ABSTRACT
Objectives: To describe and evaluate a modified evisceration procedure
that is thought to augment the scleral shell volume, allowing the use of a
larger-sized orbital implant, and enhancing the strength of the wound.
Methods: A
retrospective, descriptive, non-controlled study of evisceration with superior
post- equatorial sclerectomy, and patching the wound with autogenous scleral
graft was conducted. We reviewed the files and analyzed the data of 52 patients
(eyes) who underwent this technique from September 2003 to March 2011.
Results:
Out of
52 patients, 26 were female (50%) and 26 were males (50%). Age ranged from five
to 90 years with an average of 47.6 years. The type of implant was silicone in
49 patients and hydroxyapatite in three patients. The
diameters of the implants ranged between 14 and 20mm; four patients had 14mm,
14 patients had 16mm, 28 patients had 18mm, and six patients had 20mm implants.
The commonest indication for evisceration was trauma in 23 (44.2%) patients.
None of the patients had implant extrusion, exposure or migration. No scleral
patch melting or displacement was encountered. The mean follow up period was
35.9 months (1.25 -104).
Conclusion: Technique of evisceration
with post-equatorial sclerectomy and sclera patch graft was described. It was
found safe and useful for implantation of larger implants. However, further
comparative study is required.
Key words:
Autogenous Scleral Graft, Evisceration, Orbital Implant,
Sclerectomy
JRMS
December 2012; 19(4): 13-18
Introduction
Evisceration is an ablation surgical procedure
in which the entire contents of the globe are removed through a corneal,
limbal, paralimbal, or scleral incision. The removed contents include all
accessible uveal tissues (Iris, ciliary processes and ciliary body, and
choroid), retina, vitreous, and lens. The sclera, Tenon’s capsule, conjunctiva,
extra-ocular muscles, and the optic nerve and its surrounding meninges are not
excised.(1)
The evisceration can be done with or without the
removal of the cornea (keratectomy).(2)
The removal of the eye (ablation) results in
contracture and volume deficit that affects the anatomy and physiology of the
orbital tissues and orbital bones and can result in poor cosmetic outcome. Good
results from such surgery are not easy to achieve and a poor result can have
profound psychological implications for the patient for the rest of his life.
For that reason, orbital implant is placed in the orbital cavity during the
procedure to restore the orbital volume and prevent socket contracture that
allow the use of appropriate artificial eye that will be comfortable and not
apparent to the public at large.(3)
Evisceration is usually performed for functional
or cosmetic purposes. The main advantage of evisceration over enucleation,
which is the surgical removal of the globe from the orbital socket, in the
absence of ocular tumor and phthisis bulbi is that the procedure is simpler,
quicker, with less orbital manipulation and hemorrhage, reduced postoperative
swelling and pain, and associated trauma. Factors favoring evisceration over
enucleation are theoretically better eye movements and less chance of
postoperative enophthalmos.(4)
Evisceration is contraindicated in case of
intraocular tumors as it does not allow a complete, controlled removal of the
tumor and surgical margins are impossible to evaluate. It is also traditionally
contraindicated in eyes that are shrunken as a result of phthisis bulbi as the
sclera cannot hold an adequate sized implant, which is one of the main
determinant factors of good cosmetic results.(2)
The ablation of an eye and the subsequent
management of the anophthalmic socket still pose a considerable challenge for
the ophthalmic surgeon in spite of the numerous modifications of the standard
evisceration technique that allow the use of larger orbital implants and the
many recent advances in orbital materials.
We are presenting the outcome of a modified
evisceration technique that entails implantation of a ball, splitting the
sclera, and patching the wound using the excised scleral strip.
Methods
We reviewed the files of 52 patients (eyes) who
underwent the technique from September 2003 to March 2011 at the Royal Medical
Services Hospitals in Jordan.
Data reviewed included: age, gender, indication for evisceration, other eye
examination, implant type and size, postoperative complications and outcome, as
well as the follow up period length.
Surgical Procedure
The following is an account of how the technique
is performed in all patients reviewed at the Royal Medical Services Hospitals.
Patient is admitted as a day case. Surgery is performed under local anaesthesia
(with IV sedation) or general anaesthesia. After signing the informed consent
the correct eye is carefully identified and marked and photographed when
possible preoperatively and postoperatively. Topical anaesthesia (tetracaine
0.5%) eye drops is instilled into both eyes if surgery is performed under local
anaesthesia. Peribulbar block is achieved with the insertion of the needle
parallel to the inferior orbital floor and the second at the level of the
supra-orbital notch. A 10 ml of mixed anaesthetic solution of equal quantity of
lidocaine 2% with epinephrine (0.25 mg/20 ml) and bupivacaine 0.50% with epinephrine
(0.10 mg/20 ml) is injected. The patient is then prepped and draped. A Clarke's
lid speculum is placed. Using Westcott scissors, a 360 degree peritomy is
performed and undermining in the subconjunctival and sub- Tenon’s fascia planes
is carried out to the equator in the inferior half and behind the equator in
the superior half. An incision through the limbus is started using a sharp
blade followed by extension to each side with corneoscleral scissors. The wound
is extended to over 360 degrees and the cornea is removed with Steven’s
scissor. A cyclodialysis spatula is used to dissect the uveal tissues from the
sclera and the intraocular contents are removed using an evisceration spoon and
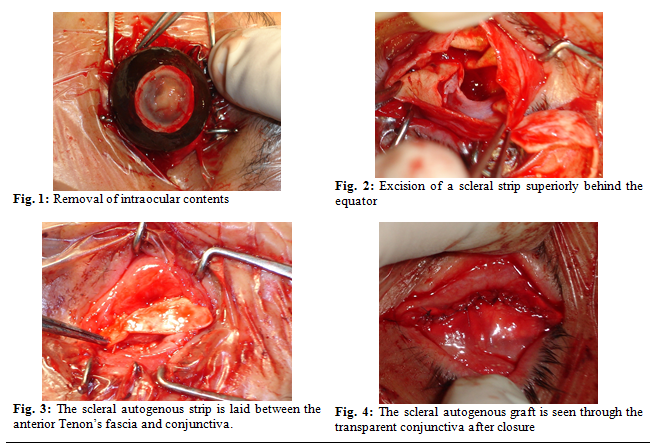
sent for histopathological examination. To maintain good view and haemostasis suction
and bipolar cautery are used (Fig. 1).
The scleral shell is thoroughly cleaned out with
cotton- tip applicators soaked with absolute alcohol (100% ethanol) to denature
any residue of uveal pigment and then rinsed thoroughly with saline solution.
Any source of bleeding is gently cauterized.
Horizontal relieving incisions are made in the sclera at five and 11
o’clock to allow the insertion of larger orbital implant.
About (3-5) X (10-17) mm strip of sclera is
marked horizontally at the equator behind the insertion of superior rectus
muscle and avoiding the superior oblique muscle insertion.
A stab incision is made using a sharp blade at the marked site and finished with Westcott scissors. The excised strip is trimmed and cleaned and kept in Gentamicin solution. The horizontal length of the harvested scleral graft is about 2 mm less than diameter of the planned orbital implant to prevent its migration (Fig. 2).
The commonest indication for evisceration
was trauma, 23 (44.2%) patients. None of the patients had implant extrusion,
exposure or migration. No scleral patch necrosis, melting, or displacement was
encountered. Orbital infection was not encountered in the study group. None of
the patients had sympathetic ophthalmia in the fellow eye. The mean follow up
period was 35.9 months (1.25 -104). Table IV shows follow up periods.
Discussion
Many
surgical modifications have been described to provide better cosmetic effect
and prosthesis motility after evisceration since it was first reported by James
Bear 1817.(5-7)
The
first review of routine evisceration was published by Noyes in 1874.(5-7)
Ten years later Mules inserted an implant into the scleral shell to restore the
orbital volume and prevent socket contracture that allow the use of appropriate
artificial eye that will be comfortable and not apparent to the public at
large.(5-7)
In
spite of the numerous modifications of the standard evisceration techniques
that allow the use of larger orbital implants and the many recent advances in
orbital materials implant extrusion and exposure is
still a major challenge for the ophthalmic plastic surgeon.
Many surgeons
recommend different techniques to prevent implant
extrusion like posterior sclerotomies, patching the
wound with temporalis fascia,(8) or wrapping the implant with
autogenous sclera like enucleation
with reverse replacement of sclera as an alternative to conventional
evisceration.(9)
In the standard technique of
evisceration, the size of the implant is usually between 14 to 16 mm, thus it
cannot guarantee a tight implantation, as scleral shrinkage may occur during
the healing periods.(10) Modified evisceration techniques
have therefore been developed, mostly involving additional scleral incisions posteriorly
that allow the placement of larger implants while reducing exposure rates.(11-16)
Our technique is as effective as Kim
et al(11) procedure, who described a
primary evisceration with four anterior relaxing incisions and posterior
sclerotomies made circumferentially behind the equator at approximately 330º,
combined with porous polyethylene orbital implant placement, and found to be a
useful technique for treating a variety of end-stage eye diseases with no
exposure or extrusion of implant over 8 years. Kim et al performed computed
tomography to confirm orbital implant migration; none of the patients in this
series had orbital computed tomography.
Huang et al,(12)
described another modified evisceration technique with scleral quadrisection
and porous polyethylene implantation. In their study there was no case of
conjunctival dehiscence, implant extrusion, implant exposure, significant
enophthalmos, superior sulcus deformity, or orbital cellulitis. This series shows comparable results, apart from the cosmetic appearance and
implant mobility which were not reported. Another technique described by Sales-Sanz
and Sanz-Lopez consisted of a 4-petal scleral sectioning from the limbus to the
optic nerve, with release of the sclera from the optic nerve.(13)
Adenis
et al.,(14) described a new technique of evisceration
after resection of the corneal epithelium and limbus, with preservation of the
posterior layer of the cornea and anterior sclera, after a 360° dissection of
the sclera behind the insertion of the extra ocular muscles, and preservation
of the insertions of the rectus muscles. The technique was designated “Parachute”
when the posterior sclera was excised, and “Russian doll” when the posterior
sclera was preserved and is behind the orbital implant. The implant was
inserted at the end of the procedure with a “birdcage” forceps. Massary and Holds,(15) performed two
full-thickness sclerotomies from the anterior limbus incision to the optic
nerve in the inferonasal and superotemporal quadrants to create two scleral
flaps with release of the sclera from them. The most recent modification was
described by Georgescu et al.,(16) who described an evisceration with
equatorial sclerotomy for phthisis bulbi and microphthalmos concluding that
this procedure could be a useful adjuvant for placement of a larger orbital implant
at the time of evisceration in patients with phthisis bulbi and microphthalmos.
Long et al.17 described a modified evisceration technique
with trans- scleral hydroxyapatite spherical implant placement. Their procedure
is based on cutting the sclera antero-posterior to the optic nerve, which is
divided, inserting a 16-20mm hydroxyapatite spherical implant and everting the
posterior scleral layers in front of the implant. The anterior half of the implant
is covered by double layers of sclera while the posterior sclera is opened to
the orbital tissues, facilitating the integration of porous implant tissue.
Their procedure is suitable for hydroxyapatite orbital implant only while our
procedure suites all types of orbital implants as it covers the implants from
posterior and anterior surfaces and provides a superior window for direct
integration of porous implant.
The
technique described in the present study involves two steps: first, excising a strip of the sclera behind the equator
to augments the ocular volume and permits insertion of a larger implant. This
minimizes the risk of developing post enucleation socket syndrome, and decreases
the tension on the wound. It also increases surface contact between porous implants
and the orbital tissue, which may facilitate more vascular integration. Second is patching
the scleral wound with the excised scleral strip which gives the implant an
additional layer of protection against exposure.
The scleral graft was laid between
the anterior Tenon’s and the conjunctiva to reduce the risk of scleral graft
melting.
During follow up, none of our
patients had implant extrusion or exposure, scleral patch melting or
displacement, or orbital infection. All fellow eyes showed no signs of
sympathetic ophthalmia.
Conclusion
The
modified evisceration technique described is as effective as other
modifications reported in the literature. It probably provides a wider scleral
shell to accommodate a bigger implant, and adds to the strength of the wound to
decrease the incidence of extrusion attributed to wound dehiscence. A
controlled comparative study is needed to further solidify these results.
References
1.Chen
WP. Evisceration. In: Chen WP, editor.
Oculoplastic surgery: The essentials. New
York: Thieme; 2001; 347-355.
2. Jeffrey
AN. Enucleation, evisceration and
exenteration: The care of the eye socket. In: Jeffrey AN, editor. Oculoplastic
surgery: The requisites in ophthalmology. St.
Louis: Mosby; 2001. P. 419- 445.
3.Leatherbarrow
B. Enucleation and evisceration. In:
Leatherbarrow B, editor. Oculoplastic surgery. London: Martin Dunitz; 2002; P. 305-317.
4.Hansen AB, Petersen C, Heegaard
S, Prause JU.
Review of 1,028 bulbar eviscerations and enucleations. Changes in aetiology and
frequency over a 20-year period. Acta Ophthalmol Scand 1999; 77:331–335.
5.Timothy NH, Freilich DE, Linberg JV. Evisceration versus
enucleation from the ocularist’s perspective. Ophthal Plast Reconstr Surg
2003; 19:417– 420.
6.Limbu B, Saiju R, and Ruit S. A retrospective study
on the causes for evisceration at Tilganga Eye Centre. Kathmandu University
Medical Journal 2009; 7(2):115-119.
7.Deborah DS. History of enucleation
and evisceration in ophthalmic surgery: principles and techniques. 2nd ed.
Blackwell 1999; 1553-1562.
8.Denoyer A, Ranguin M, Boulet F, Pisella PJ. Repair of exposed hydroxyapatite implants using temporalis fascia: four case
reports. J Fr Ophtalmol 2005; 28(9):976-980.
9.Madill SA, Maclean H. Enucleation with Reverse Replacement of Sclera as an Alternative to
Conventional Evisceration. Orbit 2005; 24(1): 23-28.
10.Yang JG, Khwarg SI, Wee WR, et al. Hydroxyapatite
implantation with scleral quadrisection after evisceration. Ophthalmic Surg
Lasers 1997; 28:915–919.
11.Kim KH, Lee H, Park M, et al. Evisceration with four
anterior relaxing incisions and circumferential posterior sclerotomies with
porous polyethylene orbital implants: an 8-year study. Acta Ophthalmol 2011; 89(7):686-690
12.Huang D, Yu Y, Lu R, et al. A modified evisceration
technique with scleral quadrisection and porous polyethylene implantation. Am
J Ophthalmol 2009; 147: 924-928.
13.Sales-Sanzm
M, Sanz-Lopez A. Four-petal evisceration: a new technique. Ophthal Plast Reconstr Surg 2007; 23(5): 389-392.
14.Adenis
JP, Rulfi JY, Robert PY. Surgical technical note:
Evisceration using the Russian-doll technique and the parachute technique. Operative techniques in oculoplastic, Orbital and Reconstructive Surgery 2001; 4(1): 25-29.
15.Massary GG, Holds JB. Evisceration with
Scleral Modification. Ophthalmic
Plastic & Reconstructive Surgery 2001;
17(1): 42-47.
16.Georgescu D, Vagefi MR, Yang CC, et al. Evisceration
with equatorial sclerotomy for phthisis bulbi and microphthalmos. Ophthal Plast Reconstr Surg 2010; 26(3):165-167.
17.Long
JA, Tann TTM, Girkin CA. Evisceration: a new technique of trans-scleral
implant Placement. Ophthal Plast Reconstr Surg 2000; 16(5):322.