ABSTRACT
Objective: To review the experience and outcome of liver
transplantation recipients at King
Hussein Medical
Center.
Methods:
We retrospectively analyzed the results
of 67 liver transplantations; 65 living-related donor liver transplantations
for 64 recipients and two cadaveric donor liver transplantation at King Hussein
Medical Center
between June 2004 and December 2011. The grafts were: 60 right liver lobes, four
left liver lobes, one hepatic segments II and III and two whole livers
(cadaveric). All living donors were closely related to the recipients except for
the cadavers. Data were obtained by a
specially designed medical record abstract form. Of the 67 liver
transplantations, the first 42, were performed under the supervision of the
Turkish liver transplantation team. Six recipients had concomitant
hepatocellular carcinoma and liver cirrhosis. Retransplantation was performed
for one recipient. Simple descriptive statistical methods (frequency, mean and
percentage) were used to describe the study variables.
Results: Total
mortality rate was 11 (17%). The causes of death were sepsis in four patients,
hepatic arterial thromboses in three patients, small-for-size in one patient, and
porto-pulmonary hypertension in one patient. Morbidity rate was 49 (73.1 %). The
main causes of morbidity were biliary leaks in 13 patients, biliary stricture
in nine patients, recurrence of primary disease in nine patients acute
rejection in five patients, wound infection in four patients, and bile duct
stones in one patient. The follow-up
period ranged between one month to 90 months (average 45.5 months). One and
three year survival rates were 80% and 70.2% respectively. However, most
complications have been treated with interventional techniques. All living donors are alive in a good health
and returned to their normal life.
Conclusions: In view
of critical shortage of cadaveric donor liver transplantation, living-donor
liver transplantation is an opportune option for patients with decompensated
liver disease in Jordan.
Our patients’ outcome is improving with time and this could be attributed to
gaining more experience and by-passing the learning curve by the liver
transplantation team in our center.
Key words: Complications, Liver transplantation, Outcome
JRMS
December 2012; 19(4): 5-12
Introduction
Liver transplantation is the therapeutic option of
choice for acute and chronic end-stage liver disease. Transplantation is a
relatively new medical specialty, dating back to only 1954 when Dr Joseph
Murray did the first living donor kidney transplantation, then followed by
cadaveric donation after eight years.(1)
Table I. Patients characteristics of the study group
|
Recipient characteristics
|
Number
|
%
|
|
Age
|
|
|
|
Adult
|
58
(17-63year (average 40))
|
86.6
|
|
Pediatric
|
9
(3-14 year
(average 9) )
|
13.4
|
|
Sex
|
|
|
|
Male
|
49
|
73
|
|
Female
|
18
|
27
|
|
Relationship to donors
|
|
|
|
Father
|
6
|
8.9
|
|
Mother
|
5
|
7.4
|
|
Son
|
22
|
32.8
|
|
Brother
|
9
|
13.4
|
|
Sister
|
9
|
13.4
|
|
Wife
|
4
|
5.9
|
|
Daughter
|
1
|
1.4
|
|
Cousin
|
1
|
1.4
|
|
Nephew
|
5
|
7.4
|
|
Uncle
|
1
|
1.4
|
|
Aunt
|
1
|
1.4
|
|
Emotional
|
1
|
1.4
|
|
Un-related (cadaver)
|
2
|
2.9
|
Table II. Indications
for liver transplantation among the study group
|
Indication for liver transplantation
|
Number
|
%
|
|
Cryptogenic hepatitis
|
14
|
20.8
|
|
AIH
|
8
|
11.9
|
|
Viral Hepatitis
|
15
|
22.3
|
|
HBV
|
8
|
11.9
|
|
HCV
|
7
|
10.4
|
|
Cholestatic liver disease
|
6
|
8.9
|
|
Malignancy:
|
8
|
11.9
|
|
HCC+HBV
|
5
|
7.4
|
|
HCC+HCV
|
1
|
1.4
|
|
HCC
|
1
|
1.4
|
|
Hepatoblastoma
|
1
|
1.4
|
|
Others
|
8
|
11.9
|
AIH: Autoimmune Hepatitis HBV: Hepatitis B Virus HCV:
Hepatitis C Virus
HCC: Hepatocellular Carcinoma
Thomas Starzl performed the first three cadaveric human liver transplantations
in 1963, all died before reaching 1-year survival, and it was not until 1967
when he did the first successful transplantation.(2-4) The
first attempt of Living Donor Liver
Transplantation (LDLT) was in children and was performed by Raia et al.
in 1988, while the first successful LDLT
in an adult recipient was done for the first time by the
Japanese in 1994 and then Western countries has followed this
path.(5,6) While the shortage of donor organs is a global
problem, the situation appears more critical in Asia where cadaveric organ
donation remains below five per million populations (pmp).(7)
Although LDLT has several advantages over cadaveric
liver donor transplantation (CDLT), the main limitation for
successful adult-to adult LDLT is Graft-Recipient weight-Ratio (G-RW-R) mismatch,
in which the graft cannot meet the metabolic demands of the recipients.(8,9)
It is obvious that adults need larger graft to meet their metabolic demand. So, left or right hepatectomies were required,
which put the donor at the risk of high morbidity from a significantly major
operation.(6,10,11)
The aim of this study is to review our experience and
outcome of liver transplantation recipients, at King Hussein
Medical Center.
Methods
Between June 2004 and December 2011, a total of 67 liver
transplantations were performed for 66 recipients. Sixty five of them were
LDLTs including one re-transplantation while the other two were CDLT. Male to female ratio was 49\18 (73%-27%). Fifty
eight percent of the patients were adults with the average age of 40 years (range
17-63 years), while the remaining recipients were children (less than 15 years
of age) with the average age of nine (range 3-14 years). Recipient characteristics are showed in Table I.
Most of the indications for liver transplantation were
chronic liver cirrhosis due to cryptogenic hepatitis (14), viral hepatitis (15),
cholestatic liver disease (6), autoimmune hepatitis (AIH) (8), and other factors
(Table II).
The pre-transplant condition of the recipients was
evaluated by the modified model for end- stage liver disease (MELD) score(12) which has been documented to be reliable in predicting the prognosis of the patients. The contraindications for transplantation are listed in Table III.
Table III. Contraindication
for liver transplantation
|
Contraindication for
transplantation
|
|
Hepatic malignancy with macrovascular or diffuse tumor invasion
Active and uncontrolled infection outside of the hepatobiliary system
Severe cardiopulmonary or other comorbid conditions
Technical and/or anatomical barriers
Age above 65years
Cholangiocarcinoma
Portal vein thrombosis
Chronic or refractory infection
Active psychiatric illness
Poor social support
|
We accepted only donors with
graft-to-recipient weight ratios ≥ 0.8% and fatty liver ≤ 20%. The remnant of
donor’s liver (residual liver volume) always exceeded 35% of the total liver volume
as calculated by computed tomography volumetry. The age of the donors ranged
from 19 to 55 years (average 37 years).
Simple descriptive statistical methods (frequency, mean and percentage)
were used to describe the study variables.
Donor hepatectomy:
Donor hepatectomy is a standard procedure in all
centers.
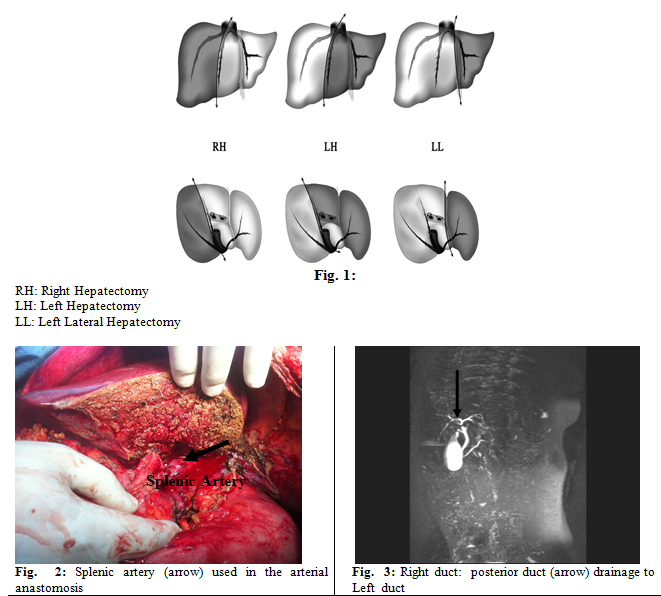
Three hepatectomies were defined
according to the segmental anatomy of Couinaud. Left Lateral Hepatectomy (LL) for resection of segments II and III, left
hepatectomy (LH) for segments resection of II, III and IV, and right hepatectomy (RH) for
segments V, VI, VII and VIII resection(13)
(see Fig.1).
Recipient operation:
Total hepatectomy performed with the original hepatic veins
(with extension to IVC to make triangular shape opening) or vena cava were used
for the hepatic vein anastomosis. Biliary, portal and hepatic anastomosis were
performed with loop magnification, and the arterial anastomosis performed by a
micro-vascular surgeon with microscope. The hepatic veins anastomosed to IVC with continuous
suture by Prolene 4\0, also the portal veins (right and left) were anastomosed to the
main portal vein by Prolene 5\0. Inferior hepatic veins (larger than 7mm) were
anastomosed end to side to the inferior vena cava. After completion of the
portal vein anastomosis, removal of the air and stagnant preservative solution
from the graft done by washing out with the portal blood. The hepatic artery
was anastomosed to the recipient right hepatic artery in the RH LDLTs except
for two recipients; we used the splenic artery because of extensive intimal
dissection in the hepatic artery which extended to the celiac trunck (Fig. 2),
and to the left hepatic artery in the LT, LL LDLTS. In the CDLTs the common
hepatic artery of the graft anastomosed to common hepatic artery of the
recipient.
Biliary reconstruction was done with a duct-to-duct
anastomosis in 60 transplants and with Roux-en-Y hepaticojejunostomy in seven
transplants. Twenty eight (41%) of the 67 liver grafts had two bile ducts (Fig.
3). In five of these 28 grafts with two bile ducts, two separate anastomoses
were performed. In the remaining 23 grafts, ductoplasty performed by
approximating the neighboring bile duct and, sutured together to create a
single bile duct opening. One of the 67 liver grafts had three bile ducts. In
this situation, two neighboring ducts were sutured together and anastomosed end-to-side
to the jejunum, and the third duct anastomosed separately end-to-side to the
jejunum (Roux-en-Y hepaticojejunostomy). In this recipient, we placed internal
catheters. In three recipients, a straight feeding tube was inserted from the
common bile duct to the anastomotic site to enable external bile drainage.
Cell-saver was used during the recipient operation for
13 patients. Standard antibiotic therapy with gram-negative and gram-positive
coverage was administered for five postoperative days. Lamivudine, 100 mg
daily, was given orally for patients with hepatitis B viral infection before
transplantation and continued long life afterward. Hepatitis B immunoglobulin was used in all
patient with hepatitis B at the anhepatic phase at a starting dose of 2000iu and then 500iu per day for one week ,then
discontinued when HBVAb titer (>100).
Immunosuppression induction therapy was provided with
Methyl prednisolone 100mg intraoperatively and on postoperative day one then
tapering daily till the day nine to be 20mg prednisolone orally. The
postoperative immunosuppression was based on tacrolimus and mycophenolate
mofetil and steroids. All recipients also received oral fluconazole 200mg daily
after the operation for three months.
Results
Of the liver transplant recipients in our study, two
underwent CDLT and sixty five underwent LDLT (60 underwent right lobe transplantation;
four left lobe; and one transplantation of the left lateral segment). In one
recipient, retransplantation was performed (8 days after the first
transplantation) because of hepatic artery thrombosis. The mean ratio of graft
volume to the body mass of
the recipients was 1% (range,0.8 –1.4) in the adult group and 3% (range, 2.6- 3.4) in the
pediatric group. The average cold ischemia time of the liver graft was 75
minutes (range, 60-90 minutes). The average operative time was 12 hours (range,
8–16 hours). All except two recipients received blood transfusion (9 U; range
0-18 U). The average postoperative intensive care unit stay was 17.5 days
(range, 10-25 days), and the average postoperative hospital stay was 37 days
(range, 13-61 days).
Hepatic arterial thrombosis (HAT) has complicated
three of our recipients (5.9%) in the early post operative days. This
complication was diagnosed during routine liver enzymes test then proved by
Doppler ultrasonographic examinations and CT angiogram. One of those three required
retransplantation to treat his HAT, but died 24 hours after the operation.
Thrombectomy was performed in one recipient, by interventional radiologist, but
failed and the patient died. The third one died before any intervention because
he developed multi-organ failure.
Two recipients developed bleeding one day after
transplantation, which necessitated reopening. One was found to bleed from a
branch of the hepatic artery and was successfully treated by ligation of the
bleeding vessel, and the other one from the site of jejuno-jejunostomy and was treated
by revision of the anastomosis.
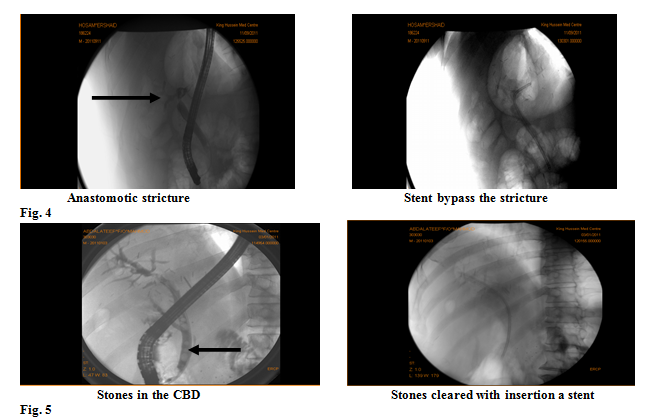
Thirteen (19.4%) and nine (13.4%), of the 67 recipients in our study
experienced a bile leak and bile duct stenosis respectively, and one of the
stenosis group had CBD stones. The bile
leak occurred at the anastomotic site in eleven recipients, and from the graft
cut surface in two recipients. Anastomotic bile leaks were treated by
percutaneous drainage followed by endoscopic placement of a 7-10Fr plastic
stent except two, where ductal anastomosis were completely disrupted and
converted to roux-en-Y hepatico- jejenostomy. The non-anastomotic bile leaks
were treated with percutaneous drainage. Bile duct stenoses occurred at the
anastomotic site in seven recipients and at the nonanastomotic site in the
remaining two recipients. All bile duct stenoses were treated with internal
stent in our hepatology unit by ERCP with excellent results (Fig. 4), except
for one that necessitated PTC by interventional radiologist and ERCP with
extraction of stones from the CBD and insertion a stent (Fig. 5).
One hepatic vein stenosis, developed during the late postoperative period which were treated by percutaneous transluminal angioplasty.
Table
IV: Complications
of the recipients and the management
|
Complication
|
Number (49)
|
% (73.1%)
|
Management
|
|
Wound infection
|
4
|
5.9
|
Antibiotics +debridement
|
|
Biliary leak
|
13
|
19.4
|
Interventional
radiology or H-J
|
|
Biliary stenoses
|
9
|
13.4
|
Interventional
radiology
|
|
Acute rejection
|
5
|
7.4
|
Steroid
recycling or pulses
|
|
Recurrence
of primary Disease
|
9
|
13.4
|
Medical treatment
|
|
Incisional hernia
|
2
|
2.9
|
Observation or surgery
|
|
Small for size
|
1
|
1.4
|
Somatostatin
|
|
CBD stone
|
1
|
1.4
|
Interventional radiology
|
|
Lymphoma
|
1
|
1.4
|
Chemotherapy
|
|
Drop hand
|
1
|
1.4
|
Physiotherapy
|
|
Hepatic vein stenoses
|
1
|
1.4
|
Interventional radiology
|
|
Hepatitis B
|
1
|
1.4
|
Antiviral therapy
|
|
Bleeding
|
1
|
1.4
|
Re-operation
|
H-J: hepaticojejunostomy
Five recipients (7.4%) experienced an episode of acute
rejection during the follow-up period. These cases were treated with
corticosteroid recycling or pulses therapy.
Two recipients had incisional hernia for which repair
was performed; and one of these patients, had hernia repair surgery outside Jordan, which was
complicated by bowel perforation and led to his death. One patient with primary sclerosing
cholangitis (PSC) had HBV infection post transplant, and he is on treatment.
One patient developed lymphoma after one year and he is on chemotherapy.
One recipient developed functional small for size
condition (SFS) due to persistent portal hypertension post operatively, and was
managed well by somatostatin infusion (250mic g\hour) for five days.
During our study twenty three (34.4%) patients died
from the subsequent causes: 11 sepsis with multiorgan failure, three
porto-pulmonary hypertension (respiratory distress), three HAT, two recurrence
HCC, one after repair of incisional hernia due to bowel perforation, one
arrested during removal of central line,
one from persistent hyperbilirubinia. At this time, the remaining 44 recipients
(65.6%) are alive with good graft function. Complications experienced in forty
two recipients (62.6%) are shown in Table IV.
Discussion
Liver transplantation has become a life saving procedure for fulminant
and chronic end-stage liver disease and for selected patients with hepatic
malignancies(14-16) LDLT has been accepted as an alternative
choice specially in Eastern societies, who otherwise would have; due to the
presence of strong cultural, traditional and religious beliefs, limited or
delayed access to a cadaveric organs. As a matter of fact, it is a remarkably
effective and real hope of new life for thousands of recipients worldwide.(17)
In Jordan we face the same problem
according to the availability of cadaveric donations (2 cases within 7 years),
so LDLT is considered the cornerstone of the liver transplantation and is now
becoming the only life saving with widely accepted treatment modality for
chronic liver failure and some selected hepatocellular carcinoma cases.
Livers from living donors offer many potential
advantages over livers from cadaveric donors. The most important advantages of
living donation are that it optimizing the timing of transplantation and
freeing patients from the waiting list, minimizing the preservation time (lower
ischemic time), and the operation is
done on a hemodynamically stable donors. So, the quality of the living donated
liver is much better.(18-20)
The survival rates after CDLT are expected to be more
than 85% and 75% at 1-year and 5-years post-transplantation, respectively, on
the other hand, LDLT had much lower survival rate at the time of start of the
procedure.(4) But later, Chuan Li et al. reported that
LDLT and CDLT have equivalent long-term survival rates, similar severe
postoperative complications, similar HBV recurrence rates and required similar
numbers of RBC transfusion units.(21) On the other hand, the incidence of biliary complication in the
patients undergoing LDLT was higher than those who received CDLT. The total
biliary complication rate was observed to be significantly different during
long-term follow up (25% after a median follow-up of 27 months), which was
significantly higher than that after CDLT.(16)
Living donor
has significant risks, including the risk of donor death (0.2%-2.0%) and
substantial morbidity (30%), that must be taken into account before patients,
physicians, and transplant programs go on board in LDLT.(22-24)
However, with improvement in surgical technique, selection of the donor, and postoperative
care, it was possible to reduce perioperative morbidity significantly.(6)
So, no effort should be spared in
avoiding complications by appropriate patient selection, controlling blood
loss, meticulous surgical technique, and post-operative care.(25)
The initial reports of high recipient successes and low donor morbidity rate
led to rapid expansion of adult-to-adult LDLT.(10)
All our donors
are alive and returned to their normal life soon after surgery.
Due to shortage of deceased donor organ in Jordan,
LDLT has acquired a great reputation. From June 2004 to December 2011, 67 cases
of LTs were performed in our center.
At the beginning of our program (first 30 cases), the
mortality rate among the recipients was eight patient (11.9%) compared to only three
recipients death in the following 37 cases (4.4%). This could be attributed to
the learning curve and our experience in selecting the patients. Sepsis (bacterial, viral, or fungal), which
is the most frequent cause of post transplant mortality, afflicts about 50% of
recipients who undergo LDLT. In the last
37 cases, three patients (4.4%) died.
The biliary complication rate in the early part of our
program was high where leakage and stenosis occurred in 47% in the first 30
patients. After identification of the possible causes of leakage, the leakage
rate was markedly reduced, but late stenosis still occurred. The overall
biliary complication rate in the subsequent 37 patients was 27%. There is a
decrease in the complication rate over the years as our experience builds up. However, it must be noted that biliary
stenosis may occur several years later. Longer follow-up is required to
ascertain a valid comparison. Nonetheless, an improvement of the early result
has indeed been observed but it still higher than other centers (14.8%).(20)
While chronic
complications related to immunosuppression and to the transplant itself are
quite common and accumulate in the long term, the quality of life of liver
transplant recipients is good and remains comparable with that of the general
population.(26, 27) Our results of 1-year and 3-year survival
(82% and 70% respectively) are relatively comparable to other centers which is 84%
and 79% respectively.(20) Most of our recipients returned to
their normal life and work. With build-up of experience in surgery and clinical
management, timely feedback and proper modification, the outcomes will be
better in the future.(5)
Conclusions
With critical shortage of cadaveric donor in
our country, LDLT continues to be a life-saving opportunity that may change
life expectancy for the majority of patients. Although chronic complications
are quite common and accumulate in the long term, the quality of life of liver
transplant recipients, even over decades, nonetheless remains comparable with
that of the general population.
Our results are comparable with the international
figures, although it is still lagging behind some other centers, with
accumulation of our experience we started to overcome the learning curve, and
to have better outcomes.
References
1.Mandell M, Tsou M. The development of perioperative practices for liver transplantation:
advances and current trends. J Chin Med Assoc 2008;71(9):435–441
2.Susumu
E, Mitsuhisa T, Masaaki H, et al. Evolution of
living donor liver transplantation over 10 years: experience of a single
center. Surgery Today 2008; 38(9): 795-800.
3.Chan S, Fan S. Historical perspective of living donor liver
transplantation. World J Gastroenterol 2008; 14(1): 15-21
4.Moon D, Lee S. Liver Transplantation. Gut and Liver 2009; 3(3):
145-165
5.Xi F, Ding Y, Gang W, et al. Outcomes of adult-to-adult living donor liver
transplantation single center experience. Chinese Medical Journal 2009;122(7):781-786
6.Broering
D, Wilms C, Bok P, et al. Evolution of donor morbidity in living relate
liver transplantation. Ann Surg 2004; 240: 1013-1026
7.Lee
V, Yip C, Ganpathi I, et al. Expanding the donor pool for liver
transplantation in the setting of an “opt-out” scheme – 3 years after New
Legislation. Ann Acad Med Singapore 2009; 38:315-21
8.Bog D,
Lee S. Adult-to-adult living donor liver transplantation at the Asan Medical
Center. Yonsie Medical
Journal 2004 15(6):1162-1168,
9.Takada
Y. Some aspects of adult
living donor liver transplantation: small-for-size graft and ABO mismatch. Hepatobiliary
Pancreat Dis Int 2009; 8(2): 121-123.
10.Saidi R, Elias N, Ko D, et al.
Live donor partial hepatectomy
for liver transplantation: is there a learning curve? Int J Org Transplant Med 2010; 1(3): 126-129
11.Chan S,
Fan S, Lo C, et al. Toward current standards
of donor right hepatectomy for adult-to-adult live donor liver transplantation
through the experience of 200 cases. Ann
Surg 2007; 245: 110–117
12.Durand F, Valla D. Assessment of the prognosis of cirrhosis: Child–Pugh
versus MELD. Journal of Hepatology 2005; 42: S100-S107.
13.Salame E, Kinkhawala M, Kapur S, et
al. Analysis of donor risk
in living-donor hepatectomy: the impact of resection type on clinical outcome.
American Journal of Transplantation 2002; 2: 780-788.
14.Campsen
J, Blei A, Jean C, et al.
Outcomes of living donor liver transplantation for acute liver failure: the
adult-to-adult living donor liver transplantation cohort study. Liver
Transpl 2008; 14:1273-1280.
15.Muller
S, Mehrabi A, Schmied B, et al. Partial liver transplantation-living
donor liver transplantation and split liver transplantation. Nephrol Dial
Transplant 2007; 22 (Suppl 8): viii13–viii22
16.Lo C, Fan S ,
Liu C, et al. Ten-year experience with liver transplantation
at Queen Mary Hospital: retrospective study. Hong Kong
Med J 2002; 8: 240-244
17.Liu C,
Fan S, Lo C, et al. Operative outcomes of adult-to-adult right
lobe live donor liver transplantation. a comparative study with cadaveric
whole-graft liver transplantation in a single center. Ann Surg 2006; 243:
404–410
18.Kawasak S, Makuuchi
M, Matsunami H, et al. Living related liver transplantation
in adults. Annals Of Surgery 1998; 227(2): 269-274
19.Nadalin
S, Bockhorn M, Malago M, et al. Living donor liver
transplantation. HPB 2006; 8: 10-21
20.Florman
S, Miller C. Live donor liver transplantation. Liver Transplantation 2006; 12:499-510.
21.Li C,
Mi K, Tianf W, et al. Outcomes of patients with benign liver
diseases undergoing living donor versus deceased donor liver transplantation. PLoS One 2011;6(11):e27366
22.Brown
R. Live donors in liver transplantation. Gastroenterology 2008;
134(6): 1802–1813.
23.Walter
J, Burdelski M, Bröring D. Chances and risks in
living donor liver transplantation. Dtsch Arztebl Int 2008; 105(6): 101–107
24.Bramstedt
K. Living liver donor mortality: Where do we stand?. Am J
Gastroenterol 2006;101:1–5
25.Azzam
A, Uryuhara K, Taka I, et al. Analysis of complications in hepatic
right lobe living donors. Ann Saudi Med 2010; 30(1):18-24
26.Aberg
F, Isoniemi H, Hِckerstedt K. Long-term results of
liver transplantation. Scandinavian Journal of Surgery 2011; 100: 14-21
27.Siddiqui
A, Jabeen R, Ansari M, et al. Spectrum of complications in post liver
transplant patients: a study of 30 cases. JLUMHS 2008, 124-12