Abstract
Objective: To
evaluate the technical success and primary patency of percutaneous transluminal
angioplasty as a modality of treatment for outflow venous stenosis in arteriovenous
fistulae used as hemodialysis access.
Methods: This is a
retrospective, single center review which was conducted between August 2008 to
August 2009, analyzing the results of percutaneous transluminal angioplasty
used to treat 49 patients with short segment venous outflow stenosis. Patency
was assessed by clinical examination and Doppler ultrasound scanning over a
follow up period of one year.
Results: The immediate technical
success rate of percutaneous transluminal angioplasty was 98%. The primary
patency at six months, and one year were 83% and 53% respectively. One patient
developed rupture of the vein at the site of angioplasty. Six patients died
during the follow up period. The deaths were not related to the procedure or
access failure.
Conclusion: Percutaneous transluminal angioplasty is an
effective method for treatment of venous outflow stenosis in surgically created
arteriovenous fistulae, with excellent technical success, acceptable one year
primary patency, and low complications rate.
Key words: Arteriovenous
fistula, dialysis access, outflow venous stenosis, percutaneous transluminal
angioplasty
JRMS
June 2012; 19(2): 21-24
Introduction
In recent years,
we have been faced with an increasing number of patients who suffer from end
stage renal disease. Such patients require hemodialysis through an access that
offers rapid blood flow of adequate volume.(1) Surgically
created arteriovenous fistulae are commonly used as hemodialysis accesses in
our hospital, because of the decreased incidence of associated complications,
and longer patency compared to arteriovenous grafts.
Dysfunction and
even thrombosis and failure of arteriovenous fistulae are not uncommon, and the
commonest cause of dialysis access dysfunction in general is venous stenosis
caused by neointimal hyperplasia.(2)
Percutaneous
transluminal angioplasty (PTA) offers a relatively minimally invasive, and safe
treatment option which corrects the venous stenosis effectively,(1,3-5)
and prolongs the access patency duration.(6-8) However, for
juxta-anastomotic stenotic lesions within four centimeters from the anastomosis,and long in lesions more than four centimetres in length, surgical intervention is advised.(9)
This is a
retrospective, single centre review, which was conducted at King Hussein
Medical Centre to assess the results of PTA performed to treat 49 significant,
short segment venous outflow stenosis encountered in symptomatic patients.
Methods
During the period
from August 2008 to August 2010, a total of 58 patients with previously
functioning arteriovenous hemodialysis fistulae, were referred to the
interventional radiology service at our institution, with symptoms and signs
related to venous outflow stenosis.
The clinical
presentation included increased venous pressure during dialysis (20 patients),
enlarging venous aneurysm (5 patients), and limb edema (33 patients). Doppler ultrasound was performed for all
patients and confirmed the presence of venous stenosis suggested by the
clinical presentation.
A fistulogram was
performed via a direct venous puncture. A full study of the draining venous
system was performed. A pressure cuff inflated distal to the fistula was used
to occlude the venous drainage temporarily, and a reflux fistulogram was
performed to evaluate the arteriovenous anastomosis, and the arterial supply of
the fistula. Digital subtraction imaging and low osmolar, nonionic contrast was
used in all cases.
Nine patients were excluded from our study
because co-existing juxta-anastomotic stenotic lesion (2 patients), long
segment stenosis in the outflow veins (2 patients), complete occlusion of the
outflow vein (2 patients), or multiple stenosis of the outflow veins (3
patients). The remaining 49 patients (27
males, 22 females), with an age range of 38 to 67 years (mean age of 57 years),
were included in the study. These patients were diagnosed to have single, short
(less than 4 cm), significant venous outflow stenosis, defined as a reduction
of the vessel diameter of more than 50% in relation to the normal vessel
diameter distal to the stenosis.(10,11)
Table I: Technical success and complications among the study
group
|
|
Patients
Number
|
Patients (%)
|
|
Technical Success
|
48
|
98
|
|
Major Complication
|
1
|
2
|
|
Minor Complication
|
2
|
4
|
Table II: Patency results among the study group
|
|
6 Months
|
12 Months
|
|
Number of Patients
|
47
|
43
|
|
Patent Venous Outflow
|
39
|
23
|
|
Failure of Angioplasty
|
8
|
20
|
|
Primary Patency Rate
|
83%
|
53%
|
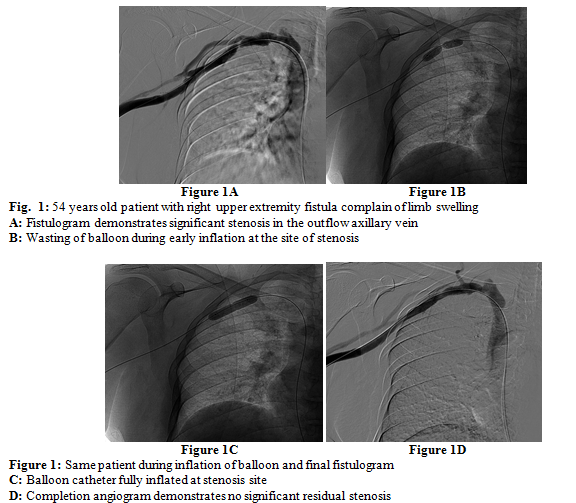
The lesions were
crossed with angled glide, 0.035 inch, hydrophilic coated Guide wire (Terumo
Inc), directed by a 5 Fr multi-purpose catheter (Cordis) (Fig. 1A). All patients received 40 International Units\kg
of Heparin intravenously prior to the dilatation. Angioplasty was performed for
each lesion using the appropriate size balloon dilatation catheter (10% more
than the diameter of the vein proximal to stenosis). The balloon was kept
inflated in place for a period of one minute (Fig. 1B, 1C).
A completion
angiogram was performed to evaluate the immediate result of the intervention (Fig.
1D). Immediate technical success was defined as residual stenosis less than 30%
of the vessel diameter in relation to the normal vessel diameter distal to the
stenosis and without major complications related to the procedure.(10,11)
The procedure
caused tolerable pain and discomfort in 46 patients. Three patients experienced
severe pain and were managed by administering 50 mg of phentanyl intravenously,
under continuous vital signs monitoring as per our institution protocol. Forty-eight
patients received treatment on outpatient basis, were monitored in our recovery
unit for 6 hours following the procedure, and were then discharged without
complications. One patient developed rupture of the vein at the site of
angioplasty and was admitted to the hospital. Two patients developed small
puncture site hematoma that was treated conservatively.
The patients were
followed up at 6 and 12 months by clinical examination tailored to detect any
signs and symptoms of venous ouflow stenosis. Doppler ultrasound scanning was
performed for all patients.
The angiographic
and interventional procedures were performed in the interventional radiology
section. The patients were followed up in the vascular surgery clinic, and Doppler
ultrasound studies were performed in the vascular surgery department.
Results
Technical success
was encountered in 48 patients as documented on their completion fistulogram.
Two patients developed small puncture site hematomas that were treated
conservatively, and did not necessitate admission to the hospital. One patient
developed rupture of the vein at the site of angioplasty and was admitted to
the hospital for surgical management. This patient was discharged after 48
hours, and was considered as a failure of primary angioplasty (Table I).
On follow up, 39
patients remained asymptomatic at six months, and 23 patients at one year.
These patients demonstrated patent outflow by Doppler ultrasound without
significant stenosis (Table II).
Twenty patients
developed recurrence of symptoms during the follow-up period. Doppler scanning done
at that time revealed recurrent stenosis. Thirteen patients were treated successfully
by a second angioplasty (11 patients) or stenting (2 patients), while the other
7 patients failed this further endovascular treatment and were therefore
referred for surgery.
Six out of the
total 49 patients died during the follow-up period, two of them in the firs six
months, due to causes not related to the procedure or access failure.
Discussion
Over the years, surgically created arteriovenous
fistulae have been accepted as efficient long term accesses for hemodialysis in
end stage renal disease patients. A major cause of delayed failure in these
accesses is stenosis affecting the venous side.(1,2) Other
causes include arterial side stenosis, generalized hypotension, extrinsic
compression, trauma, or infection.(1)
Venous outflow stenosis may present with a wide
spectrum of symptoms including persistent edema of the limb, presence of a
pulse without a thrill, inefficacious dialysis, increase in the venous
pressure, or even complete thrombosis of the hemodialysis access.(1,9)
Early detection and treatment of venous stenosis
prevents access thrombosis, and prolongs access patency.(6,7)
In recent years, there has been increasing evidence in literature supporting
the use of PTA as the primary method of treatment for dialysis access stenosis,(4,12)
offering the patients a shorter stay in the hospital, and acceptable success
rates when compared with surgery, in addition to the opportunity to immediately use the same access for dialysis.(1)
Like other medical procedures, PTA can be associated
with complications that can occur during or after the procedure. Major
complications include venous rupture, arterial embolization, symptomatic
pulmonary embolism, puncture site complications necessitating treatment, and
bleeding. Minor complications include non-flow compromising small puncture site
hematoma or pseudoaneurysm formation.(13)
In this study, we have included patients who presented
with symptoms and signs of venous stenosis, in previously functioning,
surgically created arteriovenous fistulae. Those patients who proved to have
focal short segment venous outflow stenosis by Doppler ultrasound, and fistulogram,
were treated with PTA, and were then followed up at six, and 12 months by
clinical examination and Doppler ultrasound scanning.
Patients who had multiple venous stenosis or occlusion
were treated primarily by PTA with or without stenting. Patients who failed
this primary endovascular intervention or those who were having long segment
venous stenosis, or had juxtanastomotic stenosis were referred for surgical
revision. All those patients were excluded from our study.
Our study showed a high technical success rate in treating
short segment venous outflow stenosis. The
follow up demonstrated high primary patency rates at six months (83%) and one
year (53%).
Our study showed that the procedure is relatively safe
with only one major complication (2%), and two minor complications (4%)
encountered. Our results were consistent
with the results of other studies in literature.(1,14)
Conclusion
Percutaneous transluminal angioplasty is an effective,
minimally invasive method for treatment of venous outflow stenosis in
surgically created arteriovenous fistulae, with high technical success,
acceptable one year primary patency, and relatively low complication rates.
References
1.Miquelin D, Reis L, da Silva A, de Godoy J. Percutaneous transluminal angioplasty in
the treatment of stenosis of arteriovenous fistulae for heamodialysis. Int Arch
Med 2008 January 16.
2.Lee T, Roy-Chaudhury P. Advances and new frontiers in the pathophysiology of
venous neointimal hyperplasia and dialysis access stenosis. Adv Chronic
Kidney Dis 2009 September; 16(5): 329–338.
3.Mori Y, Horikawa K, Mimuro N, et al. Stenotic lesions in vascular access:
treatment with transluminal angioplasty using high-pressure balloons. Intern Med 1994 May; 33(5):284-7.
4. Vesely TM. Endovascular intervention for the failing vascular
access. Adv Ren Replace Ther 2002
April; 9(2):99-108.
5.Lio JY, Chiang SS, Chang CH, et al. The efficacy of percutaneous transluminal
angioplasty in the treatment of failing vascular access in chronic
heamodialysis patients. Zhonghua Yi Xue Za Zhi (Taipei). 1996 November; 58(5):335-40.
6.Surlan M, Popovic P. The role of interventional radiology in
management of patients with end-stage renal disease. Eur J Radiol 2003
May; 46(2):96-114.
7.Turmel-Rodrigues, Pengloan J, Bourquelto P. Interventional radiology in heamodialysis
fistulae and grafts: a multidisciplinary approach. Cardiovasc Intervent Radiol
2002 Jan-Feb; 25(1):3-16.
8.Ayez N, Fioole B, Aarts RA, et al. Secondary interventions in patients with
autologous arteriovenous fistulas strongly improve patency rates. J Vasc
Surg 2011; 54-1095-1099.
9.Glanz S, Gordon D H, Butt KM, et al. The role of percutaneous angioplasty in
the management of chronic hemodialysis fistulas. Ann Surg 1987; 206(6):
777–781.
10.National
Kidney Foundation Kidney Diseases Outcomes Quality Initiative Clinical Practice
Guidelines for Vascular Access, 2000. Am J Kidney Dis 2001; 37(suppl 1):S137–S181.
11.Katz D. The role of interventional radiology in a
comprehensive hemodialysis program: The Access Surgeon's View. Semin Intervent Radiol 2004; 21(2): 125–127.
12.Tapping CR, Mallinson Pl, Scott
PM, et al. Clinical
outcomes following endovascular treatment of malfunctioning autologous dialysis
fistula. J Med Imaging Radiat Oncol 2010 December; 54(6):534-540.
13 Kim D, Goo D, Yang
S, et al.
Endovascular management of immediate procedure-related complications of failed
hemodialysis access recanalization. Korean
J Radiol 2005 July-September; 6(3): 185–195.
14.Dougherty MJ,
Calligaro KD, Schindler N, et al. Endovascular versus surgical treatment for thrombosed
hemodialysis grafts: A prospective, randomized study. J Vasc Surg 1999; 30(6):1016-1023.