ABSTRACT
Objectives: To evaluate Ahmed
Glaucoma Valve Implantation at King
Hussein Medical
Center. Indications,
outcomes, and complications were investigated.
Methods: The medical records of all patients who
had Ahmed Glaucoma Valve Implant surgery at King Hussein
Medical Center
during the period between August 2006 and January 2009 were retrospectively
reviewed. A total of 50 cases were
enrolled in this study. A specially designed medical record abstract form was
used to collect the following
data: type of glaucoma, visual acuity, intraocular pressure, number of
medications, and postoperative complications. Simple descriptive statistics
(frequency, mean, percentage) were used to describe the study variables
Results: The mean age of patients was 54.3 ± 2.1
years (range 1.3 to 79.9 years). Types of glaucoma included uveitic glaucoma, paediatric
glaucoma, aphakic/ pseudophakic glaucoma, neo-vascular glaucoma, traumatic
glaucoma and previous failed trabeculectomy. The mean follow-up duration was 16.6 ± 1.7 months (range 9.8 months
to 26.1 months). The mean intraocular pressure before surgery was 28.6
mm and 14.2 mmHg after surgery. The mean number of eye drops used by patient was
3.8 ± 0.4 (range 1 to 4) and 1.1 ± 0.2 (range 0 to 3) before and
after surgery respectively. Transient postoperative hypotony with shallow
anterior chamber occurred in 8 patients. Encapsulated bleb occurred in 5
patients. Revision of the procedure was performed in 3 cases. Endophthalmitis
was not encountered in our series.
Conclusion: Results of Ahmed Glaucoma Valve Implantation surgery at King Hussein
Medical Center
showed that it is safe and effective procedure for treating refractory
glaucomas.
Key words: Ahmed valve, Encapsulated
bleb, Implant and refractory glaucoma.
JRMS
March 2012; 19(1): 20-24
Introduction
Glaucoma can lead to devastating visual loss if not
adequately controlled. There are cases
of refractory glaucoma that do not respond to medical treatment or
trabeculectomy. Examples include paediatric, uveitic, neo-vascular, traumatic,
aphakic/ pseudophakic glaucoma and previous failed trabeculectomy. Glaucoma
drainage implants are useful alternatives in treating refractory glaucomas.(1-5) Among these implants is Ahmed Glaucoma Valve
Implantation.
The Ahmed glaucoma valve was introduced in
1993. It provides resistance to the aqueous outflow compared to
traditional trabeculectomy. A folded silicone membrane forms the valve that opens at
certain intraocular pressure level, thus draining aqueous from the anterior or
posterior chamber to an extra-scleral device that maintains a fibrous bleb
through which filtration can occur.(6) An advantage of this
mechanism is a decrease in the reported occurrence of postoperative hypotony
compared to previous implants.(7-8) However, complications may occur such as tube
obstruction by inflammatory debris, diplopia and tube erosion.(9-10)
Other complications that may occur after any filtering surgery may
also occur such as hyphaema, cataract, corneal decompensation, choroidal
and retinal detachments and failure of the procedure.
The aim of the study was to
evaluate Ahmed Glaucoma Valve Implantation experience at King Hussein
Medical Center.
Indications, outcomes and complications were investigated.
Methods
The medical records of all patients who had
Ahmed Glaucoma Valve Implant surgery at King Hussein
Medical Center
during the period between August 2006 and January 2009 were retrospectively
reviewed. A total of 50 cases were
enrolled in this study. A specially designed medical record abstract form was
used to collect the following
data: type of glaucoma, visual acuity, intraocular pressure, number of
medications, and postoperative complications. Simple descriptive statistics
(frequency, mean, percentage) were used to describe the study variables. A total of 50 cases were enrolled in this
study. Data collected included: type of glaucoma, visual acuity, intraocular
pressure, number of medications, and postoperative complications. Results from our data collection were
compared to other studies from literature.
Ahmed Glaucoma Valve itself consists of a
silicone tube with an outer diameter of 0.635 mm and an inner diameter of 0.305
mm connected to a polypropylene or silicone plate with surface area of 184 mm2.
(11)
Although all surgical procedures were
performed by the same surgeon, patients’ examination and follow-up were performed
by a team of ophthalmologists. A fornix-based conjunctival flap was performed
in the supero-temporal or supero-nasal quadrant. The valved implant was
irrigated by balanced salt solution through the tube using 27-gauge cannula and
then was tucked posteriorly into the inter-muscular sub-Tenon’s space and sutured
to sclera via 9-0 Prolene sutures through the anterior positional holes of the
plate, with the anterior border placed 8 mm posterior to the limbus. The tube was
cut and bevelled up to permit its extension 2 to 3mm into the anterior chamber. The anterior
chamber was entered through the cauterized limbal area with a 23-gauge needle
1.5 mm posterior to the limbus and parallel to the iris plane. The tube was
inserted into the anterior chamber via the needle track using special designed
tube insertion forceps and secured to the sclera with a loose 10-0 Nylon
suture. The tube was covered with a rectangle of preserved sclera of
approximately 5x7 mm.(2) The conjunctiva was sutured back to
its original position using 8-0 Vicryl sutures. Sub-conjunctival steroids and
antibiotics were injected at the completion of the procedure in a quadrant away
from the surgical site. Postoperative topical steroid-antibiotic and
cycloplegic preparations (prednisolone acetate 1%, ofloxacin, cyclopentolate
eye drops) were prescribed for the first several weeks.
Results
Table I summarizes the results of our
study. The mean age of patients was 54.3
± 2.1
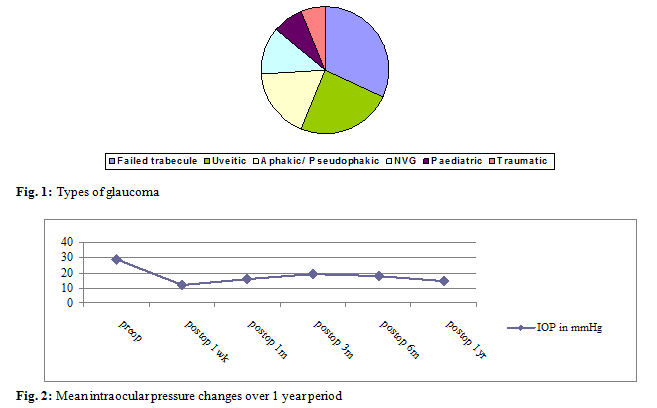
years (range 1.3 to 79. 9 years). Types of glaucoma included failed
trabeculectomy, uveitic, aphakic/pseudophakic, neo-vascular, paediatric and
traumatic glaucoma as presented in (Fig. 1). The mean follow up duration was 16.6 ± 1.7 months (range 9.8 to 26.1 months). The mean intraocular pressure before
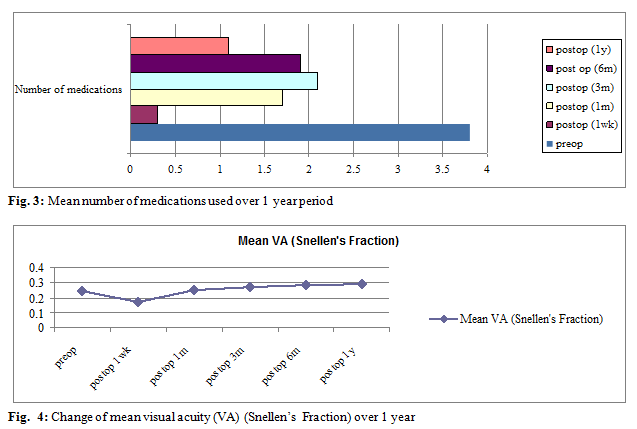
surgery was 28.6 mm and 14.2 mmHg after surgery (Fig. 2). The mean number of eye drops used by patient
was 3.8 ± 0.4 (range 1 to 4) and 1.1 ± 0.2 (range 0 to 3) before and
after surgery respectively (Fig. 3). Transient postoperative hypotony with
shallow anterior chamber occurred in 8 patients. Encapsulated bleb occurred in 4
patients. Revision of the procedure was performed in 3 cases. Of these 3 cases, Intra Ocular Pressure (IOP)
was controlled in 2 patients after revision and the other case received another
implant. Endophthalmitis was not encountered in our series. Table II shows the
complications that occurred in our series. Success rate was 90% and was defined
by IOP between 5-21 mmHg with or without medication, no further glaucoma
surgery, no devastating complications, and no loss of light perception. These
four criteria were also used by Huang MC et al(13) to define success rate.
In our series, the most common indication for Ahmed implant surgery was
previous failed trabeculectomy (16 eyes representing 32%) followed by uveitic
(24%), aphakic/ pseudophakic (18%), neo-vascular (12%), paediatric (8%) and
traumatic glaucoma (6%) (Fig. 1).
Table I. Summary of the study results including
demographic and clinical characteristics
|
Number of patients
|
50
|
|
Number of eyes
|
50
|
|
Follow up (mean and range)
|
16.6 months
|
|
Age range and mean
|
1.3-79.9 years, 54.3 years
|
|
Gender male: female
|
27:23
|
|
Intraocular pressure (preoperative and one year
postoperative)
|
28.6 mmHg → 14.2 mmHg
|
|
Mean Visual acuity in Snellen’s fraction
(preoperative and one year postoperative)
|
0.24 → 0.29
|
|
Mean number of medications (preoperative and one
year postoperative)
|
3.8→ 1.1
|
Table
II. Complications
of the procedure
|
|
No.
|
%
|
|
Transient hypotony
|
8
|
16
|
|
Progression of cataract
|
6
|
12
|
|
Encapsulated bleb
|
4
|
8
|
|
Uveitis
|
3
|
6
|
|
Choroidal detachment
|
5
|
10
|
|
Retinal detachment and loss of
vision
|
1
|
2
|
|
Revision of procedure
|
3
|
6
|
|
Diplopia
|
1
|
2
|
|
Correctopia
|
1
|
2
|
|
Tube touching iris
|
1
|
2
|
|
Dellen ulcer
|
1
|
2
|
Discussion
Glaucoma drainage implants had been used
successfully for the treatment of refractory glaucomas such as previous failed
trabeculectomy, uveitic, neo-vascular, traumatic, aphakic/ pseudophakic, post
penetrating keratoplasty, and paediatric glaucoma and irido-corneal endothelial
syndrome.
Our retrospective analysis showed high success rate for Ahmed Glaucoma Valve Implantation
which was comparable to other studies in the literature.(6,12-13)
The success rate of our series was 90%. Only 5 cases out of 50 showed failure. Four
eyes had encapsulated bleb, 3 of them had procedure revision and the fourth eye
received Diode Laser cyclophotocoagulation. The fifth case had loss of vision.
This case was complicated by choroidal detachment and vitreous haemorrhage and
eventually no light perception vision. All the three cases who their procedure
revised showed good control in the first three months after surgery. Later on,
intraocular pressure started to increase and became resistant to medications.
Encapsulated bleb was seen in all patients. The types of glaucoma in those
patients were pseudophakic, traumatic and neo-vascular. In order to decrease
the frequency of procedure failure, local steroids were used postoperatively.
Proper control of predisposing factor such as uveitis in uveitic glaucoma
increased the incidence of success rate.
Figure
2 demonstrates the changes of intraocular pressure over a one year period.
There was a dramatic drop of IOP in the first week postoperatively (28.6 mmHg
to 11.6 mmHg) that was followed by a hypertensive phase till 3-6 months
(11.6 mmHg to 18.7 mmHg), after that the IOP started to drop again (18.7 mmHg
to 14.2 mmHg, Fig. 2). The number of eye drops used also showed changes similar
to IOP change over a one year period (3.8 drops to 1.1 drops, Fig. 3). In addition, the drop of mean visual acuity in
the first week postoperatively may be due to hypotensive phase (Fig. 4). Huang MC et al(13)
conducted a study on 159 eyes and found a drop of IOP from 32.87 mmHg
preoperatively to 15.9 mmHg postoperatively with a decrease of number of eye
drops used from 2.7 to 1.1 drops and a success rate of 84%. Another study conducted
by Lai and his colleagues(6) on 65 eyes showed reduction of
IOP from 37 mmHg to 16.1 mmHg after Ahmed Glaucoma Valve surgery and a success
rate of 73.8%. The period of transient elevation of intraocular
pressure, termed the “hypertensive phase”, has been described after glaucoma
drainage implant surgery, appearing approximately 4 weeks after surgery and lasting
at least 12
to 16 weeks.(14-15) The hypertensive phase may be transient in some
patients. It is also claimed that its presence early in the
postoperative period may be associated with an unfavourable outcome
and most of these eyes may need continuing medical therapy. The
hypertensive phase is thought to be more frequent with the Ahmed valve because of
its reduced surface area.
Table II illustrates the complications we
encountered in our patients. Transient hypotony being the most common (16%),
progression of cataract occurred in 6 eyes (12%), encapsulated bleb in 8%. Uveitis
occurred
in 3 patients;
all of them had uveitic glaucoma. The procedure was revised in 3 patients. One patient had diplopia that was corrected by spectacles, and one patient had tube eroding the iris that did not require intervention. There was no case of tube eroding the cornea or endophthalmitis. Endophthalmitis was reported to occur in 0.8% to 6.3% of patients.(16-17)
Conclusion
Results for Ahmed Glaucoma Valve Implantation surgery
at King Hussein Medical
Center showed that it is
safe and effective procedure for treating refractory glaucomas.
References
1.Englert
JA, Freedman SF, Cox TA. The Ahmed valve in refractory paediatric glaucoma. Am J
Ophthalmol 1999; 127: 34-42.
2.Sidoti PA,
Minckler DS, Baerveldt G, et al. Epithelial
ingrowth and glaucoma
drainage implants. Ophthalmology 1994; 101: 872-875.
3.Susanna
R. Partial
Tenon’s capsule resection with adjunctive mitomycin C in Ahmed glaucoma valve
implant surgery. Br J Ophthalmol 2003; 87:
994-998.
4.Mata DA, Burk SE, Netland PA, et al. Management of Uveitic
Glaucoma with Ahmed Glaucoma Valve Implantation. Ophthalmology 1999;
106: 2168-2172.
5.Kirwan C,
O’Keefe M, Lanigan B, et al. Ahmed valve drainage implant surgery in the
management of paediatric aphakic glaucoma. Br J Ophthalmol 2005;
89: 855-858.
6.Lai JS, Poon AS, Chua JK, et al. Efficacy
and safety of the Ahmed
glaucoma
valve
implant in Chinese eyes with complicated glaucoma. Br J Ophthalmol 2000; 84: 718-721.
7.Lim KS, Allan BDS, Lloyd AW, et
al. Glaucoma drainage devices; past, present, and future. Br J
Ophthalmol 1998; 82: 1083-1089.
8.Coleman AL, Hill R, Wilson MR,
et al. Initial
clinical experience with the Ahmed glaucoma valve implant. Am J Ophthalmol
1995; 120:23-31.
9. Feldman RM, El-Harazi SM,
Villanueva G. Valve membrane adhesion as a cause of Ahmed glaucoma valve failure.
J Glaucoma 1997; 6: 10-12.
10.
Khan AO, Al-Mobarak
F.
Complications and 2-year valve survival following Ahmed valve implantation
during the first 2 years of life. Br J Ophthalmol 2009; 93: 795-798.
11. Ishida K, Mandal AK, Netland PA. Glaucoma drainage implants in pediatric patients. Ophthalmol
Clin N Am 2005; 18: 431-442.
12. Tran D, Souza C, Ang M et al. Comparison
of Long-Term Surgical Success of Ahmed Valve Implant versus Trabeculectomy in
Open-Angle Glaucoma. Br J Ophthalmol 2008;150870.
13. Huang MC, Netland PA, Coleman AL, et al. Intermediate-term clinical experience
with the Ahmed glaucoma valve implant. Am J Ophthalmol 1999; 127: 27-33.
14.Fellenbaum PS, Almeida AR,
Minckler DS et al.
Krupin disk implantation for complicated glaucoma. Ophthalmology 1994;
101: 1178-1182.
15.Smith MF, Sherwood MB, McGorray SP. Comparison of the double-plate Molteno drainage
implant with the Schocket procedure. Arch Ophthalmol 1992; 110:
1246-1250.
16. Al-Torbak
AA, Al-Shahwan S, Al-Jadaan I, et al. Endophthalmitis associated
with the Ahmed glaucoma valve implant. Br J Ophthalmol
2005; 89 (4): 454-458.
17. Nguyen
QH, Budenz DL, Parrish RK. Complications of Baerveldt glaucoma
drainage implants. Arch Ophthalmol 1998; 116: 571-575.