Hernia A Single Technique and a
Tactical Resource. Surg Laparosc Endosc Percutan Tech 2005; 15(5): 261-262.
2.2001/001
National Institute for Clinical Excellence. Guidelines
for the Use of Laparoscopic Surgery for the Treatment of Inguinal Hernias in
the NHS. London:
National Institute for Clinical Excellence, 2001.
3.Dulucq
Jl, Wintringer P, Mahajna A. Laparoscopic
totally extraperitoneal inguinal hernia repair: lessons learned from 3.100
hernia repairs over 15 years. Surg
Endosc 2009; 23: 482-486.
4.Schneider
BE, Castillo JM, Villegas L, et al. Laparoscopic Totally Extraperitoneal Versus
Lichtenstein Herniorrhaphy: Cost Comparison at Teaching Hospitals. Surgical
Laparoscopy, Endoscopy & Percutaneous Techniques 2003; 13(4): 261-267.
5.Beattie
DK, Foley RJE, Callam MJ.
Future of laparoscopic inguinal hernia surgery. Br J Surg 2000; 87: 1727-1728.
(Short note).
6. Taylor
CJ, Wilson T. Long-term
results of laparoscopic totally extra-peritoneal inguinal herniorrhaphy. ANZ J Surg 2005; 75: 637–639.
7.Bay-Nielsen
M, Perkins F, Kehlet H. Pain
and functional impairment 1 year after inguinal herniorrhaphy: a nationwide
questionnaire study. Ann Surg 2001; 233 (1): 1–7.
8.Kumar
S, Wilson RG, Nixon SJ, et al. Chronic pain after laparoscopic
and open mesh repair of groin hernia. Br J Surg 2002; 89:1476–1479. (Abstract)
9. McCormack
K, Scott N, Go PMNYH, et al. Laparoscopic techniques versus open
techniques for inguinal hernia
repair (Cochrane Review). The Cochrane Library Oxford: Update Software. 2003 Issue 3.
10.Øberg E, Jacobsen B, Rosenberg J. Chronic pain and recurrence after laparoscopic
inguinal herniorrhaphy. Surg Laparosc Endosc Percutan Tech 2005; 15 (5):
267-269.
11.Lau H, Patil NG, Yuen WK, et al.
Prevalence and severity of
chronic pain after endoscopic totally extraperitoneal inguinal hernioplasty. Surg
Endosc 2003; 17: 1620- 1623. (Abstract)
12.Hernia EU, Collaboration T. Laparoscopic compared with open methods of groin
hernia repair: systematic review of randomised controlled trials. Br J Surg
2000; 87:860-867.
13.Lal P, Kajla RK, Chander J, et al. Laparoscopic total extraperitoneal (TEP) inguinal
hernia repair, overcoming the learning curve. Surg Endosc 2004; 18:
642–645
14. Liem MSL, Graaf YVD, Steensel CJV, et
al. Comparison of conventional
anterior surgery and laparoscopic surgery for inguinal hernia repair. N Engl
J Med 1997; 336(22): 1541-1547.
15.Grunwaldt LJ, Schwaitzberg SD,
Rattner DW, et al. Is laparoscopic
inguinal hernia repair an operation of the past? J Am Coll Surg 2005;
200 (4): 616-620.
16.Felix EL, Michas CA, Gonzalez Jr MH. Laparoscopic hernioplasty: Why does it work? Surg
Endosc 1997; 11: 36–41.
17.Neumayer L, Giobbie-Hurder A,
Jonasson O, et al. Open mesh versus laparoscopic mesh repir of inguinal
hernia. N Engl J Med 2004; 350: 1819-1827.
18. Filipovic-Cugura J, Kirac I, Kulis T,
et al. Single-Incision
Laparoscopic Surgery (SILS) for totally extraperitoneal (TEP) inguinal hernia
repair: first case. Surg Endosc 2009; 23: 929-921.