Abstract
Objective: To determine
the common causes of persistent cervical lymphadenopathy in children and to
test a diagnostic approach.
Methods: This study was
conducted at King Hussein Medical Center/pediatric clinic over one year period
to look for all children between ages of 6 months and 14 years with persistent
lymph node enlargement. Persistent enlargement is defined as a lymph node >
1 cm in diameter, and > 2 weeks duration. A management algorithm was
proposed and followed in the management.
Results: One hundred and thirty children presented to
infectious diseases clinic with persistent lymph nodes enlargement. In 70
children (53%) the nodes regressed in 2 weeks time, in another 30 children (23%)
they regressed in 4 weeks time. Fifteen children (12%) had tuberculous lymphadenitis;
10 children (8%) had lymph node abscess; 3 children (2%) had Epstein Barr virus
infection and 2 children (1.5%) had Hodgkin’s lymphoma on initial presentation.
Conclusion: Reactive
lymphadenitis is the commonest cause of cervical lymph node enlargement in
children. Majority of lymph nodes regress in 4 weeks time. Persisting lymph
nodes more than 4 weeks warrant histological examination. Tuberculosis is a
common cause of cervical lymphadenopathy among Jordanian children.
Key words: Lymphadenopathy, Lymph node, Lymphadenitis
JRMS
June 2011; 18(2): 32-35
Introduction
Lymphadenopathy
refers to any disease process involving lymph nodes that are abnormal in size
and consistency. This condition has multiple etiologies, the most common of
which are infection, neoplasia, and autoimmune diseases. Lymphadenitis refers
to lymphadenopathies that are due to inflammatory processes. It is characterized
by nodal swelling, pain, skin changes, fever, edema and/or purulent collection.
In the pediatric age group, most lymphadenopathies are attributable to an
infectious etiology, often viral in origin. Enlarged, palpable lymph nodes are
common due to reactive hyperplasia of the lymphoid tissue.(1)
Cervical
lymphadenitis is a common pediatric problem, and most patients with this
condition are treated successfully by their primary care physicians. Histological
examination and surgical consultation are, however, often required to assist in
the diagnosis and treatment of patients who do not respond to initial therapy
or in whom there is an index of suspicion for a neoplastic process.(2)
Despite the frequency of the problem in children, few original studies on the
issue are recent. Most of the studies were conducted to define the causative
agents.
The
aim of this study was to determine the most common causes of persistent cervical
lymphadenopathy and the management strategy based on clinical, laboratory,
ultrasonic and histological findings.
Method
This
study was conducted over one year period from January 2008 to December 2008 at
King Hussein Medical Center/pediatric clinic to evaluate children with
persistent lymphadenopathy.
Persistent lymphadenopathy was defined as
enlarged lymph nodes (> 10 mm in diameter) and persisting for more than 2 weeks.
The
study included all children who were referred from the general pediatric clinic
to the infectious disease clinic with the diagnosis of persistent
lymphadenopathy. Age, gender, and accompanying diseases of the patients were
assessed.
Initial work up of all patients included: detailed physical
exam, complete blood count, blood film, erythrocyte
sedimentation rate
(ESR), purified protein derivative (PPD), chest X ray (CXR) and ultrasonic examination; viral studies for cytomegalovirus (CMV) and Epstein
Barr virus (EBV);
and histological testing by fine needle
aspirate (FNA) or excision were preserved for cases with abnormal findings (abnormal
white blood cells (WBC) count; abnormal blood
film; high ESR > 20 ml/hr; PPD > 10 mm ) Diagram 1.
|
Persistent
lymphadenopathy
- 1cm in
diameter
- 2 wks duration
. Physical examination
. CBC, Blood film, ESR, PPD, CXR
. U/S
|
|
Normal
↓
Observe for 2 wks
↓
Regressing
|
Abnormal
↓
Histological examination
( FNA, excision )
Viral studies
|
|
Persistent or increasing in
size
|
|
Histological examination
Viral study
|
|
CBC: Complete Blood Count; U/S: Ultrasound
|
Diagram 1. Suggested management
algorithm for children with persistent lymphadenopathy
Results
One
hundred thirty children between the ages of 6 months and 14 yrs were referred to
the infectious disease clinic during the specified period of time. All had
persistent lymph node enlargement based on our previous definition. Seventy
five children (58%) had unilateral cervical lymph node enlargement, while in 55
children (42%) the pathology was bilateral. There was no sex difference.
The
jugulodigastric and the submandibular lymph nodes were the two most common
enlarged nodes in 80% of children. Submental
and anterior cervical accounted for the rest of the pathology (20%). After following the suggested algorithm in the management, we
found that in 70 children ( 53%) the lymph nodes regressed in size over 2 weeks
time and in 30 children (23%) they
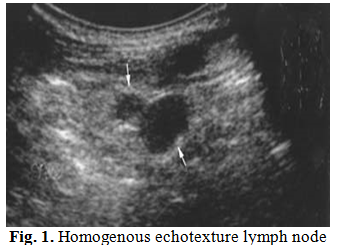
regressed in 4 weeks time as proved by ultrasonic examination. The FNA showed reactive lymphoid hyperplasia
in these 30 children. All of these children had tender, mobile, and soft nodes
on clinical examination. In all of them complete blood count, blood film, ESR
and CXRs were normal. Ultrasound showed enlarged lymph nodes with homogenous
echotexture in all of them Fig.1. Fever was the commonest
systemic manifestation in these children (77%). Of the remaining 30 children,
10 children (5%) had lymph node abscess on initial presentation based on clinical
and ultrasonic findings, surgical excision was done for them and histological testing
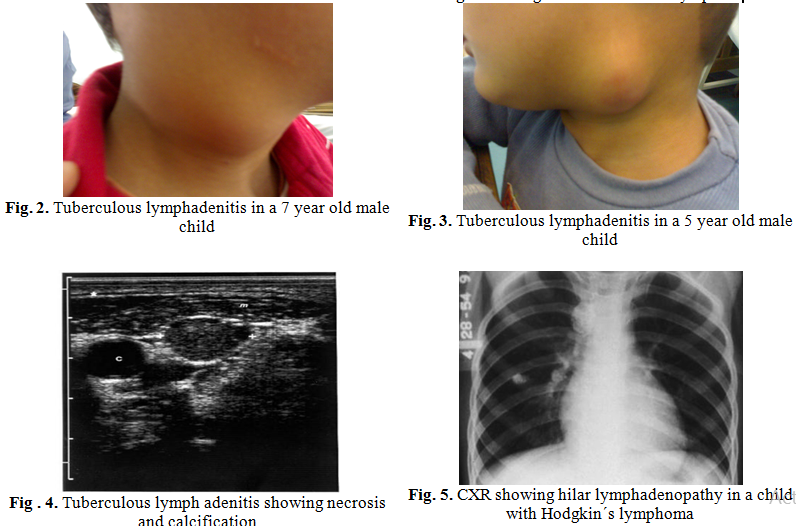
confirmed the diagnosis; tuberculous lymphadenitis was diagnosed in 15 children
(12%) based on clinical, PPD testing (> 10 mm in diameter) and caseating
granuloma on lymph node histology Fig. 2, 3. The ultrasound showed a non-homogenous
echotexture with necrotic shadows and areas of calcification Fig. 4. Three
children (2%) with bilateral lymph node enlargement and splenomegaly had
Epstein Barr virus (EBV) proved by polymerase
chain reaction (PCR);
and two children (1.5%) who had bilateral
firm, nonte`21``212nder lymph node enlargement had Hodgkin´s lymphoma on
excisional biopsy. These two children had high ESR on initial presentation, and
their CxR’s showed widened mediastinum with hilar adenopathy Fig. 5. Table I
summarizes the results.
Discussion
Cervical
lymphadenopathy is a common presentation in children in both the primary care
and hospital setting. Park states that 90% of children aged 4-8 yrs have
palpable cervical lymph nodes.(3)
Table I. Diagnosis of persistent
lymphadenopathy in 130 children
|
Diagnosis
|
Number
|
%
|
|
Reactive hyperplasia regressed
in 2 wks time
|
70
|
53
|
|
Reactive hyperplasia
regressed in 4 wks time
|
30
|
23
|
|
Lymph node abscess
|
10
|
5
|
|
Tuberculous
lymphadenitis
|
15
|
12
|
|
EBV infection
|
3
|
3
|
|
Hodgkin´s lymphoma
|
2
|
1.5
|
|
Total
|
130
|
|
According
to Larsson et al 38- 45% of otherwise healthy children have palpable cervical
lymph nodes.(4)
The
differential diagnosis of a persistent neck lump in children is different from
adults because of increased incidence of congenital anomalies and infectious
diseases and rarity of malignant disorder. In our study we excluded congenital
anomalies and limited our research to persistently enlarged lymph nodes. It is
widely accepted that the absence of clinical signs of inflammatory disease,
negative laboratory testing and progressive reduction of size of lymph node
indicate reactive hyperplasia.(5) The study indicates that reactive inflammatory
changes are the commonest pathology in children as confirmed by other studies.
Our observation indicates also that most cases of lymphadenopathy are
self-limited and require no treatment. Failure of resolution after 4 weeks
might be an indication for diagnostic histology. Most researches indicate that
bilateral lymphadenopathy is more likely to be reactive in nature but our study
cannot confirm that because in 58% of children enlargement was unilateral.(6)
Mobility,
softness and tenderness are almost always associated with reactive changes,
which is similar to observation by other researchers.(7) We
found that ultrasound is a valuable
diagnostic tool for showing the size, shape and echotexture of lymph nodes. A
homogenous echotexture, oval shape, central necrosis, blurred margins were
associated with reactive hyperplasia in most cases, while a non-homogenous
echotexture suggests other diagnosis. Nevertheless U/S should not be considered
as a definitive mean to rule out neoplasia in patients with persistent lymphadenopathy.(8)
Conclusion
Enlargement
of cervical lymph nodes is a common problem in children. Reactive hyperplasia
secondary to benign infectious causes is usually the commonest pathology. Most
of these cases regress in 4 weeks time. Persistent lymph nodes more than 4 weeks
warrant histological examination. Tuberculosis is a common cause of cervical
lymph adenopathy among Jordanian children, although no previous studies have
been done on this issue. A management strategy should be established to
diagnose children with persistent lymph node enlargement.
References
1.Luu TM,
Chevalier I, Gauthier M, et al. Acute adenitis in children: Clinical course
and factors predictive of surgical drainage. J Paediatr Child Health 2005;
14: 273-277.
2. Gosche JR,
Vick L. Acute, subacute, and chronic cervical
lymphadenitis in children. Sem in Pediatr Surg 2006; 15: 99- 106.
3.Srouji IA, Okpala N, Nelseen E, et al. Diagnostic cervical lymphadenectomy in
children: a case for multidisciplinary assessment and formal management
guidelines. Int J Paediatr Otolaryngol 2004; 68: 551- 556.
4.Niedzielska G,
Kotowski M, Niedzielski A, et al. Cervical lymphadenopathy in children-
Incidence and diagnostic management. Int J Paediatr Otolaryngol 2007;
71: 51- 56.
5.Song JY, Cheong
HJ, Kee SY, et al. Disease
spectrum of cervical lymphadenitis: Analysis based on ultrasound-guided
core-needle gun biopsy. Journal of Infection 2007; 55: 310-316.
6.Nylen O, Berg
K, Anderson B. Cervical lymph node infection
with non-tuberculous mycobacteria in preschool children: interferon gamma
deficiency as a possible cause of clinical infection. Acta Paediatr 2000;
89: 1322-1325.
7.Brown
RL, Azizkhan RG. Pediatric
head and neck lesions. Pediatr Clin North Am 1998; 45:889-905.
8. Matsumoto
F, et al. Biopsy of cervical lymph node Auris Nasus
Larynx 2008; 1107.