ABSTRACT
Objectives: To assess the
impact of age, gender, duration of diabetes and body mass index confounders on
diabetes control among a Jordanian cohort of T2DM at the Endocrine Clinic in King Hussein
Medical Center.
Methods: Patients were selected over 18 months from outpatient
clinic at King Hussein Medical
Center in Amman-Jordan.
Diabetes control assessed by mean of latest 3 HbA1c and fasting blood sugar.
Patients were divided in 2 groups according to age (<55 years Vs >55
years), gender, duration (<10 years Vs >10 years) and BMI (normal,
overweight, and obese according to WHO criteria). Statistical analysis is
performed using SPSS11.5.Good diabetes control is assessed according to American
Diabetes Association criteria
Results: A total of 405 patients were selected (223 males, 182
females). 115 patients (28.4%) were having a good control with HbA1c <7%.; 25.6%
of males and 31.9% of females were having good control (P value =0.161).
There
was no difference in diabetes control of those <55 years (n=183) Vs those
>55 years (n=222) (29%vs.28%; p=0.812). Females in both age groups were
having non statistically significant better control than males. Of those with
DM duration <10 years (n=242); 34.7% were having good control vs. only 19%
for those > 10 years duration (n=163) {P-value=0.001, RR=1.83, OR=2.26}.
Females were again having a better diabetic control in both duration groups,
p=0.024.
There
was no statically significant difference in diabetic control in all BMI
categories studied. Thirty percent of overweight patients were having good
control Vs <20% in normal and obese patients.
The
mean HBA1c in males was 8.1±1.7% Vs 7.9±1.5% in females. For the group <10
year, HBA1c was 7.75±1.5% Vs 8.32±1.54% in those >10 year. The mean HBA1C of
the group aged< 55 years was 8.1±1.8 Vs 7.9±1.5 in those >55 years of
age.
Conclusion: In this
Jordanian group with T2DM the diabetic control was modest at 28.4%. Females
were having a better diabetic control at all categories. Diabetes duration less
10 years was the only indicator of adequate control of diabetes.
Key words: BMI, Diabetes control, Diabetes duration, Gender, T2
diabetes.
JRMS
September 2012; 19(3): 33-38
Introduction
Diabetes is associated
with a reduced lifespan, largely as a consequence of cardiovascular disease.
Gender differences in diagnostic
procedures, risk factor control and treatment profile of cardiovascular disease
have been the subject of several investigations.(1-3) Less is
known, however, about corresponding gender differences in the treatment of
patients with diabetes.(4)
From the published literature we know that gender
differences in adherence to diet and diabetes treatment may be attributed, in
part, to gender differences in symptoms among young type 1 diabetics from urban
environment with poor metabolic control. Interventions targeting these symptoms
may be necessary to improve adherence and HbA1c control in male as well as
female patients.(5,6)
Male and female
diabetic patients differ in respect of biological, social, as well as
behavioral factors, frequently depending on age.(7)
In the UKPDS it was shown that the HbA1c tend to
increase with the duration of diabetes losing it control,(8) several studies also showed differences in
diabetes control among different ethnic groups ,genders and obese patients tend
to have poorer diabetes control.(8,9)
It is known that improved glycemic control improves
microvascular outcomes, less is known about the factors that influence control.
Harris et al.(10) examined racial and
ethnic differences in glycemic control in patients with Type 2 diabetes using
the Third National Health and Nutrition Examination Survey (NHANES III) and
found that black women, Mexican-American men, those treated with insulin or
oral antiglycemic medications, and patients over 60 years of age had poorer glycemic
control. Shorr et al.(11) studied the
relationship between age and glycemic control and found no significant
differences between age groups. Nichols et al.(12)
found that age, body mass index (BMI) and emotional distress were
significantly related to glycemic control. Blaum et al.(13)
found that disease duration; C peptide levels, poor self-care, and
failure to receive diet recommendations were related to control in a mostly
white, primary care population in USA.
Diabetes mellitus is a prevalent chronic disease in Jordan, the recent
estimates are of 17.1% of the population
are diabetics and 7.8% are
having impaired fasting glucose.(14)
Therefore diabetes constitutes a medical and economic burden. Studies of the factors that have an impact on
diabetic control are in Jordan;
only one study
showed
that low BMI, shorter duration of diabetes
and higher baseline HbA1c were related
to diabetes control after 12 months of follow up period.(15)
The aim of this
study is to assess the impact
of age, gender, duration of diabetes
and body mass index confounders
on diabetes control among a
Jordanian cohort of T2DM
at the Endocrine
Clinic
in King Hussein Medical Center.
Methods
This study was conducted by recruiting patients who attended
the diabetes clinic who were randomly selected over 18 months from outpatient Endocrine
clinic of endocrine division at King
Hussein Medical
Center in Amman-Jordan from
January 2009 till June 2010.
The inclusion criteria included all patients with type
2 diabetes who attended on each Tuesday of each week who have at least 2-3
HbA1c, lipid profile and Fasting Blood Sugar (FBS) performed over previous
year. Patients with type 1 diabetes were not included.
This study was approved by the Royal Medical services
Ethical Committee. Verbal consent was obtained from all participants.
The patients, after history taking, were assessed for
demographic features, anthropometric measures and associated conditions;
physical examination was performed by an endocrinologist.
Blood was drawn in a fasting stat for FBS, lipid
profile, kidney function and liver function tests, and HbA1c, tests were
performed using automated multichannel analyzer (Hitachi 917, Modular type) Diabetes control was finally expressed as the mean of
latest three readings of HbA1c and FBS results over the follow-up period of
14±2 months.
The American Diabetes Association (ADA) criteria for
adequate diabetes control for fasting blood sugar (FBS <100mg) and HbA1c
(<7%) was adopted.(16)
Patients were divided into 2 groups according to age
(<55 years Vs >55 years), gender, duration (<10 years Vs >10 years)
and three groups of Body Mass Index {BMI}: normal, overweight, and obese
according to WHO criteria.(17)
Statistical analysis Intra and inter group comparisons
were performed in all groups studies using z static for difference between two
percentages, t test for comparing means and univariate and multivariate
analyses for prediction and calculating Odd Ratio (OR) and Relative Risk (RR) performed
using SPSS 11.2 and EPI Info 6 2005, values were expressed as means and
Standard Deviation (SD); a p value < 0.05 was considered as significant.
Results
A total of 405 patients were selected; there were 223
males and 182 females, the mean age is 54.6±10.45 years (M vs. F, 53.9±11.4 vs.
55.5±9.2; p= 0.065). Diabetes duration
was 10.3 ±7.4 (M vs. F: 10.6 ±7.8 vs. 9.98 ±6.9; p= 0.2). Body Mass Index (BMI
kg/m2) was 30.4 ±4.9 (M vs. F: 29 ±4.3 vs. 32.1
±5.1; p<0.00003).
Table
I: Demographic features mean values
of HbA1c and fasting blood sugar among the study group
|
Mean
±SD
|
n=405
|
|
Age
(year)
|
54.6 ± 1.4
|
|
BMI
kg/m2
|
30.4 ± 4.9
|
|
Duration
(years)
|
10.3 ± 7.4
|
|
Smoker %
|
24.4%
|
|
HbA1c
(%)
|
7.83 ± 1.99
|
|
FBS
(mg/dl)
|
193.5 ± 84.8
|
Table
II: Percentage of diabetic control
(HbA1c ≤ 7%) according to gender, age, duration and BMI criteria
|
|
Male
|
Females
|
All
|
P value
(M vs. F)
|
|
HbA1c
≤
7%
|
25.6%
|
31.9%
|
28.4%
|
0.161
|
|
Age
<55
years
>
55 years
P
value
|
25.2%
25.8%
0.9
|
33.8%
30.4%
0.6
|
29%
27.9%
0.82
|
0.82
|
|
Duration
<10
years
>10
years
P
value
|
31.3%
17.9%
0.024
|
38.6%
20.6%
0.012
|
34.7%
19.1%
0.001*
|
0.23
0.66
|
|
BMI
Normal
Overweight
Obese
P
value
|
14.3%
17%
11.8%
0.07
|
4.8%
12.8%
17.9%
0.07
|
19%
29.8%
29.7I%
0.069
|
0.52
0.11
0.47
|
Table
III: mean HbA1c (±SD) according to
gender, age, duration and BMI criteria
|
|
Male n=223
|
Females n=182
|
All
|
P value
|
|
HbA1c
|
8.1 ±1.73
|
7.87±1.53
|
7.9±1.99
|
0.177
|
|
Age
<55
years
>
55 years
|
8.3±1.9
7.89±1.55
|
7.8±1.6
7.9±1.47
|
8.07±1.79
7.9±1.51
|
0.00
0.001
|
|
P
value
|
0.11
|
0.65
|
0.32
|
|
|
Duration
<10
years
>10
years
|
7.83±1.79
8.4±1.6
|
7.65±1.53
8.2±1.46
|
7.75±1.67
8.37.75±1.5
|
<0.001
0.029
|
|
P
value
|
0.02
|
0.012
|
0.001
|
|
|
BMI
Normal
Overweight
Obese
|
8±1.7
8.1±1.77
8.04±1.75
|
7.9±1.39
7.6±1.3
7.96±1.65
|
7.98±1.62
7.9±1.64
7.99±1.69
|
0.9
0.07
0.7
|
|
P
value
|
0.75
|
0.38
|
0.77
|
|
Demographic characteristics and mean levels of HbA1c
and fasting blood sugar (FBS) are shown in Table I.
One hundred and fifteen patients (28.4%) were having a
good diabetes control with HbA1c <7%;
25.6%
of males and 31.9% of females were having good control (P value =0.161).
In a univariate analysis there was no statistically
significant difference in diabetes control of those <55 years (n=183) Vs
those >55 years (n=222) (29%vs.28%; p=0.812). When gender groups were
considered; Females in both age groups have no statistically significant better
control than males (Table II).
Of those with DM duration <10 year (n=242); 34.7%
were having good control vs. only 19% for those > 10 years duration (n=163)
{P-value=0.001, RR=1.83, OR=2.26}. Females again were having a better diabetic
control in both duration groups, p=0.024 as demonstrated in Table II.
There was no statistically significant difference in diabetic
control in all BMI categories studied. Thirty percent of overweight patients
were having good control Vs <20% in normal and obese patients. (Table III)
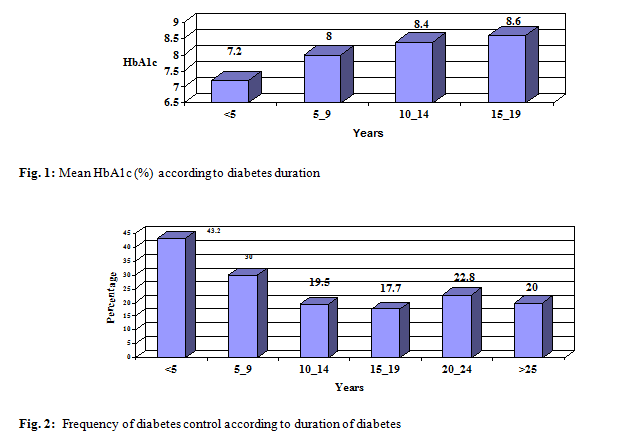
The mean HBA1c in males was 8.1±1.7% Vs 7.9±1.5% in
females. For the group <10 years, HBA1c was 7.75±1.5% Vs 8.32±1.54% in those
>10 year. The mean HbA1C of the group aged< 55 years was 8.1±1.8 Vs
7.9±1.5 in those >55 years of age (see Table III).
The course of mean HBA1c is illustrated in Fig. 1
where HBA1c increased with increasing duration of DM, while diabetic control
dropped with increasing age (Fig. 2).
Discussion
Diabetes control is
of paramount importance due to strong consensus that excellent control improves
micro-vascular complication in T2DM.(18)
Identifying
demographic, psychological and treatment factors that have an impact on
diabetes control may improve outcome by allowing better selection of patients
to compensators interventions.(12)
Diabetes control
expressed as HbA1c ≤ 7% was achieved in 28.4% of the cohort studied; females showed
non significantly better control than males (31.9 % vs. 25.6% p: 0.162 ), these findings
come in accordance to other loco-
regional studies form Jordan;(15) Saudi Arabia 27%19 and Kuwait.(20) However these figures are lower than
that reported in USA and Europe.(8,21,22)
Diabetes control
showed a steady worsening expressed by increasing HbA1c over follow up period since
diagnosis and with increasing age (Fig. 1 and 2) that is in keeping with many
studies including UKPDS33 and Benoit et al.(8,18) The decline in β cell function with type 2 diabetes progressions
over time is the explanation of this deterioration in diabetes control that has
an impact on patients’ physical and psychological wellbeing, quality of
adherence to treatment and on health economics.
The demographic
features studied in this study, in a univariate analysis, did not show any
significant impact on diabetes control; there was no difference in total
diabetes control for those patients above 55 years vs. those below 55 years. This
also did not show differences in both gender studied (Table II, III). These results
were at odds to the study of Benoit et al(17) that showed that younger
age was significant in the final models with main effects.
Duration of
diabetes exerted an impact on diabetes
control; those with shorter duration ≤
10 years were having better diabetes
control than those with longer duration (34.7%
vs. 19.1% p= 0.001; RR=1.83 (1.27-2.62),
OR=2.26 (1.38-3.73)
). No difference between the two genders studied in this
category (Table II). The mean HbA1c was significantly lower in those with
shorter duration vs. longer duration. This comes in accordance with UKPDS and
other studies(8,14,22,23) and contradicts the
results of Nicholas et al.(12)
Body mass index was
not found to have any impact on diabetes control in this study; all categories
of BMI showed no difference in diabetes control rates nor in mean HbA1c levels (Table
II, III), these results contradicts the results achieved by Nicholas et al(12)
and Adham M et al(15) who showed a good relationship
between BMI and DM control.
This study showed
that diabetes control worsen with increasing duration of diabetes being more
than 43% achieving DM control of HbA1c ≤
7 for those < 5 years duration and this drop to ≈20 % for those with duration
> 20 years.
This study results
is consistent with other international studies that showed that longer duration
of diabetes worsens DM control and proved that progressing age impacted the
outcome of adequate HbA1c control.(24)
The rather small
sample size and calculating the mean of the latest three HbA1c levels are
probably limiting factors on final outcome
Summary and Conclusion
The current study
showed a modest diabetic control of 28.4% achieving HbA1c <7%. The diabetes
duration impacted the outcome when same genders were compared but not when
comparing males vs. females.
Age exerted an
impact on the mean HbA1c levels being better for females whether below or above
55 years old, while duration impact was evident for mean HbA1c levels being
better for males whether below or above 10 years duration . The mean HbA1c
showed a steep increase in its level with increasing duration of diabetes. The
diabetes control showed a drop in prevalence with increasing diabetes duration
A structured
program of intensified diabetes education and follow-up in needed to improve
diabetes control in Jordan.
Larger cross
sectional studies on factors implicated in diabetes control are warranted to
have better predictors of diabetes control and to address theses confounders.
Acknowledgement
The authors wish to
thank Mrs Ala’
Rifai; Diabetic Dietician, for her help in performing the statistical analysis.
References
1.Hippisley-Cox J, Pringle M,
Crown N, et al. Sex inequalities in ischemic heart disease in general
practice: cross-sectional study. BMJ 2001; 322:832-834.
2.Canto JG, Rogers
WJ, Goldberg RJ, et al.
Association of age and sex with myocardial infarction symptom presentation and
in-hospital mortality. JAMA 2012; 307(8):813-822.
3.Nilsson P, Brandstrom H,
Lingfors H, et al. Gender differences in secondary prevention: reasons
to worry or not? Scand J Prim Health Care 2003; 21:37-42.
4.Siann T, Duncan EM, Sullivan F, et al.
Area-wide diabetes care: the Lanarkshire
experience with primary health care teams 1994-1997. Diabetic Med 1998;
15(Suppl 3):S54-7.
5.Naar-King S, Idalski A, Ellis D, Frey M, et al. Gender differences in
adherence and metabolic control in urban youth with poorly controlled type 1
diabetes: the mediating role of mental health symptoms. J Pediatr Psychol. 2006; 31(8):793-802.
6.Biesenbach G, Bodlaj G,
Pieringer H. Gender-associated
Differences in Weight Gain, Insulin Requirement and Metabolic control in newly
Insulin-treated Type 2 Diabetic patients with secondary sulfonylurea Failure-a
one-year Observation. Clinical Medicine: Endocrinology and Diabetes 2009;
2:75-80
7.Rurik I. Nutritional differences between elderly men and
women. Primary care evaluation in Hungary. Ann Nutr Metab
2006; 45-50.
8.Intensive blood-glucose control
with sulphonylureas or insulin compared with conventional treatment and risk of
complications in patients with type 2 diabetes (UKPDS 33). UK Prospective
Diabetes Study (UKPDS) Group. Lancet 1998; 352(9131):837-53.
9.Egede LE, Gebregziabher M,
Hunt KJ, et al. And racial/ethnic variation in glycemic control in a
national sample of veterans with diabetes. Diabetes Care 2011; 34: 938-943.
10.Harris
MI, Eastman RC, Cowie CC, et al. Racial and ethnic differences in
glycemic control of adults with type 2 diabetes. Diabetes Care 1999; 22:403-408.
11.Shorr RI,
Franse LV,
Resnick HE,
et al. Glycemic control of older adults
with type 2 diabetes: Findings from the
Third National Health and Nutrition
Examination Survey, 1988–1994. J Am Geriatr Soc 2000; 48:264–267.
12.Nichols
GA, Hillier TA, Javor K, et al. Predictors of glycemic control in
insulin-using adults with type 2 diabetes. Diabetes Care 2000; 23:273–277.
13.Blaum CS,
Velez L, Hiss RG, et al. Characteristics related to poor glycemic control in NIDDM
patients in community practice. Diabetes Care 1997; 20:7–11.
14.Ajlouni K, Khader YS, Batieha
A, et al. An increase in prevalence
of diabetes mellitus in Jordan
over 10 years. J Diabetes Complications
2008; 22(5):317-324.
15.Adham M, Froelicher ES,
Batieha A, et al. Glycaemic control and its associated factors in type 2
diabetic patients in Amman,
Jordan. Eastern Mediterranean Health Journal 2010;16(7):732-739
16.Diagnosis
and Classification of Diabetes Mellitus. American Diabetes Association. Diabetes Care 2006; 29:S43-S48
17.WHO
expert consultation. Appropriate body-mass index for Asian populations and
its implications for policy and intervention strategies. The Lancet
2004; 157-163.
18.Benoit SR, Fleming R, Ming JI. Predictors of glycemic control among patients with
Type 2 diabetes: A longitudinal study BMC
Public Health 2005; 5: 36.
19.Akbar DH. Low rates of diabetic patients reaching good control
targets. East Mediterr Health J
2001; 7(4-5):671-678.
20.Al-
Sultan F, Al-Zanki N. Clinical epidemiology of type 2 diabetes mellitus in Kuwait.
Kuwait
Medical Journal 2005;37: 98-104
21.Guzder RN, Gatling W, Mullee
MA, et al. Impact of metabolic syndrome criteria on
cardiovascular disease risk in people with newly diagnosed type 2 diabetes. Diabetologia 2006; 49(1): 49-55.
22.Saaddine JB, Cadwell B, Gregg
EW, et al. Improvements in diabetes processes of care and intermediate outcomes: United States, 1988-2002. Ann
Intern Med 2006; 144(7): 465-474.
23.Goudswaard AN, Stolk RP,
Zuithoff P, et al. Patient characteristics do not predict poor glycaemic
control in type 2 diabetes patients treated in primary care. Eur J Epidemiol
2004; 19(6):541-545.
24.El-Kebbi IM, Cook CB, Ziemer
DC, et al. Association of
younger age with poor glycemic control and obesity in urban African Americans
with type 2 diabetes. Arch Intern Med 2003;163(1): 69-75