Abstract
Objectives: To
determine how central corneal thickness in patients with primary open-angle
glaucoma correlates with intraocular pressure diurnal fluctuations. This
study also verifies the effect of positioning (supine or sitting) on intraocular
pressure.
Methods: This
study was conducted on a 38 subjects with mild to moderate primary open
angle glaucoma were recruited and evaluated for 24 hours in a controlled
environment, having their intraocular pressure measured. During the hours of
7:00 AM to 9:00 PM, intraocular pressure was measured in the sitting and supine
positions, while in the hours of 11:00 PM to 5:00 AM they were made in the
supine position only. Patients were maintained on their normal medication
schedules. Baseline information was gathered from clinical charts in addition
to a detailed patient history.
Results: The mean circadian intraocular pressure
fluctuation was 8.8 (3.2) mmHg (p<0.0001). Night time intraocular pressures
were on an average 2.3 (2.6) mmHg higher than day time pressures (p<0.0001).
Daytime supine pressures were significantly higher than sitting by 2.8 (1.1)
mmHg, (p<0.0001), but daytime supine mean IOP 19.9 (4.0) mmHg was lower than
night time supine intraocular pressure of 20.8(4.3), (p=0.04). Intraocular
pressure fluctuations were greater among patients with thinner central corneas.
Inverse relationship was observed between central corneal thickness and daytime
supine intraocular pressure flux (Spearman rho= -0.39, p=0.02) and between central
corneal thickness and night time supine intraocular pressure flux (rho = -0.37,
p=0.02).
Conclusion:
This study has shown that significant
fluctuations in intraocular pressure still occur in clinically controlled
patients with primary open-angle glaucoma. And that those patients with thinner
corneas show greater diurnal intraocular pressure fluctuations than patients
with thicker corneas. Furthermore, supine intraocular pressure measurement may
provide a more clinically relevant picture in those patients, as compared to
sitting pressures.
Key
words: Central corneal thickness, Intraocular
pressure, Primary open angle glaucoma.
JRMS
June 2012; 19(2): 51-55
Introduction
Glaucoma is the second leading cause of blindness
worldwide and in the USA in individuals over the age of 50 years and is expected
to become a major health issue as individuals live longer.(1)
Primary Open-Angle Glaucoma (POAG), which is the most
common type of glaucoma, is considered to be a multifactorial progressive optic
neuropathy with an intricate interplay of both ocular and systemic risk
factors.(2) Intraocular Pressure (IOP) fluctuations and thin Central
Corneal Thickness (CCT) are considered independent risk factors for glaucoma
progression.(3,4) Wide fluctuations in IOP are recognized to
be major factors in the progression of glaucoma.(5) These
fluctuations, including diurnal changes of IOP, may be important considerations
in managing patients with glaucoma. Elevated IOP and CCT are considered powerful
predictors for the development of POAG.
Individuals with thicker corneas have poorer IOP
responses to ocular hypotensive medications than those with normal or thin
corneas.(6,7) But it is unknown if IOP fluctuations are
influenced by CCT.
This study was designed to determine the relationship
of CCT to diurnal IOP fluctuations.
Methods
A total of 38 patients from the UT Southwestern James
W. Aston Ambulatory Care Center with mild to moderate POAG between the ages of
50 and 80 years were recruited for participation in this study.
Inclusion criteria were: typical glaucomatous optic
nerve cupping, corresponding visual field damage (-2 to -12 mean deviation) in
the worse eye, open irido-corneal angles by gonioscopy, reliable Humphrey
visual field tests (fixation losses less than 20%, false positive and false
negative errors less than 30%) and visual acuity of 20/100 or better in the
worse eye. Patients with prior glaucoma surgeries were permitted.
Baseline information was gathered from clinic charts
and a detailed patient history including patient age, gender, race, systemic
medications, systemic illnesses, duration of glaucoma, glaucoma medications,
status of optic nerves including cup-to-disc ratio, past ocular surgeries,
visual acuity, Humphrey visual field, average of last two IOP (Goldmann
Applanation Tonometer, Haag-Streit, Mason, OH) measurements, slit lamp
findings, average nerve fiber layer thickness by ocular coherence tomography or
Heidelberg retinal tomography, and CCT (Corneo-Gage Plus pachymeter, Sonogage
Inc., Cleveland, OH) was also collected.
Patients were admitted two at a time to the General Clinical
Research Center
located in Parkland
Memorial Hospital
on Friday evenings.
The patients were provided with nursing supervision
and full meals (limited free-water intake of 3000 ml for the 24-hours of data
collection and no caffeine or tobacco). They were instructed to take their
medications, both ocular and systemic, at their normal at-home schedule.
After calibration according to manufacturer’s specifications,
IOP measurements were taken during the study using the Mentor Model 30 Classic
Pneumotonometer (Mentor O&O, Inc., Norwll,
MA). IOP measurements were
performed bi-hourly from 7:00 AM on Saturday till 7:00 AM the next day. Three
measurements were made each time on each eye and then averaged. The right eye
was always measured first. Topical 0.5% proparcaine was used for anesthesia.
During daytime hours of 7:00 AM to 9:00 PM, IOP was
measured in the sitting and supine positions. During night time hours of 11:00
PM to 5:00 AM, IOP measurements were made in the supine position only.
The POAG patients were compared with two-sample
t-tests for continuous variables and Fischer’s Exact test for categorical
variables. Comparisons within subjects (e.g., day versus night) were made with
paired t-tests. Spearman correlation coefficients were used to assess the
association between CCT and IOP circadian fluctuations.
Results are expressed and mean and standard deviation
unless otherwise indicated. Statistical analysis was performed using SAS v9.1.3
software (SAS Institute, Cary,
NC).
Results
In total, there were 38 subjects in the study. The
mean age of all subjects was: 67.7 years (SD±8.9) with 23 (61%) female and 15
(39%) male.
Sixteen subjects (42%) were Caucasian, 14 (37%) were
African-American, 5 (13%) were Hispanic, and 3 (8%) were of another ethnicity.
Notably, only 54% reported any family history of glaucoma. Thirteen subjects
(34%) had previous glaucoma surgery. At baseline IOP was 15.4 (3.9) mmHg and
CCT was 547 (26).
IOP
measurements during the day and night time periods and in sitting and supine
positions are summarized in Table I. The
mean circadian IOP fluctuation was 8.88(3.2) mmHg from maximum to minimum
(p<0.0001, paired t-test). Night time IOPs were an average of 2.14(2.6) mmHg
higher than day time pressures (p<0.0001). Daytime supine pressures were
significantly higher than sitting by 2.8(1.1) mm Hg, (p<0.0001).
Daytime supine pressures were significantly lower than
night time supine pressures by 0.9(2.5) mm Hg, p=0.04. (Fig. 1)
No significant difference was observed between peak
daytime IOP, 22.5(4.5) mm Hg and peak night time IOP, 22.6(5.1) mm Hg.
IOP fluctuations were greater in patients with thinner
central corneas.
Table I. IOP
in 38 subjects with POAG
|
|
24-hr
|
Day
|
Night
|
|
|
Minimum
|
Maximum
|
|
All readings, mmHg
|
14.8 (3.4)
|
23.7 (5.3)
|
18.5 (3.8)
|
20.8 (4.3)
|
|
Sitting, mmHg
|
14.9 (3.5)
|
22.5 (4.5)
|
17.1 (3.7)
|
-
|
|
Supine, mmHg
|
17.0 (3.8)
|
23.5 (5.2)
|
19.9 (4.0)
|
20.8 (4.3)
|
Results
are expressed as mean (SD).
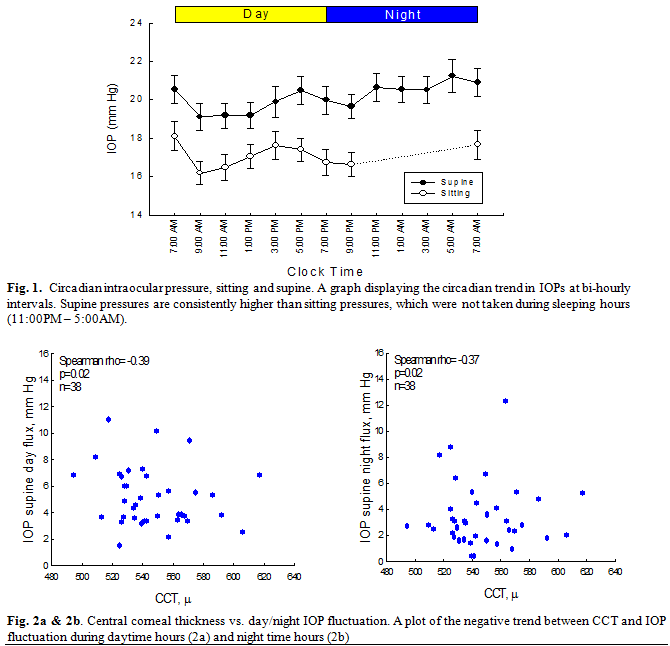
Significant inverse association were observed between CCT and daytime supine IOP flux (figure 2a, rho=-0.39, p=0.02) and between CCT and night time supine IOP flux (figure 2b, rho=-0.37, p=0.02).
Discussion
IOP control is the mainstay of clinical glaucoma management.(2)
In this well controlled group of patients, significant IOP fluctuations
were clearly evident during day and night. Even though daytime supine values
were greater than daytime sitting values, as expected, the maximum supine
values between day and night were not significantly different. Thus,
maintaining the patient’s daytime IOP peak within the target IOP range would
give a clinician confidence that the night time peak may not exceed the target
IOP.
Notably, the biphasic peak IOPs tended to occur at
5:00 PM and 5:00 AM, outside of typical clinic hours. Considering that daytime
and night time peaks are similar, managing the average fluctuation of a
patient’s daytime IOP would suffice in trying to achieve 24-hour IOP control.
The average diurnal fluctuation of 8.88 mmHg could
mean that a single in-office IOP measurement is not enough. An innocuous IOP
taken at 9.00 AM office visit could increase beyond the acceptable upper
threshold later in the day. Therefore, for optimal care, both the patient’s
daytime IOP peak and range of IOP fluctuations may need to be assessed.
CCT may play a larger role, directly or indirectly, in
IOP fluctuation than previously described.(8-10) Our data
shows that CCT may explain up to 15% of the variance in fluctuation between
patients with thinner and thicker CCTs. This may explain the importance of CCT
in progression of glaucoma. CCT is a simple and non-invasive method to assess
risk of progression.
This reinforces the conclusion recently published in a
report by the Academy
of Ophthalmology,(11)
that stated: “measuring CCT is an important component of a complete ocular
examination, particularly for patients being evaluated for the risk of
developing POAG. Therefore, CCT measurement should be included in the
examination of all patients with ocular hypertension. Although the evidence
supporting the necessity of measuring CCT as part of screening for POAG or as a
risk factor for glaucoma progression is not as strong, IOP is the only
modifiable risk factor in the treatment of glaucoma, and CCT has the potential
to significantly impact IOP measurement by applanation tonometry in all
patients.”
Also, a study by Liu et al.(12)
found that glaucomatous eyes have higher mean diurnal IOP compared with healthy
eyes, their diurnal-to-nocturnal change of habitual IOP is smaller, and the
posture-independent IOP pattern around normal awakening time is different in
eyes with early glaucomatous changes.
These represent a growing body of evidence that CCT
plays an important role in diurnal IOP and long-term effects on optic disc
damage. Patients with thin CCTs may require a much lower target IOP
than previously described.
Conclusion
This study has shown that diurnal IOP fluctuations are
common even in clinically controlled patients with glaucoma (8.88 mmHg) of whom
patients with POAG and thinner central corneas showed greater diurnal IOP
fluctuations. They are at a greater risk of further damage to the optic disc
than individuals with thicker CCTs. CCT may be very useful risk factor to
consider when creating a target IOP range for adequate control.
The postural influence on IOP is also relevant in
clinical practice. Supine pressures, such as those found during nocturnal
sleep, are significantly higher than the typical daytime sitting pressure taken
during clinic hours.
It is also important, as this study has demonstrated,
to assess the peak IOPs in any given patient before calculating the intended
target pressure. As daytime peaks mimic night time peak IOP, it may not be as
necessary to seek a 24-hour analysis of pressures as long as the daytime peak
has been measured.
References
1.Quigley HA, Borman AT. The
number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol 2006; 90: 262-267.
2.American Academy of Ophthalmology Quality of Care Committee Glaucoma
Panel. Primary open angle glaucoma, preferred
practice pattern. American
Academy of Ophthalmology,
San Francisco, 2005. Available at: www.aao.org/ppp.
3.Gordon MO, Beiser JA, Brandt JD, et al. The ocular hypertension treatment study: baseline
factors that predict the onset of primary open-angle glaucoma. Arch
Ophthalmol 2002; 120:714–720.
4. Jonas J B, Stroux A,
Velten I, et al. Central corneal thickness correlated with glaucoma
damage and rate of progression. IOVS 2005; 46:1269-1274.
5.Asrani
S, Zeimer R, Wilensky J, et al. Large diurnal fluctuations in intraocular pressure are independent risk
factors in patients with glaucoma. J Glaucoma 2000; 9: 134-142.
6.Johnson T, BA, Toris C, Fan S,
et al. Effects of central corneal thickness on the efficacy
of topical ocular hypotensive medication. J Glaucoma 2008; 17:
89-99
7.Brandt JD, Beiser JA, Gordon
MO, et al. Ocular hypertension
treatment study group: central corneal thickness and measured IOP response to
topical ocular hypotensive medication in the ocular hpertension treatment study.
Am J Ophthalmol 2004; 138(5):717-722.
8.Haknilton K, Optam B, Pye D,Aggarwal S, et al. Diurnal variation of central corneal thickness and
goldman applanation tonometry estimates of intraocular pressure. Glaucoma 2007; 16:29-35.
9.Mosaed S, Chamberlain W, Liu J, et al. Association of Central Corneal Thickness and 24-hour
Intraocular Pressure Fluctuation. J Glaucoma 2008; 17: 85-88.
10.Fogagnolo P, Rossetti L,
Mazzolani F, et al. Circadian
Variations in central corneal thickness and intraocular pressure in patients
with glaucoma. Br J Ophthalmol 2006; 90:24–28
11.Dueker DK, Singh K, Lin SC. Corneal thickness measurement in management of
primary open-angle glaucoma a report by the American Academy of Ophthalmology. Ophthalmology
2007; 114: 1770-1787
12.Liu
JH, Zhang X, Kripke DF, Weinreb RN. Twenty-four-hour
intraocular pressure pattern associated with early glaucomatous changes. Invest
Ophthalmol Vis Sci 2003; 44(4):1586-1590.