Abstract
Objectives: To evaluate the use of the buccal fat pad in closure of oroantral
communications.
Methods: Fifty three patients with different sizes of oroantral fistulas
were treated with a pedicled buccal fat pad to close these defects between 2003
and 2008, with minimal follow up of two months. The age, sex, and etiology were
recorded.
Results: Fifty three patients (34 males and 19 females) were treated,
ranging age from 17 to 73 years. The reasons of the oroantral communication
were due to dental extraction of upper premolars, molars, excision of cystic
lesions, implant removal and different kinds of tumors. The procedure was successful among 52
patients. Postoperatively, the orally exposed fat gradually was transformed
into a granulation-like tissue and epithelization developed within 3 weeks.
Conclusions: Use of the buccal fat pad is a safe and easy method to be used in
oroantral communications closure and the procedure has wide applications and a
high degree of success. Good vascularization, ease of access, and minimal donor
site morbidity make it a reliable soft tissue graft.
Key words: Buccal
fat pad, Fistula, Oroantral.
JRMS June 2011; 18(2): 26-31
Introduction
Oroantral Fistula
(OAF) can be defined as a pathologic communication between oral cavity and maxillary
sinus and is usually located between the antrum and vestibule. The oroantral
communication is a term includes the oroantral fistula in addition to any
communication more than 10 mm in diameter which might result from more
extensive procedures like bullet injury and maxillectomy surgeries.(1,2)
Oroantral
fistulas most commonly arise because of tooth extraction, mostly follows
removal of the maxillary first molars because there is, anatomically, a close
relationship between the root apices of these teeth and the antrum. OAF usually
heal within 2 to 3 weeks if less than 2 mm in diameter, but when there is more
than a 3-mm defect, or there is sinusitis or periodontal disease, the opening
often persists.(2) After 3 weeks, they are accepted as
chronic, spontaneous healing is uncommon, and surgical correction is necessary.
Although the surgical closure is successful in more than 95% of cases,
inappropriate operation will result in closure failure.(2-5)
Table I. Distribution
of causes of oroantral fistula
|
Cause
|
Frequency (%)
|
|
Extraction of max. 1st molar
|
15 (28.3.)
|
|
Extraction of max. 2nd
molar
|
11 (20.8)
|
|
Extraction of max. 3rd molar
|
3 (5.7)
|
|
Extraction of max. 1st
premolar
|
1 (1.9)
|
|
Extraction of max. 2nd
premolar
|
8 (15.1)
|
|
Excision of tumor
|
6 (11.3)
|
|
Implant removal
|
5 (9.4)
|
|
Enucleation of cystic
lesion
|
4 (7.5)
|
|
Total
|
53 (100)
|
Variable methods for the
closure of OAF
have been reported
in the literature, most of them based on mobilizing the buccal sliding flap and
palatal flap tissue and advancing the resultant flap into the defect. However,
these procedures have not always provided satisfactory results.(5)
Numerous modifications of existing techniques were recommended for soft tissue
closure of the fistulas. A pedicled graft of the buccal fat pad (BFP), which
enables the closure of oral defects even up to an area of 60 × 50 mm and a
thickness of 6 mm, has often been used for the reconstructions of intraoral defects
since the procedure was first introduced by Egyedi.(4,6-8)
The buccal fat
pad is different from other subcutaneous fat tissue and can easily be used in
some intraoral operative procedures. It can be used as a pedicled graft for
coverage of intraoral defects such as seen after ablative surgery or in case of
oroantral fistulas.(6, 7) Tideman et al.
reported that the epithelialization of this uncovered BFP graft takes place
readily within 2 to 3 weeks.(9)
For a long
time the only surgical importance of this structure seemed to be herniation
into the oral cavity or into the maxillary sinus in association with facial
trauma.(10) Only in the last quarter of
this century has the buccal fat pad been used as a grafting source. In 1977,
Egyedi reported the use of the buccal
fat pad as a pedicled graft in closing oronasal fistula. Neder, in 1983, was
the first to describe the use of the buccal fat pad as a free graft for
intraoral defects.(7,11,12)
In this
study we tried to evaluate our experience in the use of the buccal fat pad in
closure of oroantral communication.
Methods
Between July 2003 and November 2008, the
buccal fat pad was used to close oroantral fistula among 53 patients at Prince Hashem
Bin Al-Hussein
Hospital, Queen
Alia Military
Hospital, Princess
Haya Bint
Al-Hussein Hospitals,
Prince Ali
Bin Al-Hussein
Hospital and King Hussein
Medical Center, age ranged from 17 to 73 years, there were 34
males (64%) and 19 females (36%). All surgical procedures were performed by the
authors themselves throughout there periodic rotation on the previously
mentioned hospitals.
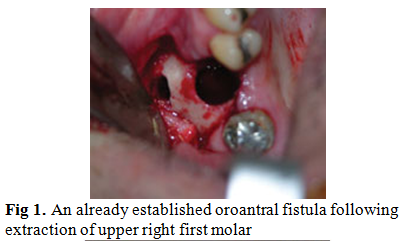
All of the patients presented with
established oroantral fistulas i.e. the time of injury more than three weeks in
cases of dental extraction. In cases of surgical defects due to tumor
resection, cyst enucleation, and implant removal immediate closure was considered,
the minimal follow up period was two months postoperatively. The factors
considered were sex, age, cause of the OAF, and time of injury.
Preoperative antibiotics were used to
eliminate infection and for all cases intraoperative antibiotics were administered.
Caldwell-luc operation was performed when necessary (to remove tooth remnants
or foreign bodies).
The
surgical technique:
After
inducing local anesthesia (mepivicain 2% with 1:80,000 adrenaline), a circular
incision with a 3-mm margin was made around the OAF, and the epithelial tract
and any inflammatory tissue within the opening were completely excised. Two
divergent cuts were then made from each end of the circular incision extending
into the vestibule. The trapezoidal buccal mucoperiosteal flap was then
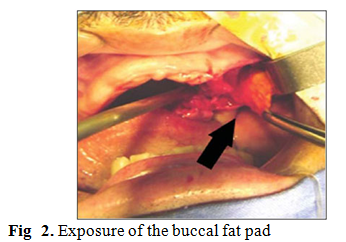
reflected from the alveolar process and the lateral wall of the maxilla. The
BFP was exposed through a 1-cm-long vertical incision in the reflected
periosteum posterior to the zygomatic buttress. In some tumor cases, the buccal
fat pad was already visible through the wide exposure and prolapsed into the
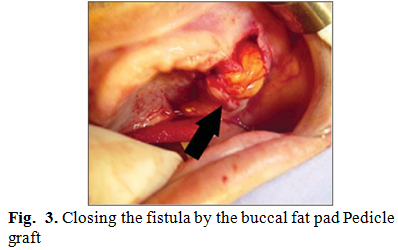
defect. The BFP was gently advanced into the bony defect and secured to the
palatal mucosa without tension with 4-0 vicryl sutures (Fig. 1, 2, 3). Finally,
the mucoperiosteal flap was replaced in its original position, and sutures were
inserted between the BFP and the buccal flap so that part of the BFP was
exposed in the oral cavity and finally a stabilizing suture was placed between
buccal flap and palatal mucosa. No surgical splint or dressings were used.
Furthermore, the patient should be motivated to avoid intraoral negative
pressure such as blowing the nose and to use antibiotics for prophylaxis
(amoxycillin 500mg three times a day for 5 days).
Results
Out of the
53 patients there were 34 males (64%) and 19 females (36%), with an average age
of 38 years, ranging from 17 to 73 years. Nine patients had hypertension, 7
diabetes mellitus, 3 hypertension and diabetes mellitus concomitantly, 5
cardiopathy, 2 asthma.
The
interval from fistula development to repair varied from immediately in the same
session to 2 years. In cases of tumor resection immediate reconstruction was performed
in 3 cases of maxillary eosinophilic granuloma, two cases of maxillary squamous
cell carcinoma, and another one of osteogenic sarcoma. The same was applied for
patients with cystic lesions and faulty endosseous implants where immediate
repair of OAF was possible at time of initial surgical management.
Thirty
eight cases of OAF out of the 53 (71.7%) developed after removal of one of the
maxillary teeth. The remaining 15 cases were caused by excision of tumor (6
cases), implant removal (5 cases), and enucleation of cystic lesions (4 cases).
The detailed distribution of causes is stated in (Table I). The size of the oroantral defects ranged
from 3 to 20 mm in diameter.
The most
frequent symptoms that patients suffered were those of acute sinusitis including
fever, fatigue and malaise, and pain that increased upon bending forward. Five
patients with acute sinusitis also had swelling of the periorbital tissues, and
all 29 had a purulent discharge from the fistula. An isolated discharge and
fluids leak through the nose was seen in 9 patients. Also, phonetic changes
were observed in most of these patients. History of traumatic extraction was
reported in 6 patients were in four of them a root fragments were retrieved
from the antrum.
In five
patients a complicated implant procedures which were performed in private
clinics the associated peri-implant infection and faulty prosthesis where the
main symptoms among them. On the other hand an intraoral swelling was the
complaint of three patients two of them proved to have huge cystic lesions
related to necrotic and endodontically treated maxillary first molar, and the
last one the histopathological study revealed osteogenic sarcoma of the edentulous
maxilla. In two patients a persistent ulcer was the main complaint they have
squamous cell carcinoma. A severe periodontal destruction was seen in three
eosinophilic granuloma patients. An accidentally found residual cystic lesion
in two patients who never suffered, but a preprosthetic preparation of the
maxilla by extracting multiple chronically infected roots but in the panoramic
x-ray revealed the cystic lesions.
Not all
the cases were fresh that is to say in 8 patients a failed OAF closure was
attempted somewhere else. The dentist made several treatment trials before
referring the patient to the maxillofacial surgeon. This fact accounted for the
delay in diagnosis in such cases.
29 of these
patients also had been suffering from acute sinusitis which in 20 of them was
treated preoperatively with oral amoxicillin 500 mg three times daily, for one
week combined with antral irrigations with normal saline. Postoperatively, oral
500 mg Amoxycillin three times daily for one week
In 9 cases
of maxillary sinus pathology, a Caldwell-Luc operation was performed, which
included sinus polyposis excision and inferior meatal nasal antrostomy. The
sinus is then packed gently with medicated ribbon gauze which is removed after
48 hours. All our patients who underwent a Caldwell-luc operation received intraoperative and postoperative
antimicrobial treatment with intravenous amoxicillin 1g three times daily in addition to oral metronidazole 250 mg
two times daily for 5 days, and oral 500
mg two times daily for one week..
Twenty two
patients were operated on under local anaesthesia which was applied to the
palatal and buccal sides of the upper jaw, while in 31 patients general
anesthesia was necessary.
Clinically,
in the typical course, the surface of the orally exposed fat became
yellowish-white and then gradually became red within one week, which was likely
due to the formation of young granulation tissue. This changed into a firmer
granulation tissue during the second week, and it became completely
epithelized, with a slight contraction of the wound, by 3 weeks
postoperatively. No local infections were noticed.
The BFP
failed in a residual pin point fistula just in one case, where it was employed
to repair an oroantral communication near to the first maxillary premolar.
Dealing with complications, we detected a partial necrosis of the flap in 2 of
the 53 cases, with no clinical deficits, achieving a complete epithelization
later. A total necrosis was not discovered.
Discussion
Surgical
repair of the oroantral fistula is one of the more challenging problems
confronting the surgeon working in the maxillofacial region. The multiple
techniques described in the literature over the last 50 years point to the lack
of consensus for a uniformly successful procedure.(9)
An
oroantral fistula may arise secondary to dental infection, osteomyelitis, the
sequellae of radiation therapy, trauma, or the removal of maxillary cysts or
tumors.(13) The
extraction of maxillary posterior teeth is the most common etiology of the
oroantral fistula because of the proximity of the apices of the bicuspids and
molars to the antrum, and the thinness of the antral floor (ranging from 1 to 7
mm). A fistula develops when the apices of upper teeth and the lining of the
maxillary sinus are closely related. This is rarely the result of pathologic
change, such as associated infection or cyst formation.(14)
Most small
acute oroantral communications, 1 to 2 mm in diameter, heal spontaneously in the
absence of sinus infection. However, almost all oroantral defects larger than 5
mm and present for longer than 3 weeks will epithelialize into chronic
oroantral fistulas requiring secondary surgical closure.
Treatment
modalities to repair the oroantral fistula include local or distant soft tissue
flaps, with or without autogenous grafts or alloplastic implants.(15)
Immediate repairs of the acute oroantral defect have a uniformly high success
rate approaching 95%, but the success rate of secondary closure of the chronic
oroantral fistula is reported to be as low as 67%. Two principles must be observed at time of OAF closure,
first, the sinus must be rendered free of infection, and secondly a tension
free well vascularized flap is used.(15-17,
21) The BFP is the anterior
extension of the masticatory fat pad which fills the space between the
masticatory muscles. It has gained considerable importance during the past two
decades. Apart from its importance as a donor site for free-fat grafting or a
pedicle fat flap, it is also important in facial contouring in cosmetic surgery.
The size of the BFP, is fairly constant among different individuals
regardless of the overall body weight and fat distribution.(9,22- 24)
Several
reports have shown that the BFP can be used safely in the closure of OAF after
tooth removal.(7,25-27) Tideman
et al. reported that the epithelialization of this uncovered BFP graft
takes place readily within 2 to 3 weeks.(9)
In this
study, the frequency of occurrence of OAF was nearly the double in males than
in females 64% to 36% respectively, which differs from that found in other
studies,(28-30) and agrees
with what had been found by others.(2,31)
However, according to Lin and Bukachaevsky, females exhibit larger sinuses than
males and should, therefore, be at greater risk of OAF.(32)
Our
results are consistent with results in the literature regarding the most
frequent cause which was dental extraction.(5,28,30)
The OAFs in this study mostly occurred after extraction of the first and second
molars, a finding which agrees with other reports.(1,28,33) While
in other studies the extraction of the second premolar was the most causative
factor followed by the first molar.(5)
The
drainage and adequate aeration of the sinus should be achieved in cases with
mucosal thickening and cystic or polypoid degeneration of mucosa.(1,13,32) Our
results were concordant with the literature. According to Del Junco et al and
Bluestone, a nasoantral window is essential for drainage, whereas equally good
results were achieved by treating sinus pathology with antibiotics and without
drainage of the maxillary sinus into the nose. Bluestone reports that no surgical procedure is
needed when the maxillary sinus is free of disease.(34-36)
The easy
mobilization of the buccal fat pad and its excellent blood supply and minimal
donor site morbidity make it an ideal flap. It can be very useful in older
patients to reconstruct defects quickly under local anesthesia. Our results
showed that the BFP is a safe, useful and effective procedure for closure of
oroantral fistulas. In addition, it is useful procedure for reconstruction of
hard palate defects, soft palate defects and coverage of bone augmentation
procedures as recommended by other authors.(37,38)
Conclusions
Use of the
buccal fat pad is a safe and easy method to be used in oroantral fistula
closure and the procedure has wide application and a high degree of success.
Good vascularization, ease of access, and minimal donor site morbidity make it
a reliable soft tissue graft.
The
advantages of this were the simplicity and ease of the technique, the high
success rate, the lack of a visible scar at the donor site, the minimal
discomfort for the patient, and the low rate of complications.
References
1.Amaratunga NA. Oro-antral
fistulae. A study of
clinical, radiological and treatment aspects. Br J Oral Maxillofac Surg 1986;
24:433-437.
2. Yilmaz T, Suslu AE, Gursel B. Treatment of oroantral fistula:
Experience with 27 cases. American Journal of Otolaryngology 2003; 24(4):221-223.
3. Schuchardt K. Treatment of oro-antral perforations and fistulae. Int Dent J
1955; 5:159.
4. Hanazawa Y, Itoh K, Mabashi T, Sato K. Closure of oroantral communications using
a pedicle buccal fat pad graft. J Oral Maxillofac Surg 1995; 53:771-775.
5. Giiven O. A clinical study on oroantral fistulae. Journal of Cranio- maxifacia
Surg 1998; 26: 267-271.
6. Colella G, Tartaro G, Giudice A. The buccal fat pad in oral reconstruction.
The British Association of Plastic Surgeons 2004; 57: 326–329.
7. Egyedi P. Utilization of the buccal fat pad for closure of oro-antral
and/or oronasal communications. J Maxillofac Surg 1977; 5:241-244.
8. Watzak G, Tepper G, Zechner W, Monov G, Busenlechner D, Watzek G. Bony press-fit closure of oro-antral
fistulas: a technique for pre-sinus lift repair and secondary closure. J
Oral Maxillofac Surg 2005; 63:1288-1294.
9. Tideman H, Bosanquet A, Scott J. Use of the buccal fat pad as a pedicled
graft. J Oral Maxillofac Surg 1986; 44:435.
10.
Xiao H, Bayramiçli M, Jackson IT. Volumetric analysis of the buccal fat pad.
Eur J Plast Surg 1999; 22:177-181.
11.
Neder A. Use of buccal fat pad for
grafts. Oral Surg 1983, 55:349.
12.
Hudson JW. Use of pedicled fat pad graft as an
adjunct in the reconstruction of palatal cleft defects. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod 1995; 80:24-27.
13.
Del Junco R, Rappaport I, Allison GR. Persistent oral antral fistulas. Arch
Otolaryngol Head Neck Surg 1988; 114:1315-1316.
14.
Killey HC, Kay LW. An analysis of 250 cases of oro-antral fistula treated by the
buccal flap operation. Oral Surg Oral Med Oral Path 1967; 24: 726.
15.
Brusati R. The use of an osteoperiosteal flap to close oroantral fistulas. J
Oral Maxillofac Surg 1982; 40:250-251.
16.
Yih WY, Merrill RG, Howerton DW. Secondary closure of oroantral and
oronasal fistulas. J Oral Maxillofac Surg 1988; 46:357-364.
17.
Lazow SK. Surgical management of the oroantral fistula: flap
proceduresoperative techniques in otolaryngology. Head and Neck Surgery 1999;
10 (2): 148-152.
18.
Dergin G, Gurler G, Gursoy B. Modified connective tissue flap: A new
approach to closure of an oroantral fistula. Br Jour Oral and Max facial
Surg 2007; 45: 251–252.
19. Awang MN. Closure of oroantral fistula. Int J Oral
Maxillofac Surg 1988; 17:110-115.
20.
Hori M, Tanaka H, Matsumoto M, Matsunaga S. Application of the Interseptal Alveolotomy
for Closing the Oroantral Fistula. J Oral Maxllofac Surg 1995; 53:1392-1396.
21.
Steiner M, Gould AR, Madion DC, et
al. Metal plates
and foils for closure of oroantral fistulae.
J Oral Maxillofac Surg 2008; 66:1551-1555.
22.
Dubin B, Jackson IT, Halim A, et al. Anatomy of the buccal fat pad and its
clinical significance. Plast Reconstr Surg 1989; 83:257.
23.
Stuzin JM, Wagstrom L, Kawamoto HK, et
al. The anatomy
and clinical applications of the buccal fat pad. Plast Reconstr Surg 1990; 85:
29.
24.
Macintosh RB. Fat and dermis grafting in oral and maxillofacial surgery. Oral
Maxillofac Surg Clin North Am 1993; 5: 579.
25. Haas R, Watzak G, Baron M,
et al. A
preliminary study of monocortical bone grafts for oroantral fistula closure. Oral Surg Oral Med Oral
Pathol Oral
Radiol Endod 2003; 96:263-6.
26. Anavi Y, Gal G,
Silfen R, Calderon S. Palatal rotation-advancement flap for delayed
repair of oroantral fistula: A retrospective evaluation of 63 cases. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 2003; 96:527-34.
27.
Hai KH. Repair of palatal defects with unlined buccal fat pad grafts. Oral
Surg Oral Med Oral Path 1988; 65:523.
28.
VonWowern NV. Oroantral communications and displacements of roots into
the maxillary sinus: a follow up of 231 cases. J Oral Surg 1971; 29:622 -627.
29.
Skoglund LA, Pedersen SS, Holst E. Surgical management of 85 perforations to
the maxillary sinus. Int J Oral Surg 1983; 12: 1-5
30.
Punwutikorn A, Waikakul LG, Pairuchvej V. Clinically significant oroantral
communications-a study of incidence and site. Int J Oral Maxillofac Surg
1994; 23:19-21.
31.
Martin-Granizo R, Naval L, Costas A, et al. Use of buccal fat pad to repair intraoral
defects: review of 30 cases. Br J Oral and Max facial Surg 1997; 35:
81-84.
32.
Lin PT, Bukachaevsky R, Blake M. Management of odontogenic sinusitis with
persistent oro-antral fistula. Ear Nose Throat J 1991; 70:488-490.
33.
Ehrl PA. Oroantral communication. Int J Oral Surg 1980, 9: 351-358.
34.
Yalcin S, Aybar B, Haznedaroglu F, Yucel E. Bilateral oroantral fistulas following
devitalization of teeth by arsenic trioxide: a case report. J Endodontics
2003; 29(3):205-207.
35.
Bluestone CD. The management of oroantral fistulas. Otolaryngol Clin North
Am 1971; 4:179-191.
36. Car M, Juretic M. Treatment of oroantral communication
after tooth extraction. Is drainage into the nose necessary or not?. Acta
Otolaryngol 1998; 118:844-846.
37.
Abuabara A, Cortez ALV, Passeri LA, et al. Evaluation of different treatments for
oroantral / oronasal communications: experience of 112 cases. Int J Oral
Maxillofac Surg 2006; 35: 155–158
38.
Baumann A, Ewers R. Application of the buccal fat pad in oral reconstruction. J Oral
Maxillofac Surg 2000; 58: 389-392.