Abstract
Objectives: To assess the
sensitivity of the Brückner test in detecting a change in the brightness of the
fundus reflex (Brückner reflex) when the fixation point changes between the
ophthalmoscope light and a visual target beside the ophthalmoscope.
Methods:
In a
prospective, single blinded, randomized study, 3 experienced examiners
conducted the Brückner test on 10 subjects with central fixation, normal visual
acuity (≥ 1.0), and absence of any organic eye disorder. The test was performed
at a distance of 1 m with and without pupillary dilatation, allocating 4
different degrees of ocular deviation (2.5 deg, 5 deg, 7.5 deg, 10 deg) on
either side of the ophthalmoscope. The lateral fixation targets were marked by
bold crosses. The subjects were asked to close one eye and to change fixation
between the light of the ophthalmoscope and one of the 8 crosses starting
either at the light or at one of the eccentric targets. The sequence of targets
was unpredictable for the examiner and followed a previously prepared chart on
which the targets were called A or B in a pseudo-random order. In each trial,
the examiner had to state in which position, either A or B, the Brückner reflex
appeared brighter, this when the subject was fixating the light or the
eccentric target (or vice versa). Subjects were divided into 2 groups, 5
emmetropes aged 17-24 years (mean 21 years), and 5 myopes (0.25-2.50 diopters) aged 21-25 years (mean
23.6 years).
Results: With non-dilated pupils, in 97.2% of 160 trials on emmetropes (OD, 96.2%;
OS, 98.1%) and 97.5% of 160 trials on myopes (OD, 96.9%; OS, 98.1%), the red
reflex appeared brighter when the subject fixated the eccentric target. With
dilated pupils, corresponding rates were 97.2% (OD, 95.1%; OS, 99.3%) in 144
trials on emmetropes and 99.7% (OD, 99.4%; OS, 100%) in 160 trials on myopes,
regardless of horizontal direction and degree of eccentricity.
Conclusion: In eyes without
organic pathology, the Brückner test allows for sensitive discrimination
between alternate central fixation of the ophthalmoscope light and fixation of
a target beside the light.
Key
words: Amblyopia; Brückner reflex; Brückner test; Strabismus
JRMS
September 2011; 18(3): 10-15
Introduction
The idea of
performing a test which allows detection of strabismus and other amblyogenic
risk factors by means of the fundus red reflex came from the German and French(1)
literature through an article published in 1962 by Roland Brückner, who was an
ophthalmologist working in Basel,
Switzerland, at
that time. Brückner illuminated both pupils from a distance of 1 m and assessed
the following criteria [Brückner 1962]:( 2)
1.
Position of the 1st Purkinje images
relative to the pupil
2.
Colour of the fundus red reflex in the pupil
3.
Size and constriction of the pupils
4.
Eye movements with alternating illumination of the
pupil
Assessment of the
first two criteria requires simultaneous illumination of both eyes, while
assessment of the following two criteria
requires alternate illumination of both eyes. Comparison of the positions of the
1st Purkinje images in both eyes had already been described by
Hirschberg as a method to estimate the amount of manifest strabismus.
Hirschberg assumed that asymmetry of 1 mm in the 1st Purkinje images
of both eyes corresponded to a squint angle of 7
degrees.(3) Later it has been shown that factually 1mm corresponds
to an angle of 12 degrees.(3,4) Therefore and due to possible difference in
the angle kappa between both eyes, the use of the Hirschberg method to detect
small angle strabismus is limited. In 1965, Brückner stressed the essential
component of his test which is the assessment of the red reflex of the fundus
when the pupil is lighted and viewed through a direct ophthalmoscope.(5)
He described inter-ocular difference in brightness of the red reflex in
manifest strabismus with the brighter reflex coming from the deviated eye when
the patient was fixating the ophthalmoscope light. This component was new
regarding strabismus diagnosis.
Amblyopia is
estimated to affect approximately 2-5% of the population in the Western
countries, and is the leading cause of vision loss in children and adults. It
is considered a significant preventable cause of vision loss. Causes of
amblyopia include ptosis, media opacities, strabismus, and refractive errors.(6-9)
Early detection of these factors plays a role in preventing or minimizing the
deepening of amblyopia. Reliance on the subjective response and cooperation of
the child being examined is the limiting factor in performing screening tests
to detect amblyopia.(1,6,8) Brückner test can overcome such
obstacles.
The Brückner test
is performed with a direct ophthalmoscope. While the light beam is directed
into the patient’s eyes simultaneously, the reflected light coming from the
pupillary zone should be observed and evaluated in terms of glowing bright red
reflex or dim red reflex. Dimming occurs in the fixating eye when the patient
takes up central fixation of the ophthalmoscope light. One of the major factors explaining the dimming phenomenon is the pupillary
light reflex. Central fixation of the ophthalmoscope light causes pupillary
constriction due to the higher light sensitivity of the fovea compared to the
paracentral or peripheral retina. So the pupils become smaller when the patient
looks directly into the ophthalmoscope light. This leads to both less
illumination of the retina and less amount of light coming back through the
small pupil to the examiner’s eye. Since direct and consensual pupillary light
reflexes are nearly equal, detection of strabismus by means of inter-ocular
asymmetry in the fundus red reflex, i.e., by lack of foveal dimming in the
deviated eye, cannot be explained by pupillary constriction.(1,2,5,6,10)
So, if strabismus shall be detected by asymmetry in the fundus reflex of both
eyes not due to anisometropia, differences in reflectivity of the central vs.
paracentral retina or retinal surface, respectively, must be the decisive
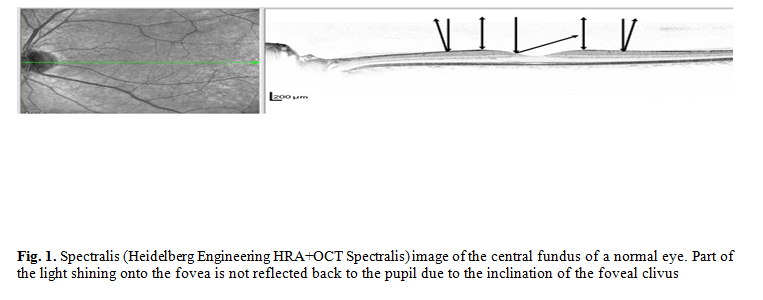
factor (Fig. 1). As a precondition to detect strabismus by inter-ocular
difference in the fundus red reflex, the test must allow for reliable discrimination
between the red reflexes of the central and the eccentric fundus.
This
study was conducted to
investigate the capability to discriminate between central monocular
fixation of the ophthalmoscope light and of a target beside the light when the
gaze was alternating between both targets.
Methods
This single
blinded study was conducted in the Department of Ophthalmology, Justus-
Liebig-University of Giessen.
Examiners were two ophthalmologists and one medical student in his 6th
year of medical education. A scale was prepared in the form of a cartoon bar
which was fixed horizontally on the front side of the ophthalmoscope head (Beta
200, Heine Optotechnik, Herrsching,
Germany). On
this bar, four fixation targets on either side of the ophthalmoscope were drawn.
Their position was calculated by using the tangent function. In centimeters,
this were 100 tan α, for α = 2.5 degrees, 5.0 degrees, 7.5 degrees, and 10
degrees. Targets were marked as red and black bold crosses, alternating in
color, to make communication and fixation easier.
First the experiment was explained to the participants who were medical students and trainee orthoptists (in the following
called subjects). Written informed consent was obtained
from
all subjects adhering to the tenets of the Declaration of Helsinki. All subjects underwent autorefractometry (Topcon RM-8800), visual acuity determination (according to EN ISO 8596), slit lamp examination (Haag Streit M-900) for the anterior and posterior segments using a 78 D biomicroscopy lens (Volk Double Aspheric), stereo testing (Lang 1 random dot stereo test), and orthoptic examination including alternate cover testing at far fixation (5m) of a small light and near fixation (0.3m) of a small recognition target forcing accommodation. Exclusion criteria were any organic eye disease, strabismus, and hypermetropia.
Then the subject received by the investigator
a sheet on which for each trial the position of the ophthalmoscope light was
defined by the letter A or B and one of the eight visual targets by the
opposing letter B or A. Eight such positional orders according to the 8
eccentric target positions were pre-defined in a pseudo-random sequence. The
distance between the examiner and the subject was adjusted to 1 m. The room
light was switched to dim mood and the subject was asked to close one eye by
his or her hand. The investigator who stood behind the examiner let the subject
move gaze between A and B, according to the scheme on the sheet. The examiner
looked through the ophthalmoscope and had to decide which position, A or B,
gave the brighter red reflex. The decision was recorded by the investigator or
by a fourth person. The same procedure was performed on the other eye. In
another session, the subjects were examined again, following the same protocol,
10 minutes after installation of 3 drops of tropicamide 1% solution
(Mydriaticum Stulln®) within 20 minutes. Pupillary dilatation and
complete blockage of the pupillary light reflexes were mandatory. In all stages
of testing the test was carried out at least by two of the three examiners.
Results
The 10 subjects were divided into 2
groups. Group 1 included 5 emmetropic female subjects aged 17 to 24 years (mean,
21 years). With non-dilated pupils (Table I), there were 160 trials on each
eye, 64 for examiner 1(QA), 80 for examiner 2 (CV) and 16 for examiner 3 (MG).
The trials of each examiner were performed for all eccentricities on the
examined subject. Finally, there were 8 trials on each eccentricity for QA, 10
for CV, and 2 for MG. Examination on right eye (OD) yielded the brighter reflex
from the nasal fundus (i.e., when the subject was fixating a target on the left
hand side of the ophthalmoscope light compared to fixation of the
ophthalmoscope light) and the dimmer reflex from the fovea in 18 (2.5 deg), 20
(2-5 deg), 20 (7.5 deg), and 20 (10 deg) of 20 trials. Comparing fixation of
the ophthalmoscope light and a target on the right hand side of the light, the
brighter reflex came from the temporal fundus in 19, 20, 18, and 19 of 20
trials, respectively. In left eye (OS), 20, 20, 20, and 19 of 20 trials the
brighter reflex came from the nasal and 19, 20, 20, and 19 trials from the
temporal fundus. Thus in 97.2% (OD, 96.2%; OS, 98.1%) of trials on emmetropes,
the red reflex appeared brighter when the subject was fixating an eccentric
target compared to fixation of the ophthalmoscope light, regardless of the
horizontal direction and degree of eccentricity of the eccentric target.
With the use of mydriatic eye drops on
the same subjects, there were 144 trials (QA, 64; CV, 80). Out of 18 trials on
each eccentricity in OD, the reflex from the nasal fundus appeared brighter
compared to the central reflex in 17, 18, 18, and 18 trials. The reflex from
the temporal fundus was brighter in 17, 18, 15, and 16 trials, respectively.
For OS, corresponding rates were 18, 18, 18, and 18 nasally and 17, 18, 18, and
18 temporally. Thus, of 144 trials on mydriatic
emmetropes, 97.2% (OD,95.1%; OS, 99.3%)
yielded the brighter red reflex when the subject was fixating an eccentric
target compared to fixation of the ophthalmoscope light, regardless of the
horizontal direction and degree of eccentricity of the target (Table II). This means, the mean sensitivity of the test to detect
central fixation of the ophthalmoscope light was 97.2% both with reactive and
with dilated pupils.
Group 2 included 5 subjects aged 21-25
years (mean 23.6 years) who were myopic by -0.25 to -2.50 diopters in OD and
-0.25 to -2.00 diopters in OS. Of 160 trials conducted without mydriatic eye
drops, 64 were performed by QA, 80 by CV, and 16 by MG with the following
results (Table III). In OD, the
brighter reflex came from the nasal fundus in 18, 18, 20, and 20 trials and
from the temporal fundus in 20, 19, 20, and 20 trials. In OS, the corresponding
rates were 20, 20, 20, 20 and 19, 19, 20, 19. Thus, 97.5% (OD, 96.9%;
OS, 98.1%) of trials on myopes yielded the brighter red reflex was when the
subject was fixating the eccentric target, regardless of its eccentricity.
With mydriatic pupils, corresponding
rates were 19, 20, 20, 20 (OD nasal) and 20, 20, 20, 20 (OD temporal) as well
as 20, 20, 20, 20 (OS nasal) and 20, 20, 20, 20 (OS temporal). Except 1 trial,
the Brückner reflex always (99.6%) appeared brighter with fixation of the
eccentric target or from the eccentric fundus, respectively (Table IV). This means, there
was no significant difference in test sensitivity to detect central fixation of
the ophthalmoscope light between myopic and emmetropic eyes, neither with
reactive or with mydriatic pupils.
Discussion
Results of this study show a high
sensitivity of the test to detect central fixation of the direct ophthalmoscope
light by the Brückner reflex test. When fixation changed back and forth between
the ophthalmoscope light and an eccentric target, dimming of the Brückner
reflex was detected, regardless of the degree of eccentricity of this visual
target. Sensitivity did not decrease when pupils were dilated. Results in
emmetropic and myopic eyes were equal at that examination distance.
Table I. Results in emmetropic eyes with non-dilated pupils
|
Temporal
vs. central
|
Nasal
vs. central
|
Total
No. of trials on each eye
|
|
|
Foveal
dimming
|
Foveal
dimming
|
|
10o
OD/OS
|
7.5o
OD/OS
|
5.0o
OD/OS
|
2.5o
OD/OS
|
10o
OD/OS
|
7.5o
OD/OS
|
5.0o
OD/OS
|
2.5o
OD/OS
|
|
8/7
|
6/8
|
8/8
|
7/8
|
8/7
|
8/8
|
8/8
|
8/8
|
64
|
Examiner
1
|
|
9/10
|
10/10
|
10/10
|
10/10
|
10/10
|
10/10
|
10/10
|
9/10
|
80
|
Examiner
2
|
|
2/2
|
2/2
|
2/2
|
2/1
|
2/2
|
2/2
|
2/2
|
1/2
|
16
|
Examiner
3
|
|
19/19
|
18/20
|
20/20
|
19/19
|
20/19
|
20/20
|
20/20
|
18/20
|
160
|
Total
|
Table
II. Results in emmetropic eyes with dilated pupils
|
Temporal
vs. central
|
Nasal
vs. central
|
Total
No. of trials on each eye
|
|
|
Foveal
dimming
|
Foveal
dimming
|
|
10o
OD/OS
|
7.5o
OD/OS
|
5.0o
OD/OS
|
2.5o
OD/OS
|
10o
OD/OS
|
7.5o
OD/OS
|
5.0o
OD/OS
|
2.5o
OD/OS
|
|
8/8
|
6/8
|
8/8
|
7/8
|
8/8
|
8/8
|
8/8
|
8/8
|
64
|
Examiner
1
|
|
8/10
|
9/10
|
10/10
|
10/9
|
10/10
|
10/10
|
10/10
|
9/10
|
80
|
Examiner
2
|
|
16/18
|
15/18
|
18/18
|
17/17
|
18/18
|
18/18
|
18/18
|
17/18
|
144
|
Total
|
Table III. Results in myopic eyes
with non-dilated pupils
|
Temporal
vs. central
|
Nasal
vs. central
|
Total
No. of trials on each eye
|
|
|
Foveal
dimming
|
Foveal
dimming
|
|
10o
OD/OS
|
7.5o
OD/OS
|
5.0o
OD/OS
|
2.5o
OD/OS
|
10o
OD/OS
|
7.5o
OD/OS
|
5.0o
OD/OS
|
2.5o
OD/OS
|
|
8/7
|
8/8
|
7/7
|
8/8
|
8/8
|
8/8
|
7/8
|
7/8
|
64
|
Examiner
1
|
|
10/10
|
10/10
|
10/10
|
10/9
|
10/10
|
10/10
|
9/10
|
9/10
|
80
|
Examiner
2
|
|
2/2
|
2/2
|
2/2
|
2/2
|
2/2
|
2/2
|
2/2
|
2/2
|
16
|
Examiner
3
|
|
20/19
|
20/20
|
19/19
|
20/19
|
20/20
|
20/20
|
18/20
|
18/20
|
160
|
Total
|
Table
IV. Results in myopic eyes with dilated pupils
|
Temporal
vs. central
|
Nasal
vs. central
|
Total
No. of trials on each eye
|
|
|
Foveal
dimming
|
Foveal
dimming
|
|
10o
OD/OS
|
7.5o
OD/OS
|
5.0o
OD/OS
|
2.5o
OD/OS
|
10o
OD/OS
|
7.5o
OD/OS
|
5.0o
OD/OS
|
2.5o
OD/OS
|
|
8/8
|
8/8
|
8/8
|
8/8
|
8/8
|
8/8
|
8/8
|
7/8
|
64
|
Examiner
1
|
|
10/10
|
10/10
|
10/10
|
10/10
|
10/10
|
10/10
|
10/10
|
10/10
|
80
|
Examiner
2
|
|
2/2
|
2/2
|
2/2
|
2/2
|
2/2
|
2/2
|
2/2
|
2/2
|
16
|
Examiner
3
|
|
20/20
|
20/20
|
20/20
|
20/20
|
20/20
|
20/20
|
20/20
|
19/20
|
160
|
Total
|
The dimming phenomenon is a necessary precondition to detect strabismus by means of red reflex asymmetry between eyes. Provided normal pupillomotor innervation and normal
reactivity of both pupils, pupillary light reflexes are equal in both eyes when one
eye is illuminated. The light coming out of both eyes should be equal, if there
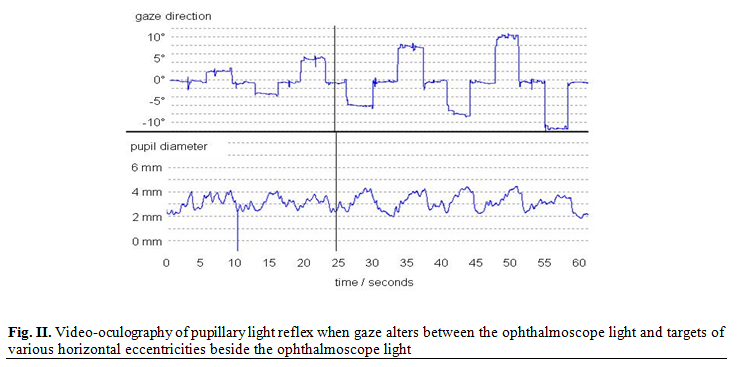
is no difference in fundus reflectivity. Dimming of the Brückner reflex can be
caused by pupillary constriction which is stronger when the ophthalmoscope
light falls on the fovea because the retinal light sensitivity is maximal in
the fovea (Fig. 2). The fact that results both with
reactive and dilated pupils were equal shows that pupillary light reflex cannot
be the exclusive cause of the dimming phenomenon. As a second possible cause of
dimming, Brückner mentioned stronger pigmentation compared to the more
peripheral fundus and as a third, light reflection at the retinal surface.(2)
Due to the inclination of the foveal clivus, part of the light shining through
the pupil onto the fovea will not be reflected back to the pupil (Fig. 1).
This may be the most decisive factor
explaining foveal dimming and would also explain the frequent lack of the dimming
phenomenon in young infants,(11) when their fovea is not yet
differentiated to an adequate stage. Archer et al.(12)
mentioned that neonates and most infants younger than 2 months of age do not
show dimming of the fundus reflex with fixation. The lack of dimming may be
explained by still lacking differentiation of the foveal pit as described above.
Roe and Guyton(10)
described specular reflection of the retina from the internal limiting membrane
that changes slope with ocular rotation. If significant amount of light were
reflected from the internal limiting membrane of the retina, perhaps the slope
of the foveolar pit would reflect enough light away from the pupil. For that
the red reflex darkens but does not entirely disappear, as the fundus red
reflex is not solely caused by reflection from the choroid and the retinal pigment epithelium.(13)
However, it is a different task to assess
the Brückner reflex in the same eye when the patient changes fixation between
the ophthalmoscope light and a second target, than to compare the brightness of
simultaneous Brückner reflexes in both eyes. The first task does not require
any gaze movement of the observer who can concentrate on the same pupil and
successive change in its brightness. The latter task requires a gaze movement
of the observer from one eye to the other eye of the patient. Alternatively the
observer can view the patient’s nose to assess brightness of both reflexes.
Both methods seem to be less sensitive to detect small difference in
brightness.
Griffin et al.(14)
used a photographic method for Brückner testing and found 80% of ocular deviations
could be diagnosed when the degree of deviation was at least 5 prism diopters,
but they noticed subject error with their method. Thus, detection of manifest
strabismus by interocular difference in the fundus reflex appears to be more
difficult than discrimination between successive foveal and peripheral retinal
illumination in the same eye.
Conclusion
By using the
Brückner test, the dimming phenomenon allows for highly sensitive
discrimination of foveal vs. parafoveal retinal illumination when the patient’s
gaze changes between the ophthalmoscope light and an eccentric visual target. It seems to be easier to detect
successive changes in brightness of the same pupil than an equal difference in
brightness between both pupils which can be caused by strabismus. Regarding the
sensitivity to detect small angle strabismus by means of asymmetry in the
fundus red reflex, further investigation will be necessary.
References
1.Tongue AC, Cibis GW. Brückner
test. Ophthalmology 1981; 88: 1041-1044.
2.Brückner R. Exakte Strabismusdiagnostik bei 1/2 bis 3 jährigen
Kindern mit einem einfachen Verfahren, dem "Durchleuchtungstest"
[Exact strabismus diagnostic in ½- to
3-year-old children with
easy method, the "transillumination test"] German. Ophthalmologica
1962; 144: 184-198.
3.Hirschberg J. Beiträge zur Lehre
vom Schielen und von der Schieloperation Contributions to the doctrine of the squint and squint
surgery] German. Zentralblatt für
praktische Augenheilkunde 1886; 10: 5-9.
4.Barry JC. Hier irrte Hirschberg: Der richtige Winkelfaktor
beträgt 12o/mm Hornhautreflexdezentrierung. Geometrisch-optische
Analyse verschiedener Methoden der Strabismometrie [The correct angle factor is
12 degrees pro mm corneal reflex decentration. Geometric optical analysis of
various methods in strabismometry] German. Klinische Monatsblätter für Augenheilkunde 1999; 215: 104-113.
5. Brückner R. Praktische Übungen mit dem Durchleuchtungstest zur
Frühdiagnose des Strabismus [Practical use of the illumination test in the
early diagnosis of strabismus] German. Ophthalmologica
1965; 149: 497-503.
6.Gräf M, Jung A.
The Brückner test: extended distance improves sensitivity for ametropia. Graefes
Archive for Clinical and Experimental Ophthalmology 2008; 246: 135-141.
7.Donahue SP.
Relationship between anisometropia, patient age, and the development of
amblyopia. Transactions of the American Ophthalmological Society 2005;
103: 313-336.
8. Paysse EA, Williams GC, Coats DK.
Detection of red reflex asymmetry by pediatric residents using the Brückner
reflex versus the MTI photoscreener. Pediatrics 2001; 108: 1-7.
9. Miller JM, Hall HL, Greivenkamp
JE, Guyton DL. Quantification
of the Brückner test for strabismus. Investigative Ophthalmology and Visual
Science 1995; 36: 897-905.
10.Roe LD, Guyton DL.
The light that leaks: Brückner and the red reflex. Survey of Ophthalmology
1984; 28: 665-670.
11. Roe LD, Guyton DL.
An ophthalmoscope is not a retinoscope. The difference is in the red reflex. Survey
of Ophthalmology 1984; 28: 405-408.
12.Archer SM. Developmental
aspects of the Brückner test. Ophthalmology 1988; 95:1098-1101.
13.Gole GA, Lisa, Douglas LM.
Validity of the Brückner reflex in the detection of amblyopia. Australian
and New Zealand Journal of Ophthalmology
1995; 23: 281-285.
14. Griffin JR, Mclin LN, Schor CM. Photographic
method for Brückner and Hirschberg testing. Optometry and Vision Science
1989; 66: 474-479.