ABSTRACT
Objectives: To assess the efficacy of ultrasound guided compression therapy for the treatment of post catheterization femoral pseudoaneurysms.
Methods:A retrospective review of 21 patients who underwent ultrasound guided compression for treatment of post catheterization pseudoaneurysm at King Hussein Medical Center / Vascular unit between February 2009 and March 2010 was conducted. Fifteen patients were males and 6 were females with mean age of 62 years. Eight patients had diagnostic catheterization while 13 had interventional cardiac procedures. All patients were diagnosed using Duplex scan and were treated with compression. Analysis of the results, efficacy and safety of the ultrasound guided compression treatment modality were discussed.
Results: Successful pseudoaneurysm compression was obtained in 16 patients (76%) whereas 5 patients failed compression and underwent surgical repair. Pseudoaneurysm size ranged between 2.0 -4.5 cm. The mean compression time to accomplish closure was 25 minutes. Two patients required more than one session to get a successful result. Pseudoaneurysm involved the common femoral artery in 8 patients while in 13 patients the origin was distal to the femoral artery bifurcation.
All patients were followed up one week after successful compression procedure by a new Duplex scan with no recurrence of pseudoaneurysm and no arterial or venous complications were reported.
Conclusion:Ultrasound guided compression for the treatment of post catheterization pseudoaneurysm is an effective alternative to surgical repair. It is non invasive and safe modality with high success rate and low complications. It should be considered as a first line of management of uncomplicated femoral pseudoaneurysms.
Key words: Catheterization, Pseudo aneurysm, Ultrasound compression.
JRMS June 2011; 18(2): 11-16
Introduction
The common femoral artery is the primary access site for a wide range of cardiac procedures and is considered to be ideal because of its relative large size and compressibility.(1,2) Femoral artery pseudoaneurysm is an uncommon but well recognized complication of femoral artery catheterization.(3,4) The increasing use of minimally invasive techniques in the form of diagnostic and interventional catheterization procedures has meant that vascular complications from these procedures are seen more frequently.(1,2) Studies documented significant increase in the occurrence of pseudo aneurysm from 0.2 % of diagnostic to 9.0 % of interventional procedures.(1,4,5,6) A pseudo aneurysm forms when blood flows outside the arterial lumen from the puncture site that fails to seal and dissects into the surrounding tissue to form a sac connected to the femoral artery by a neck.(1,2) Symptoms of pseudoaneurysm include groin pain, bruising, palpable mass, bruit and occasionally drop in hematocrit with retroperitoneal hematoma in high punctures.(4) Rupture of a pseudoaneurysm is a life threatening complication whilst compression of the neurovascular structures may result in neuropathy, deep vein thrombosis and limb ischemia.(4,5) Femoral artery pseudoaneurysm has been treated by a variety of means. Traditionally, open surgery was the standard treatment until early nineties.(4,7,8) Less invasive modalities including ultrasound guided compression, percutaneous thrombin injection and transcutanous coil embolization and stenting have been accepted as an alternative and first line treatment.(7,8) In this study, we present our experience on ultrasound guided compression as an efficient and safe modality of treating femoral artery pseudo aneurysm.
Methods
A retrospective review of patients’ records with post cardiac catheterization pseudo aneurysm at King Hussein Medical Center between February 2009 and March 2010 who were referred to the vascular unit for treatment was conducted.
During this period, a total of 8223 cardiac catheterization procedures were performed (4786 diagnostic and 3437 interventional).Twenty one patients (0.25%) referred with femoral pseudoaneurysm were included in the study, fifteen males (71%) and 6 females (29%).Their mean age was 62 years (45 – 72 yrs). Eight patients underwent diagnostic catheterization while 13 had interventional procedures for cardiac disease. All were performed through right femoral artery. Catheter size ranged from 6F – 8F. Post procedure hemostasis was achieved by manual compression for 20 minutes and patients were kept in bed for 6 hours. Seven patients were inpatients while 14 were detected as outpatients /cardiology clinic during follow up visits.
All the patients were evaluated by their cardiologist for typical signs of post catheterization pseudo aneurysm. Patients with bruit, hematoma, pulsatile mass and pain at the puncture site were submitted on the same day for an initial ultrasound imaging to detect the presence of pseudo aneurysm or other complications related to the puncture site. Patients were referred to the vascular unit for further management afterwards.
All patients were on antiplatlets therapy; 21 on aspirin and 4 had clopidogril as well. One patient was on warfain for previously replaced cardiac valve. Sixteen patients had controlled hypertension, 14 were diabetic and 12 were smokers. None of the patients’ medication was stopped during compression therapy.
On arrival to the vascular unit laboratory, patients were re examined with ultrasound B mode imaging combined with color and pulsed Doppler using 5.0 – 7.5 MHz linear –array and curved linear- array transducers. Study included evaluation of flow in distal external iliac vessels and femoral vessels with particular attention to exclude the presence of an associated arterio-venous fistula or deep vein thrombosis (Fig. 1). Ultrasound criteria applied to diagnose pseudo aneurysm were the typical swirling pattern of flow within the pseudo aneurysm lumen and hemodynamicly the ‘’to and fro ‘’ pattern in the neck with antegrade flow entering the pseudo aneurysm during systole and retrograde flow during diastole.(4,5,9,10) (Fig. 2). Evaluation of pseudo aneurysm anatomic features including sac size, shape and neck diameter were noted.
Ultrasound guided compression therapy was the first line of treatment for all our patients’ pseudoaneurysms. Analysis of the results, efficacy and safety of the procedure were discussed.
Ultrasound guided compression technique Pseudo aneurysm compression was carried out using the technique described by Fellmeth et al in 1991.(10-13)
The pulses and Ankle Brachial Pressure Index (ABPI) were documented pre and post procedure.
The arterial lumen and the pseudo aneurysm neck are localized using color duplex scan. Enough pressure to the neck is applied to preclude flow into the aneurysm but maintain flow into femoral artery checked frequently by duplex while applying pressure by the transducers (5.0 – 7.5 MHz linear –array and curved linear- array transducers, SIEMENS, ACUSON CV70). Manual compression for 10 -20 minutes periods was applied after which the pressure is slowly released and pseudo aneurysm is re examined for patency, to reposition transducer or change operator. Compression was reapplied until pseudo aneurysm thrombose; the patient refuses further treatment, operator fatigue or no progression despite repeated adequate compression. After successful thrombosis of the aneurysm, the artery and vein were restudied to exclude subsequent thrombosis (Fig. 3). Intravenous morphine 3mg was given to patients who experienced significant pain during the procedure and all patients were sent home with a prescription of paracetamol tablets. In-patients were kept supine for 6 hours while out-patients were reviewed in 3 hours of complete bed rest and then discharged with the advice of avoiding vigorous exercise.
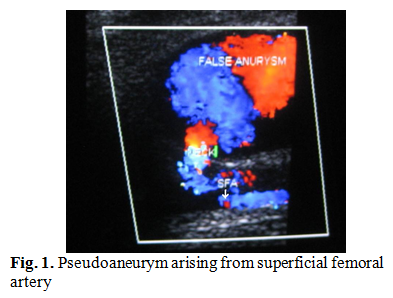
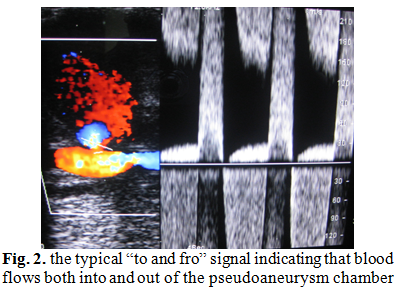
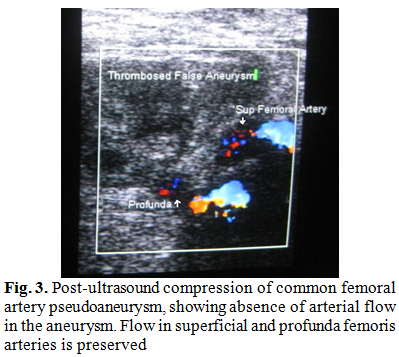
Table I: Pseudo aneurysm size in the reviewed patients
|
Pseudo
aneurysm size
|
No of Patients
|
|
2
- 2.5
|
2
|
|
2.5
– 3.0
|
8
|
|
3.0
– 3.5
|
6
|
|
Ø 3.5
|
5
|
Results
During the study period, successful pseudo aneurysm compression was obtained in 16/21 patients (76 %) whereas compression failed in 5 patients and those were treated by surgical approach.
Twenty patients had pseudo aneurysm with one cavity while one patient had multi compartmental aneurysm that was successfully obliterated by compression.
The time interval between arterial injury and the diagnosis ranged between 3 days – 2 weeks.
Pseudo aneurysm size ranged between 2.0 – 4.5cm Table I. The mean time to achieve closure was 25 minutes (20–80min). Two patients required 2 sessions to get a successful result. In one patient who had partial thrombosis in his first compression session, was found to have completely thrombosed pseudo aneurysm at his follow up visit one week later.
Pseudo aneurysms involved common femoral artery in 8 patients, superficial femoral artery in 8 patients whereas the origin was profunda femoris artery in 5 patients.
In the unsuccessfully treated group (5/21), all patients were referred for surgical repair. One patient (1/5) was an in-patient and had his surgery performed during the same admission while the rest were scheduled on outpatient basis. In one of the patients, compression was too painful to tolerate so the procedure was aborted and surgery was advised. Two patients were on both aspirin and clopidogril on presentation. The aneurysm size was 2.5 – 3.0cm in 4 patients while one patient had a 4.0cm aneurysm. The artery of origin was profunda femoris in 3 patients.
At the end of each compression session, patients’ arteries and veins were checked by ultrasound as well as pulses status. No complications were reported as a result of the procedure.
All patients were followed up after successful thrombosis of the pseudo aneurysms by one week time by means of a new scan, pulse assessment and ankle brachial pressure index that showed complete obliteration of pseudo aneurysm and no clinical complications or recurrence.
Discussion
The growing number of diagnostic and therapeutic interventions performed in the dynamically developing invasive cardiology procedures has been associated with increase in the occurrence of post arterial cannulation complications, frequently in the term of femoral artery pseudoaneurysm.(5,14 )
Pseudo aneurysm diagnosis can be achieved using Doppler ultrasound, angiography, CT, MRI and even scintigraghy.(2,4,5) Angiography requires a new puncture site to confirm diagnosis. CT and MR angiography can be helpful in doubtful cases with difficult anatomy or when the pseudoaneurysm arises from above the inguinal ligament. Contrast administration is required in these three investigations. Numerous studies have shown the sensitivity and specificity of sonography and Doppler in diagnosing pseudoaneurysm as 94% and 97% respectively, making this modality as the standard procedure for diagnosing femoral artery pseudoaneurysm.(2,4,15) In our study, we used Doppler ultrasound as the mainstay for diagnosing pseudoaneurysm using the typical ‘‘to and fro’’ Doppler wave form as a distinctive feature of pseudoaneurysm.(3,16,17)
A variety of therapeutic strategies have been described to treat post catheterization pseudoaneurysms.(1,7,8,9,18) These included surgical repair, ultrasound guided compression, thrombin injection and transcutaneous coiling and stenting.(5,15)
Traditionally, surgery was the standard modality of treatment. Currently, it is indicated in cases of rapidly expanding or actively bleeding pseudoaneurysm, when the femoral neurovascular bundle is compressed resulting in distal ischemia or neuropathy and in infected pseudoaneurysm with overlying skin necrosis.(4,5,15) In our review,5 patients needed surgery mainly due to failure of compression rather than having a definite indication for surgery. All these patients had uneventful surgical repair.
Ultrasound guided percutaneous injection of thrombin has been described by Cope and Zeit in 1986 with high success rates been reported.(17,18) Although compression is cost effective and less invasive, thrombin injection has become the modality of choice of treating femoral pseudoaneurysm in some centers.(6,9) Thrombin is an active form of factor II (prothrombin).It transforms inactive fibrinogen to its active form, fibrin, which subsequently contributes to thrombus formation. Human thrombin as well as bovine thrombin have been used for injection therapy with the latter having a small risk of allergic reactionsThrombin most feared complication is arterial thrombosis and distal embolization. This makes pseudoaneurysms with short and wide neck at relatively higher risk and choosing an alternative technique may be more suitable.(5,8) high success rates (ranging from 91% to 100%), low complication rates, ease of performance, short procedure times, and no radiation exposure favor the use of US-guided thrombin.(4,5,6)
Ultrasound guided compression obliteration of pseudoaneurysm has been shown to be safe and effective method for repair of femoral artery pseudoaneurysm and has become the primary modality at many institutes.(3,10) We adopted this technique as the first line of treatment in all our patients with femoral artery pseudoaneurysms. It is non invasive, accurate and cost effective. We achieved a success rate of (76%) which is comparable to other studies.( 1,14,15,18 )
Conversely, compression therapy may have some drawbacks. It is time consuming, painful and demanding manpower as it may take more than one hour on some occasions making it difficult for both the patient and operator to tolerate .Some reviews described the use of conscious sedation and local anesthesia to create as comfortable as possible situation.(5,12,18) Even so, some patients cannot tolerate the procedure. In one of our patients the procedure was converted into open repair because of unbearable pain and anxiety.
Ultrasound compression can be seriously complicated by pseudoaneurysm rupture, arterial occlusion and distal embolization requiring urgent transfer to operating theatre.(4) None of these complications was reported in any of the patients in our review.
The published literature has identified several factors that may be responsible for a higher risk for developing post catheterization complications. These includes: old age, female gender, catheter size, anticoagulation and complexity of pseudo aneurysm.(2,3,11,17) In our study, the majority of patients were males (71%). The catheter size ranged from 6F in diagnostic to 8F in therapeutic cases. One patient was on regular anticoagulation (warfarin) and had a successful compression while 2 of the 5 patients (40 %) who failed compression were on both aspirin and clopidogril. One pseudoaneurysm was multilobulated and resulted in successful obliteration by compression. Reviewing the mentioned data, we noticed one drawback to our review is that the study sample is small to allow statistical analysis of risk factors for the development of pseudoaneurysm.
Proper puncture technique as shown by other studies in an effort to prevent formation of pseudoaneurysm has been described.(1,2,9) Correct puncture site selection ,avoiding multiple punctures with posterior wall injury, using smaller sheath and proper post procedure haemostatic compression were noticed to help in reducing puncture complications. We noted that the greater part of our patients (13/21) had their puncture sites beyond the common femoral artery bifurcation which makes successful compression of arterial hole a harder goal to achieve.(4) This has been yet clearly demonstrated in our group that failed compression as profunda femoris artery was the origin of pseudoaneurysms in 3/5 of the patients. Compression of this artery branches is usually difficult as they are not opposing a bone or covered by the femoral sheath.(11)
While spontaneous thrombosis of small pseudoaneurysms (< 2.5cm) of femoral artery was reported in some studies, we noticed spontaneous thrombosis in one of our patients on his second visit for another session of compression therapy.(4,6,17) We believe that these patients usually need close observation and follow up during the observation period.
Compression therapy has been demonstrated to be a safe and cost-effective method for achieving thrombosis of femoral pseudoaneurysm. limitations include patient’s intolerance and the operator’s capability to sustain adequate pressure.(1,3,7) According to our experience, we think that compression therapy shows favorable results in uncomplicated small pseudoaneurysms (< 3.0 cm) having a narrow neck and a visible point of origin from the femoral artery.
The limited evidence base appears to support the use of thrombin injection as an effective treatment for femoral pseudoaneurysm.(19) We believe that practical approach may be to use compression as first-line treatment, reserving thrombin injection for those in whom the compression procedure fails.
Conclusion
Therapeutic options for pseudoaneurysm repair have evolved in recent years from the traditional surgical option towards less invasive approaches. Ultrasound guided compression is a safe alternative with high success rate and low complications in treating pseudoaneurysms. It is effective inexpensive method and should be considered as the first therapeutic modality for the management of uncomplicated simple post catheterization femoral pseudoaneurysms.
References
1.Ahmad F, Turner SA, Torrie P, et al. Iatrogenic femoral artery pseudoaneurysms. A review of current methods of diagnosis and treatment. Clinical Radiology 2008; 63:1310-1316.
2.Ates M, Sahin S, Konuralp C, et al. Evaluation of risk factors associated with femoral pseudoaneurysms after cardiac catheterization. J Vasc Surg 2006; 43:520-4.
3.Eisenberg L, EK Paulson, MA Kliewer, et al. Sonographically guided compression repair of pseudoaneurysms: Further experience from a single institution. AJR Am J Roentgenol 1999 Dec; 179):1567-1573.
4.Middleton WD, Dasyam A, Teefey SA. Diagnosis and treatment of iatrogenic femoral artery pseudoaneurysms. Ultrasound Quarterly 2005; 21:3-17.
5.Heis HA, Bani Hani EK, Elheis MA, et al. Post-catheterization femoral artery pseudoaneurysms: therapeutic options. A case-controlled study. Int J Surg 2008 Jun; 6(3):214-9.
6.Schneider C, Malisius R, Kuchler R, et al. A prospective study on ultrasound guided percutaneous thrombin injection for treatment of iatrogenic post catheterization femoral pseudoaneurysms. Int J Cardiology 2009; 131:356-361.
7.Paschalidis M, Theiss W, Kolling K et al. Randomized comparison of manual compression repair versus ultrasound guided compression repair of postcatheterisation femoral pseudoaneurysms. Heart 2006; 92:251-252.
8.Bloom AI. Iatrogenic femoral pseudoaneurysms. Radiology 2002; 222 (1):292-293.
9.Stone PA, AbuRahma AF, Flaherty SK, et al. Femoral pseudoaneurysms. Vasc Endovasc Surg 2006; 40:109-117.
10.Yerli H, Yucel C, Ozdemir M, et al. US-Guided Compression repair in iatrogenic pseudoaneurysm. Medical Journal 2004; 15: 87-95.
11.Knight CG, Healy DA, Thomas RL. Femoral artery pseudoaneurysms. Risk factors, prevalence, and treatment options. Ann Vasc Surg 2003; 17:503-508.
12.Fellmeth BD, Roberts AC, Bookstein JJ, et al. Postangiographic femoral artery injuries: nonsurgical repair with US guided compression. Radiology 1991; 178:671-675.
13.Coley BD, Roberts AC, Fellmeth BD, et al. Postangiographic femoral artery pseudoaneurysms: further experience with US guided compression repair. Radiology 1995; 194:307-311.
14.Dean SM, Olin JW, Piedmonte M, et al. Ultrasound guided compression closure of postcatheterization pseudoaneurysms during concurrent anticoagulation: A review of seventy seven patients. J Vasc Surg 1996; 23: 28-35.
15.Demirbas O, Guven A, Batyraliev T. Management of 28 consecutive iatrogenic femoral pseudoaneurysms with ultrasound guided compression. Heart Vessels 2005; 20:91-94.
16.Zweibel W. Introduction to vascular sonography, 5th edition. WB saunders. 2005 p 391-395.
17.Webber GW, Jang J, Gustavson S, et al. Contemporary Management of Postcatheterization Pseudoaneurysm. Circulation. 2007; 115:2666-2674.
18.Luedde M, Krumsdorf U, Zehelein J, et al. Treatment of iatrogenic femoral pseudoaneurysm by ultrasound guided compression therapy and thrombin injection. Angiology 2007; 58: 435-439.
19.Tisi PV, Callman MJ. Treatment for femoral pseudoaneurysms. Cochrane Database of Systematic Reviews 2009, Issue 2.