Abstract
Objective: Vertebral osteomyelitis
is an uncommon illness; adults are mostly affected. Our objective is to
evaluate the short term outcome of oral versus parenteral antimicrobials treatment
for pyogenic (non-tuberculous and non-brucellosis) vertebral osteomyelitis, and
the best invasive diagnostic method yielding a microbiological diagnosis.
Methods: The medical records were
reviewed in a retrospective study for patients ≥ 18 years old from five urban hospitals
within Amman-Jordan; two teaching and three primary care hospitals, during the period
between August 1999 to June 2007. Due to the small numbers in the arm of
antimicrobials treatment, t-students’ test was used to assess inferences like
95% confidence interval and p-values for the difference among treatment arms.
Results: Seventy-four medical records
were available, inpatients records 35 from two teaching hospitals, 39 records from
three primary care hospitals. The orally treated patients showed lack of
difference against the parenteral therapy group at the end of 6 weeks therapy (p
> 0.05). Diagnostic methods tested for microbiological diagnosis were as
follows; True cut biopsy, fine needle aspiration and limited laminectomy did
not differ significantly in their microbiological diagnostic ability. Our data
suggested lack of difference between oral and parenteral therapy groups at the
end of six weeks treatment, but a questionable tendency (95% CI; -0.11 to 0.64,
p= 0.08). The diagnostic ability of the three methods did not suggest
significant differences (p >0.05), except for true cut biopsy versus fine
needle aspiration where it showed tendency (95% CI; - 0.20 to 0.42, p= 0.07).
Conclusion: The key to successful
management is the early diagnosis, and bone sampling for microbiological
examination, allowing proper antimicrobial selection. A proper bone sampling
method is important to evaluate, especially in the absence of surgical
indication and the co-notation in some parts of the world that M. tuberculosis
is the most -if not the sole- pathogen in vertebral osteomyelitis.
Key
words: Oral
treatment, Vertebral osteomyelitis, Vertebral osteomyelitis diagnostic
procedure.
JRMS
June 2011; 18(2): 43-48
Introduction
Vertebral osteomyelitis (VO) is an uncommon disease,
with incidence ranges between 1-7% of bone infections, and occurs at a rate of
1/100,000 in the general population, its incidence is increased in the
immunocompromised and with the increased number of invasive procedures as part
of diagnostic and therapeutic interventions. Before the advent of antibiotics large
proportions of patients with spinal infections died, estimated to be 40-70%.(1-3)
Well controlled studies addressing different aspects of VO have been sparse like
best diagnostic method(s), empiric antimicrobials treatment regimen whether parenteral
or oral, and the best empiric antimicrobial regimen used in the absence of
cultivable organism, especially in the era of availability of modern
antimicrobial agents with descent bone penetration like linezolid and tigecycline.(4-9)
Some oral agents are useful in the suppressive phase of VO treatment however; oral
antimicrobial agents are not widely recommended in the initial phase of VO treatment.
The short-term outcome of treatment was not
addressed in earlier studies; somewhat long-term outcome and mortality were evaluated.
In addition, case reports based on microorganisms reporting are abundant, whether
common microorganisms in endemic areas like in Brucellosis and Salmonellosis, or
rare ones like in, Aspergillus, Candida, Rhodococcus and Bartonella henselae.(1,10-17)
Some studies showed that S. aureus, Coagulase
Negative Staphylococcus (CoNS) and gram-negative bacilli were dominating.(3,10,11,18)
This
study was conducted to evaluate the short term outcome of oral versus
parenteral antimicrobials treatment for pyogenic (non-tuberculous and non-brucellosis)
vertebral osteomyelitis, and the best invasive diagnostic method yielding a
microbiological diagnosis.
Methods
Study design, setting and inclusion criteria:
This is a retrospective study from five hospitals;
two teaching, each of about 320 beds and three urban primary care hospitals,
each of about 100-120 beds. Approval for the study by the medical
administrators and/or ethics committee was obtained for the teaching hospitals.
Patients’ records were reviewed utilizing the following search terms; vertebral
osteomyelitis, unspecified osteomyelitis and disciitis for the period between
August 1999 and June 2007. Patients were considered for analysis if they were
18 years old or older and finished six weeks of therapy, and they received
antimicrobials as parenteral, oral or combined therapies (two weeks of
parenteral therapy followed by four or more weeks of oral therapy). Postoperative
VO patients were also included. Excluded patients were eight; younger than eighteen
years were 4, fractures 2, one with a tumor and one diagnosed as degenerative
disease (Table1).
Statistical analysis:
SPSS software version 15 was used. Study
variables were analyzed like the short-term outcome of oral versus parenteral antimicrobials,
and best invasive diagnostic method yielding a microbiological diagnosis. Due
to the small numbers in the arm of antimicrobials treatment, t-students’ test
was used to assess inferences like 95% confidence interval and p-values for the
difference among treatment arms.
Results
Patients Demographic Features:
Eighty-two patients were available for review;
eight patients were excluded (Table I). Seventy-four patients met the diagnosis
of VO inpatients were 35. Thirty-nine (52.7%) patients were from other three primary
care hospitals. Postoperative VO was found in 9 (12.1%) cases, four (5.4%) patients
with paravertebral abscesses, two of which were tuberculous. There were 74
patients with 74 episodes of VO, the mean age was 49.5 years (males mean age was
50.9 years, females mean age was 46.9 years). Males made up 48 (64.9%) and females
26 (35.1%). Fifty (72.4%) patients had no comorbidities and in the rest,
diabetes mellitus was the most common comorbidity. Data for the site and extent
of disease were available for 69 patients, the lumbar vertebrae were mostly
affected; lumbar 42 (60.8%), lumbosacral 10 (14.5%), and 22 (29.7%) other sites.
The majority of patients, 61 (88.4%) got more than one vertebra involved; two adjacent
vertebrae in 46 (69.7%), three adjacent vertebrae in 9 (13.6%) (Table II).
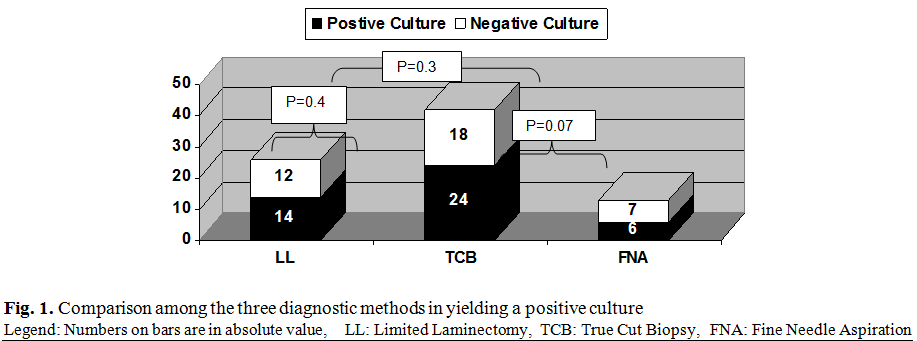
Diagnostic procedures:
Eighty-one diagnostic procedures were available
for 62 patients. In twelve patients the information was not clear which
procedure(s) gave the diagnosis and were excluded (Table III). True cut biopsy (TCB)
was done in 42 patients with positive microbiological result in 24 (57%), fine
needle aspiration (FNA) in 13 patients with positive microbiological result in
6 (46%), laminectomy (LL) in 26 with positive microbiological result in14
(54%). The paired comparisons between the three diagnostic groups in getting a
microbiological diagnosis showed lack of means’ difference between procedures; TCB vs. LL (95%CI; -0.23 to 0.29, p =0.4). TCB vs. FNA (95%CI; - 0.20 to 0.42, p= 0.07). FNA vs. LL (95%CI; -0.25 to 0.41, p=0.3).
Table I. Patients flow and
distribution
|
Total
number of patients
|
82
|
|
Total
number of excluded patients
|
8
|
|
Younger
than 18 yrs of age
|
4
|
|
Diagnosed
as a fracture
|
2
|
|
Diagnosed
as a tumor
|
1
|
|
Diagnosed
as degenerative disease
|
1
|
|
Total
number of studied patients
|
74
(100%)
|
|
Post
operative cases
|
9
(12.1%)
|
|
Patients
with abscess
|
4
(5.4%)
|
|
Patients
from three primary care hospitals*
|
39
(52.7%)
|
|
Patients
from the two teaching hospitals
|
35
(47.3%)
|
* Including
patients from Al Khalidi Medical Center, the Specialty
Hospital and the Arab Medical
Center
Table
II.
Demographic characteristics and clinical features of 74 cases of Vertebral Osteomyelitis
|
Feature
|
Number
of patients/ Total numbers available for analysis
|
|
Age
|
Mean ±
SD
|
49.5 ±
14.0 yrs
|
|
|
Range
|
22-76 yrs
|
|
Gender
|
Male
|
48/74
(64.9%)
|
|
|
Female
|
26/74
(35.1%)
|
|
Residence
|
Jordanians
|
36/74
(48.6%)
|
|
|
Other
Arabs
|
36/74
(48.6%)
|
|
|
Not
entered
|
2/74(2.7%)
|
|
Anatomical
location
|
Lumber
|
42/69
(60.9%)
|
|
|
Lumbosacral
|
10/69
(14.5%)
|
|
|
Thoracic
|
8/69
(11.6%)
|
|
|
Cervical
|
4/69
(5.8%)
|
|
|
Thoracolumbar
|
3/69
(4.3%)
|
|
|
Sacral
|
1/69
(1.4%)
|
|
|
Cervicothoracic
|
1/69
(1.4%)
|
|
Extent
of Disease
|
One
vertebra
|
8/69
(11.6%)
|
|
|
Two
vertebrae or more
|
61/69
(88.4%)
|
|
Morbidities
|
Diabetes mellitus
|
18/69
(26.5%)
|
|
|
Renal
failure
|
2/69
(2.7%)
|
|
|
Bone and joint diseases
|
1/69
(1.4%)
|
|
|
No Comorbidity
|
50/69
(72%)
|
|
|
Not
available
|
5/69
(7.2%)
|
Table
III.
Eighty one Invasive procedures used in the diagnosis of available 62 patients
with Vertebral Osteomyelitis
|
Finding
|
Positive
finding/total number of available invasive procedures
|
|
True Cut
Biopsy
|
24/42
(57%)
|
|
Fine
needle aspiration
|
6/13
(46%)
|
|
Limited
laminectomy
|
14/26
(54%)
|
|
Procedure-recovered microbiological findings
for 44 patients in whom data were
available
|
|
S.
aureus (including 5 MRSA*)
|
8/44
(22.7%)
|
|
CoNS**
|
5/44
(11.3%)
|
|
Brucellosis
|
4/44
(9.0%)
|
|
Tuberculosis
|
10/44
(22.7%)
|
|
Salmonellosis
|
1/44
(2.2%)
|
|
Other
includes (Burkholderia cepacia, Proteus mirabilis, 2 pseudomonas, E. coli,
Serratia, Acinetobacter, Klebsiella, one case from above (Klebsiella plus
MRSA).
|
8/44
(18.1%)
|
|
No
growth
|
17/44(38.6%)
|
*MRSA =
Methicillin-resistant Staphylococcus aureus **CoNS = Coagulase Negative Staphylococcus
Forty-four
patients in whom data were available (Table III): Eight (18%) isolates were
Staphylococcus aureus (six MRSA, one case postoperative). Five (11.3%) isolates
were CoNS, none recorded to have previous hardware in his/her back.
Mycobacterium tuberculosis constituted 10 (22.7%) isolates. Brucellosis
constituted 4 (9.0%) plus two from blood culture. (Patients with tuberculosis
and brucellosis were excluded from treatment analysis). One case (2.2%) was Salmonellosis.
The rest of the microbiological isolates were 8 (18.1%) different gram negative
bacilli, and the remaining 17(38.6%) showed no growth.
Antimicrobials therapies follow up:
Fifty-three patients were available at the end
of six weeks of therapy for follow up; forty one (77.3%) of the followed up
patients had improvement in pain and ambulation. Parenteral therapy constituted
only 9 patients, four (44.4%) patients showed improvement in pain and
ambulation. Combined therapies were administered in 21 patients, ten (47.6%)
showed improvement of pain and ambulation, when compared with parenteral
therapy there was no significant difference (95% CI; - 0.32 to 0.35, p = 0.4).
The oral therapy group, our main concern to analyze, excluding MTB and brucellosis-constituted
24 patients: seventeen (70.8%) patients showed improvement in pain and
ambulation, when compared with parenteral therapy (95% CI; -0.11 to 0.64, p =
0.08). Anti-tuberculosis therapies were used
in 10 patients, anti-brucellosis regimen in 6 patients (two were diagnosed by
blood cultures), both groups were excluded from analysis.
Radiological diagnosis:
Imaging data were available for 72 patients. MRI
was utilized in 65 patients from whom 61 (93.8%) patients findings were
described as diagnostic of VO, CT scan data were available for 15 patients from
whom 8 (53.3%) patients’ findings were diagnostic of VO.
Erythrocyte Sedimentation Rate:
Seventeen paired orally treated patients were
available for analysis. The ESR improvement in means difference for the oral
showed significant improvement (means’ difference: 95% CI 11.5–52.3,
p= .004), likewise the combined therapy group improvement at the start and at
the end of six weeks therapy were (95% CI
9.2–52.4, p = 0.009), and likewise the parenteral treatment group with
significant means difference i.e. improvement (95% CI 7.4-71, p = 0.02).
Discussion
The primary outcome measures were to evaluate the
short term outcome benefit at the end of 6 weeks for the oral therapy group
(excluding tuberculosis and brucellosis, since both infections’ treatment is
essentially oral), and the ability of the three tested invasive diagnostic
procedures in obtaining a microbiological diagnosis. We compared the outcome of
the three arms of treatment in pairs, the oral, the parenteral, and combined at
the end of six weeks therapy. This comparison was made to identify if we can
formulate some different treatment recommendation about the method of antimicrobial
administration i.e. employing the oral therapy and whether it is as good as the
parenteral therapy, as our review did not materialize studies based on oral
therapy.(1,3,10) The oral therapy group did not suggest a
significant difference from parenteral therapy for improvement, but rather
tendency (95% CI; -0.11 - 0.64, p= 0.08). The combined therapy group and the
parenteral group did not show a significant difference though it is marginal
(95%CI; -0.048 - 0.512, p= 0.055). The availability of oral antimicrobial
agents with proper spectrum, high bioavailability and good bone concentration
may argue to employ them, at least in some patients suffering from
microorganisms that respond to those oral regimens, prospective randomized studies
are needed with this regard.
TCB is a reliable and practical procedure for
obtaining a microbiological diagnosis, as good as LL, with no significant
difference (95% CI; -0.214 - 0.274, p = 0.4). But TCB showed tendency for
reliability over FNA (95%CI; - 0.20 to 0.42, p=0.07). This study tends to recommend that LL should
not be utilized unless surgical intervention for other indications other than
sampling is deemed necessary (Fig. 1).
Inflammatory parameters showed improvement in
the oral treatment group at the end of six weeks therapy at least as good as
parenterally treated patients (p < 0.05). Males predominate in VO (64.9%) in
line with others; the majority of this population was elderly
but about a decade younger than previously published elsewhere where median age was 60 and 62.5 years. Diabetes mellitus was the commonest comorbidity (26.5%), (diabetes incidence in Jordanian adult population is 13.4%), two patients were diabetic with renal failure (2.7%). No sickle cell disease or intravenous drug users were identified, both are rare in Jordan.(1,3,10,19-22)
The location and extent of disease showed that majority
were lumbar (60.9%), followed by lumbosacral (14.5%) followed by other sites.
The extent of involvement was mostly multiple vertebrae in 61(88.4%) patient, all were adjacent;
and the majority were two adjacent ones (69.7%) matching earlier studies.
Adjacent vertebrae are jointly affected due to the mode of pathogens spread through
blood supply as well as the anatomical extension.(10,18,19)
Mycobacterium tuberculosis followed by S. aureus
including MRSA took the lead. One out of six cases of MRSA was from postoperative
source and five cases were community acquired (CA-MRSA). CA-MRSA is now
increasing in incidence; it is expected to contribute to the future burden of
VO, especially in individuals who have been recently hospitalized, had
hemodialysis, surgery, catheterization, and those in need of ambulatory medical
care. Of note here is the presence of
MTB (22.7%) and Brucellosis (9.0%) in considerable proportion, though the
battle against both diseases is ongoing in Jordan and nearby Arab countries,
it seems further efforts are needed. Some studies did not show tuberculosis
among their patients; it is imperative to look at ones’ regional data for management
that is more precise rather than relying on data from other regions with
different epidemiology.(3,10,12-17,23)
The imaging investigation mostly utilized
was MRI.
The number of vertebral bodies involved is less in pyogenic
than in tuberculous VO, and the paravertebral abscesses are smaller, probably due
to the insidious onset of tuberculosis and its propensity not to induce intense
inflammation for it lacks endotoxins and exotoxins, in our patients all had two
or more vertebrae involved with two patients had abscesses on presentation. In our experience, bone
scan may be needed in MRI borderline cases. Should be there a contraindication
to MRI then CT scan is a useful option, however CT is less sensitive than MRI
for the detection of epidural abscesses or soft tissue lesions. In our review of
CT scan studies, it was described as diagnostic in 53.3% of patients. Plain
radiological investigation was found earlier not sensitive in VO diagnosis,
even Colmenero et al. found that plain radiography was repeatedly normal
throughout the entire evolutive course in 7/219 (3.1%) patients, six had brucellosis,
and one had tuberculous VO.(4,6,11,16,19,25)
ESR lacks specificity but is useful in follow up,
it showed that both orally-treated and parenterally-treated groups demonstrated
similar improvement between the start and at the end of six weeks (p <
0.05), though patients’ numbers were small to make a firm conclusion.(18,19)
Conclusion
TCB is a
reliable procedure in yielding microbiologic diagnoses especially if surgical intervention
was not found necessary. However, the initial antimicrobial treatment in the
first six weeks is parenteral, but this study threw light that it may be in some cases
replaced by oral
therapy, or shorter parenteral
course may be administered (two weeks) and to follow that by oral treatment. In
the era of some oral antimicrobials with descent bone concentration and spectrum,
that covers the concerned potential pathogens; larger interventional studies
are needed to address this point, as it bears significant cost effectiveness in
sources limited patients and countries, and better patient compliance. The
shortcoming of our study is that we did not adjust for the difference in
diseases severity, comorbidities or different pathogens among the therapy
groups, the patients’ number were small, and due to the nature of the study, specific
oral antimicrobial agents were not tested against specific parenteral ones.
Furthermore, a randomized controlled study knows how to answer the outcome more
precisely and highly needed.
Acknowledgment
We thank the Islamic Hospital and Jordan Hospital
for their cooperation in conducting the study, Dr. Mazen Alqathi, the Islamic
Hospital, and Reem Jamal Wadi for her help in statistical analysis.
References
1.Nather A, David V, Hee HT, Thambiah J.
Pyogenic vertebral osteomyelitis: a review of 14 cases. Journal of
Orthopaedic Surgery 2005;13(3):240-244
2.Lee
BB. Vertebral osteomyelitis and psoas abscess occurring after
obstetric epidural anesthesia. Regional Anesthesia and Pain Medicine 2002
March 2; 27: 220-224
3.Acosta FL Jr, et al. Diagnosis and management
of adult pyogenic osteomyelitis of the cervical spine. Neurosurg Focus 2004; 17(6):E2
4.Arizono
T, Oga M, Shiota E, et al. Differentiation of
vertebral osteomyelitis and tuberculous spondylitis by magnetic resonance
imaging. International Orthopaedics 1995 October; 19(5):319-322
5.Meyers
SP, Wiener SN. Diagnosis
of hematogenous pyogenic vertebral osteomyelitis by magnetic resonance imaging. Archives of Internal Medicine 1991 April 1;151(4)
6.Abbey
DM, Hosea SW. Diagnosis of vertebral osteomyelitis in a community hospital by using
computed tomography. Archives of Internal Medicine 1989 September; 149(9):
2029-2035.
7.Lovering MA, Zhang J, Bannister GC, et al. Penetration of linezolid into bone, fat, muscle and haematoma of patients undergoing routine hip replacement. Journal of Antimicrobial Chemotherapy 2002; 50: 73-77.
8.Melzer M,
Goldsmith D, Gransden W. Successful Treatment
of Vertebral Osteomyelitis with Linezolid in a Patient Receiving Hemodialysis
and with Persistent Methicillin - Resistant Staphylococcus aureus
and Vancomycin-Resistant Enterococcus Bacteremias.
Clinical Infectious Diseases 2000; 31:208-209.
9.Yin LY, Lazzarini L, Li F, et al. Comparative evaluation
of tigecycline and vancomycin, with and without rifampicin, in the treatment of
methicillin resistant Staphylococcus aureus experimental osteomyelitis in a
rabbit model. Journal of Antimicrobial Chemotherapy 2005; 55: 995–1002
10.McHenry
MC, Easley KA, Locker GA. Vertebral osteomyelitis: long-term outcome for
253 patients from 7 cleveland-area hospitals. Clinical Infectious Diseases
2002; 34:1342–1350
11.Fernandez
M, Carrol CL, Baker CJ. Discitis and vertebral osteomyelitis in
children: an 18-year review. Pediatrics 2000;105:1299-1304
12.Colmenero JD, Ruiz-Mesa JD, Plata A, et al. Clinical findings, therapeutic approach, and outcome of brucellosis vertebral osteomyelitis. Clinical Infectious Diseases 2008; 46(3):426-433
13.Santos EM, Sapico Francisco L. Vertebral osteomyelitis
due to Salmonellosise: report of two cases and review. Clinical Infectious
Diseases 1998; 27: 287–295
14.Vinas FC, King PK, Diaz FG. Spinal
Aspergillus Osteomyelitis. Clinical Infectious Diseases 1999; 28: 1223-1229
15.Hendrickx L, Van Wijngaerden E, Samson I,
Peetermans W E.
Candidal vertebral osteomyelitis: report of 6 patients, and a review. Clinical
Infectious Diseases 2001; 32:527–533
16.Fischer L, Sterneck
M, Albrecht H, et al.
Vertebral osteomyelitis due to rhodococcus
equi in a liver transplant recipient. Infectious Diseases 1998; 26:
749–752
17.Hulzebos CV,
Koetse HA, Kimpen JLL, Wolfs T FW. Vertebral osteomyelitis
associated with cat-scratch disease. Clinical Infectious Diseases 1999;28:1310–1312
18.Lew
DP, Waldvogel FA. Osteomyelitis. The Lancet 2004 July 24; 364(9431): 369-379
19.Colmenero
JD, Jiménez-Mejías ME, Sánchez-Lora FJ, et al. Pyogenic,
tuberculous, and brucellosisr vertebral osteomyelitis of 219 cases: a
descriptive and comparative study.
Ann Rheum Dis 1997;56(12):709-715
20.Ajlouni
K, Jaddou H, Batieha A. Diabetes and impaired glucose intolerance in Jordan: Prevalence
and associated risk factors. Journal of Internal Medicine 1998; 244:
317-323
21.Al-Rimawi
HS, Abdul-Qader M, Jallad MF, Amarin ZO. Acute Splenic Sequestration In Female
Children With Sickle Cell Disease In The North Of Jordan. Journal of Tropical
Pediatrics 2006;52(6):416-420
22.H M
Queen Noor of Jordan. Prevention as an issue
of concern for all nations: Mentor Substance Abuse Prevention Forum. The Marsh
Centre, January 25th, 2000; [Cited May 25, 2008]; Available from:
http://www.noor.gov.jo/main/mentor.html.
23.CDC. Multidrug-Resistant
Organisms in Non-Hospital Healthcare Settings.
Community-Associated MRSA. [Cited May 25, 2008]; Available from: http://www.cdc.gov/ncidod/dhqp/ar_mrsa.html
24.American
Thoracic Society: Diagnostic Standards and Classification of Tuberculosis in
Adults and Children Am J Respir Crit Care Med. 2000 April;161(4):1376-1395
25.Miller
JC, Phil D.
Radiology Rounds, Vertebral Osteomyelitis. 2006 Novermber/December; 4(11).