Abstract
Objective:To compare the histopathological characteristics of
acquired cholesteatoma in adults, children and recurrent cases.
Methods:A retrospective analysis of 60 histopathological specimens
for 60 patients aged 9 to 63 years who underwent otologic surgery
for chronic otitis media with cholesteatoma was carried out at King Hussein
Medical Centre between January 2006 till July 2010. Patients were divided into three groups as follows; group A patients
aged > 16 years with no history of previous ear surgery, group B patients
aged > 16 years and had history of previous otologic surgery for
cholesteatoma and group C patients aged ≤ 16 years. Histopathological analysis was performed for specimens.
Results for group A were compared with
results of groups B & C separately.
Results:After histopathological analysis; atrophy was present
in 26(84%) specimens in group A, 10 (71%)specimens in group B and 11(73%)
specimens in group C. Twenty-
seven (87%) specimens had acanthosis in
group A, and , 13 specimens (93%)
in group B and 12 (80%) in group C. Basal . Basal cell hyperplasia was present in 29 (94%) specimens in group
A, 100% of group B, and 97% of group C. Epithelial cones were present in 20 (65%), 10 (71%), and 10
(67%) of our study groups respectively. Peri- matrix inflammation was present
in 30(97%) of group A and 100 % of both groups B and C. Results showed that there were no statistically
significant differences between our study groups.
Conclusion:Although the sample size in this study was small but
the statistical analysis showed that the histopathological characteristics of
acquired cholesteatomas did not differ significantly between adults, children
and recurrent cases. The characteristics of the peri-matrix should be analyzed
more, especially in children to find if there is correlation with the behavior
and aggressiveness of the disease.
Key words: Cholesteatoma, Histopathology, Recurrent cases.
JRMS
March 2012; 19(1): 41-45
Introduction
Cholesteatomas are benign epidermally-derived temporal
bone lesions that are locally destructive and frequently recurrent.
Cholesteatomas cause temporal bone destruction due to mechanical pressure,
enzymatically mediated bone resorption, and promotion of acute and chronic
infections.(1,2) The growth of keratinocytes in the epidermis
is regulated by a delicate balance between molecules that control cell survival
and cell death. If this regulation is disturbed, epithelial cells may become
pathological hyper-proliferative lesions, such as cholesteatoma.(3) Cholesteatoma
has altered growth properties compared with the normal epidermal epithelium. It
is characterized by an excessive growth of keratinocytes that leads to mucosal
destruction.(4) The molecular and cellular processes
resulting in the clinical hallmarks of cholesteatomas (i.e., migration,
uncoordinated proliferation, altered differentiation, and aggressiveness) are
not yet fully understood.(5) Annual incidence of
cholesteatoma ranges around 3 in 100,000 in children and 9.2 in 100,000 in
adults, and it is more predominant in male.(6,7) There are no medical therapies for
cholesteatoma and current treatment is surgical resection. Recurrences are
common and many individuals with cholesteatoma undergo multiple operations.(8,9)
Histologically, the cholesteatomas consist of keratinized squamous stratified
epithelium (matrix), with four layers identical to those of thin skin (basal,
squamous, granulous, and stratum corneum), lying on a bed of connective tissue
(peri-matrix).(10) According to Sudhoff H, the
matrix is enclosed in a thin layer of connective tissue called the peri-matrix.(11)
This is separated from adjacent bone by an inflammatory infiltrate
which plays a decisive role in the potential spread of the cholesteatoma.(12,13)
Cholesteatomas have hyperproliferating characteristics (14)
with epithelial acanthosis, hyperplasia of the basal layer and the presence of
epithelial cones in the matrix. This
study was conducted to compare the histopathological characteristics of
acquired cholesteatoma in adults, children and recurrent cases.
Methods
A retrospective analysis of 60
histopathological specimens for 60 patients aged 9 to 63 years who underwent
otologic surgery for chronic otitis media with cholesteatoma was carried out. Ethical
Committee Approval was obtained. This study was conducted at King Hussein
Medical Centre (KHMC) for the period January 2006 till July 2010. Exclusion criteria
included: absence of cholesteatoma matrix or perimatrix in the specimen and cases
which were diagnosed as congenital cholesteatoma. Patients were divided into
three groups as follows; group A patients aged > 16 years with no history of
previous ear surgery, group B patients aged > 16 years and had history of previous
otologic surgery for cholesteatoma and group C patients aged ≤ 16 years.
Histopathological analysis was performed for specimens which were processed by routine histopathological
techniques that included; 10% formaldehyde fixation, embedding in paraffin,
cutting using the microtome, placing
tissue sections on the slides and staining them with Hematoxylin and
Eosin (H+E stain), and finally light microscopic examination. One serial number
was used for each case. In our analysis five histopathological features were
evaluated for these cases which were: atrophy
which is defined as matrix with thickness of up to 4 keratinocyte layers, basal
layer hyperplasia, acanthosis, epithelial cone formation, and perimatrix
inflammation. Histopathological findings were assessed as absent or present and
graded according to intensity as focal or predominantly atrophic for the first
variant, and graded as mild, moderate and severe for acanthosis, basal layer
hyperplasia and perimatrix inflammation. Results for group A were compared with
results of groups B and C separately.
Statistical analyses were performed with Statistical Package for Social Science - SPSS
for Windows, using t-test and Fisher's exact tests when appropriate. All data are expressed as the mean ± standard
deviation (SD). A value of P<0.05 was considered statistically
significant.
Results
The patient's data was comparable between group A and
B for age and gender (p < 0.05). Group A composed of 31 patients of whom 16(52%)
were males and 15(48%) females; the mean age was 32.4 ± 17.2 years. Group B
composed of 14 patients of whom 8(57%) were males and 6(43%) were females; the
mean age was 31.3 ± 14.6 years. Group C composed of 15 patients of whom 7(47%)
were males and 8(53%) were females; the mean age was 12.8 ± 2.3 years, (Table I).
After histopathological
analysis; atrophy was present in 26(84%) specimens in group A, 10(71%) specimens
in group B, and 11(73%) specimens in group C. The degree of atrophy was as
follows; in group A, 10 (38%) was focal and 16 (62%) was predominant. In group B, 4 (40%) was focal and
6 (60%) was predominant. In
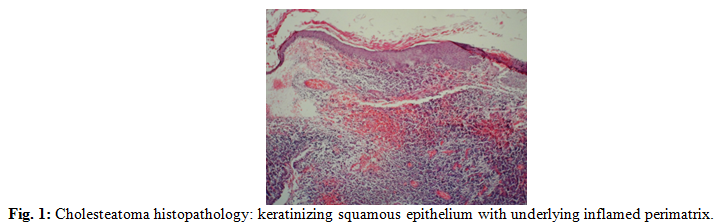
group C, 4 (36%) was focal and 7 (64%) was predominant. Twenty- seven (87%) specimens have acanthosis in group A, of which 8 (30%) were mild, 10 (37%) were moderate and 9 (33%) were severe. It was absent in 4 (13%) specimens. In group B, acanthosis was present in 13(93%) specimens and the degree was mild in 3 (23%), moderate in 6 (46%) and severe in 4 (31%) specimens, it was absent in 1(7%) specimen. In group C, acanthosis was present in 12 (80%) and absent in 3 (20%) of the specimens, the degree was mild in 3 (25%), moderate in 6 (50%) and severe in 3 (25%) of the specimens. Basal cell hyperplasia was present 29(94%) specimens in group A, 14 (48%) had mild degree, 11 (38%) had moderate and 4 (14%) had severe degree. In group B; all specimens had basal cell hyperplasia, 50% was mild, 5 (36%) had moderate and 2 (14%) had severe degree while in group C it was present in 14 (93%), absent in 1 (7%) and the degree was mild in 6 (43%), moderate in 5 (36%) and severe in 3 (21%) specimens. Epithelial cones were present in 20 (65%), 10(71%) and 10 (67%) of our study groups respectively. Perimatrix inflammation was present in 30 (97%) of group A, 14 (47%) had mild degree, 9 (30%) had moderate and 7 (23%) had severe degree of inflammation. In group B, inflammation was present in all specimens examined (Fig. 1), 6 (43%) had mild degree, 5 (36%) had moderate degree and 3 (21%) had severe degree of inflammation. In group C, perimatrix inflammation was also found in all examined specimens, and the degree of inflammation was mild in 1 (7%) specimen, moderate in 3 (20%) and severe in 11 (73%) of the examined specimens. Table II represents the histopathological findings and statistical analysis of the study groups results showed that there were no statistically significant differences between the three study groups.
Table I:
Demographic data of the study groups
|
|
Group A
|
Group B
|
Group C
|
P value
A versus B
|
P value
A versus C
|
|
Age Year
|
32.4 ± 17.2
|
31.3 ± 14.6
|
12.8 ± 2.3
|
0.836
|
<0.001
|
|
Gender M:F
|
16:15
|
8:6
|
7:8
|
0.492
|
0.500
|
|
Total number
|
31
|
14
|
15
|
|
|
Table II: Histopathological findings in the study
groups
|
Histopathological feature
|
Group
A
|
Group
B
|
Group
C
|
P value
A & B
|
P value
A & C
|
|
Atrophy
|
Absent
|
5
(16%)
|
4
(29%)
|
4
(27%)
|
0.280
|
0.312
|
|
|
Present
|
26
(84%)
|
10
(71%)
|
11(73%)
|
|
Acanthosis
|
Absent
|
4 (13%)
|
1
(7%)
|
3
(20%)
|
0.496
|
0.619
|
|
|
Present
|
27 (87%)
|
13
(93%)
|
12
(80%)
|
|
Epithelial cones
|
Absent
|
11 (35%)
|
4
(29%)
|
5
(33%)
|
0.461
|
0.578
|
|
|
Present
|
20 (65%)
|
10
(71%)
|
10
(67%)
|
|
Basal layer
|
Absent
|
2 (6%)
|
0
|
1
(7%)
|
0.468
|
0.701
|
|
Hyperplasia
|
Present
|
29 (94%)
|
14(100%)
|
14
(93%)
|
|
Perimatrix
|
Absent
|
1 (3%)
|
0
|
0
|
0.689
|
0674
|
|
Inflammation
|
Present
|
30 (97%)
|
14(100%)
|
15(100%)
|
|
Total No.
|
|
31
|
14
|
15
|
|
|
Discussion
Cholesteatomas were defined by Schuknecht (15)
as the accumulation of exfoliated keratin in the middle ear or any pneumatized
area of the temporal bone, deriving from a keratinized squamous
epithelium. And it should be differentiated
from congenital cholesteatoma which presents early in life as a white pearly
mass behind an intact tympanic membrane.(16,17) It may affect
both children and adults, but there is controversy about its clinical behavior
in the different age ranges in which it is manifested; Dornelles et al,(18) draw an analogy between the perimatrix and a
“battlefield”, where there is a fight for the middle ear territory, between
the cholesteatoma matrix itself and the
adjacent tissues of the tympanic box. With the expansion of cholesteatoma, the
inflammatory reaction would increase and therefore, it would produce more
elements of the inflammatory cascade. TNF-α is found in cholesteatomas,
promoting bone resorption by different routes. It acts on osteoclast
differentiation and maturation and also exposes the bone matrix.(19)
Ferlito et al(20) described the perimatrix as the most
peripheral portion of the cholesteatoma, comprising granulation tissue or
inflammatory subepithelial connective tissue, with lymphocytes, histiocytes and
neutrophils.(21) Aural cholesteatomas vary in progression and
aggressiveness; the presence of bacterial biofilms in some cholesteatomas may
explain their activity. (22)
By the histological analysis of cholesteatomas,
Dornelles(23) found an inverse correlation between the
perimatrix size measured in micrometers and the age of patients at the day of
surgery and that the degree of the perimatrix inflammation was strongly
correlated with the perimatrix thickness. According to different authors,(24-26)
pediatric cholesteatoma is less expansive, which leads to lower incidence of
complications. Conversely, others(27-31) reported that acquired
cholesteatoma in children should be presented in a more aggressive way and with
more extensive growth. In our study we have not found any histopathological
differences between cholesteatoma specimens of adults and children on one hand,
and between specimens of adults who have first time surgery and those with
revision surgeries. These results are comparable to what Dornelles and her
colleagues (32) and Leal Alves et al (13)
have found. We have noticed the higher
intensity of perimatrix inflammatory response in children compared to adults
but we failed to show statistically significant difference as Dornelles(23)
did. Quaranta et al(33) proposed that the
characteristics of the perimatrix may play an important role in the
pathogenesis of the cholesteatoma, suggesting that these histo-morphological
characteristics would influence the recurrence and invasion of pediatric cholesteatomas.
Dornelles and colleagues indicated
that not only the perimatrix is more active in
pediatric cholesteatomas, but also that the matrix would have a more active
proliferation either current or past,(32) and their findings
corroborate the hypothesis from Bujia et al(29) who
suggested that pediatric cholesteatomas would present a more pronounced
proliferative state. The aggressiveness of pediatric cholesteatomas may be also
related to the histology of pediatric bone.
Conclusion
Although the sample size in
this study was small but the statistical analysis showed that the
histopathological characteristics of acquired cholesteatomas did not differ
significantly between adults, children and recurrent cases. The characteristics
of the perimatrix should be analyzed more, especially in children to find if
there is correlation with the behavior and aggressiveness of the disease.
References
1. Friedland DR, Eernisse R, Erbe
C, et al. Cholesteatoma
growth and proliferation: post-transcriptional regulation by microRNA-21.
Otol Neurotol 2009; 30(7): 998-1005.
2. Shin SH, Shim JH, Lee HK. Classification of external auditory canal cholesteatoma
by computed tomography. Clin and Exp Otorhinolaryngol, 2010; 3(1):
24-26.
3.Kojima H, Tanaka Y, Tanaka T,
et al. Cell Proliferation and apoptosis
in human middle ear cholesteatoma. Arch Otolaryngol Head Neck Surg.
1998; 124: 261-264.
4.Mallet Y, Nouwen J, Lecomte-Houcke
M, et al. Aggressiveness and quantification of epithelial proliferation
of middle ear cholesteatoma by MIB1. laryngoscope, 2003; 113:328–331.
5.Byun JY, Yune TY, Lee JY, et
al. Expression of CYLD and NF-kappaB
in human cholesteatoma epithelium. Mediators of inflammation 2010; 2010:
796315.
6.Tos M. Cholesteatoma in children: long term results. In Tos
M, ed. Cholesteatoma and mastoid surgery. Amsterdam
Berkeley, Milano: Kugler and Ghedini; 1989: 677-683.
7.Olszewska E, Wagner M,
Bernal-Sprekelsen M, et al.
Etiopathogenesis of cholesteatoma. Eur Arch Otorhinolaryngol 2004;
261(1): 6-24.
8.Mukherjee P, Saunders N, Liu
R, Fagan P. Long-term outcome of
modified radical mastoidectomy. J Laryngol Otol 2004; 118: 612-616.
9.Yung M, Jacobsen NL, Vowler
SL. A 5-year observational study of
the outcome in pediatric cholesteatoma surgery. Otol Neurotol 2007;
28:1038-1040.
10.Lim DJ, Saunders WE. Acquired cholesteatoma: light and electron
microscopic observations. Ann Otol Rhino Laryngol 1972; 81(1): 1-11.
11.Sudhoff H, Tos M. Pathogenesis of attic cholesteatoma: clinical and
immunohistochemical support for combination of retraction theory and
proliferation theory. Am J Otol 2000; 21(6): 786-792.
12.Schuknecht HF. The pathology of the
ear. Cambridge: Harvard University,
1974.
13.Alves
AL, Pereira CS, Ribeiro FA, et al. Analysis of histopathological
aspects in acquired middle ear cholesteatoma. Braz J Otorhinolaringol 2008; 74(6):835-841.
14.Naim R, Sadick H, Bayerl C, et al. Angiogenic factors in external
auditory canal cholesteatoma-fibroblast cell culture. HNO 2005; 53(11): 952-956
15.Dornelles C, Costa SS, Meurer
L, et al. Correlation
of cholesteatomas perimatrix thickness with patient’s age. Braz J Otorhinolaringol
2005 71(6): 792-797.
16. Isaacson G. Diagnosis of Pediatric Cholesteatoma. Pediatrics
2007; 120(3); 603-608.
17.Koltai PJ, Nelson M, Castellon
RJ, et al. The Natural History of Congenital
Cholesteatoma. Arch Otolaryngol Head Neck Surg. 2002; 128: 804-809.
18.Dornelles C, Rosito LPS,
Meurer L, et al.
Hystology findings’ correlation between the ossicular chain in the
transoperative and cholesteatomas. Braz J Otorhinolaringol 2007;
73(6):738-743.
19.Vitale RF, Ribeiro FAQ. The role of Tumor Necrosis Factor -Alpha (TNF-α) in
bone resorption present in middle ear cholesteatoma; Braz J Otorhinolaringol
2007; 73(1):117-121.
20.Ferlito O, Devaney KO, Rinaldo
A, et al. Clinicopathological
consultation. Ear cholesteatoma versus cholesterol granuloma. Ann Otol
Rhinol Laryngol 1997; 106(1): 79-85.
21.Popescu C, Ionita E, Mogoanata
CA, et al. Clinical and histopathological aspects
in otomastoiditis. Rom J
Morphol Embryol 2009; 50(3):453–460.
22.Chole RA, Faddis BT. Evidence for Microbial Biofilms in Cholesteatomas. Arch
Otolaryngol Head Neck Surg 2002; 128(10): 1129-1133.
23.Dornelles C, Costa SS, Meurer L, et al. Some consideration about
acquired adult and pediatric cholesteatomas. Braz J Otorhinolaringol
2005; 71(4): 536-546
24.Sheehy JL. Management of cholesteatoma in children. Adv
Oto-Rinolaryngol 1978; 23: 58-64.
25.Tos M. Treatment of cholesteatoma in children: A long-term
study of results. J Otol 1983; 4: 189-197.
26.Edelstein DR, Parisier SC, Han JC. Acquired Cholesteatoma in Pediatric Age Group. The
Otolaryngol Clin North Am 1989; 22(5): 955-64.
27.Glasscock ME, Dickins JFE,
Wiet R. Cholesteatoma in children. Laryngoscope
1984; 91(10): 1743-1753.
28.Ruah CB, Schachem PA,
Paparella MM, Zelterman D. Mechanisms
of retraction pocket formation in the pediatric tympanic membrane. Arch Otolaryngol
Head Neck Surgery 1992; 118(12): 1298-1305.
29.Bujia J, Holly A,
Antoli-Candela F, Tapia MG, et al. Immunobiological peculiarities of cholesteatoma in
children: quantification of epithelial proliferation by MIB1. Laryngoscope 1996;
106 (7): 865-868.
30.Palva A, Karma P, Kärjä J. Cholesteatoma in children. Arch Otolaryngol 1997;
103(2): 74-77.
31.Sudhoff H, Dazert S, Gonzales
AM, et al. Angiogenesis and
angiogenic growth factors in middle ear cholesteatoma. Am J Otol 2000;
21(6): 793-798.
32.Dornelles C, Meurer L, Costa
SS, Schweiger C. Histologic
description of acquired cholesteatomas: comparison between children and adults.
Braz J Otorhinolaringol 2006; 72(5):641-648.
33.Quaranta A, Resta L,
Santangelo A. Otomastoid
cholesteatoma in children: histopathological findings. Int J Pediatric
Otorhinolaryngol 1986; 12(2): 121-126.