ABSTRACT
Objective: The purpose of the
study is to identify the pharmacist's awareness and the contributing factors of
drug counterfeiting in Jordan.
Method: The study used a descriptive cross-sectional design.
Study participants included a convenience sample of 100 Jordanian pharmacists
who worked in three different fields of pharmacy including community,
industrial and quality control in Amman.
The data were collected by a self report questionnaire which was developed by
the authors and was composed of open and closed ended questions. The validity of questionnaire was assessed by
experts in the field of the pharmacy working in the Jordan Food and Drug
Administration with no
modification and it was piloted and tested on four pharmacists. The response
rate was 62%. The data were analyzed by using the Statistical Package for
Social Sciences.
Results: The results showed that around 76% reported high awareness of drug
counterfeiting problem and the current laws and regulations in Jordan and 54.8%
perceived the regulations are extensive enough. The majority (63%) of the
respondents did not come across any case of counterfeiting themselves, while 37%
had come across counterfeit cases and 50% of them had come across several
cases. About half (51%) of the respondents thought that drug counterfeiting is
not a serious problem while 48.4% thought it is a very serious problem. In
addition to that, 54.8% thought that it is difficult to invade the Jordanian
market with counterfeit drugs while 35.5% think that Jordan could be invaded easily.
Conclusions: This study supports
that drug counterfeiting is a
major health problem and has a major impact worldwide on public, pharmaceutical
companies as well as governments. It also emphasizes that more statistical
databases and national research on the percentage of drug counterfeiting in
Jordan are needed to analyze and facilitate monitoring the size of problem.
Key words: Awareness, Drug
counterfeiting, Pharmacist
JRMS June 2013;
20(2): 57-70 /DOI: 10.12816/0000079
Introduction
Improving the quality of health services depends on many factors one of
which is providing drugs; therefore they have to be available at all times and
reachable to all population. Access to medicines especially for developing
countries is still a big challenge because of their high prices, causing
patients in these countries to seek alternative cheap sources thus making patients
more vulnerable to counterfeit medicines.
On the other hand, the new technologies in developed countries expose
their patients to criminals dealing with counterfeit medicines mainly through
the internet by fake advertisement about medicines.
The World Health Organization (WHO) estimates that medicines purchased over
the internet from sites that conceal their physical address are counterfeit in
over 50% of cases.(1) Counterfeit drugs are a global public
health problem, causing death, disability and injury affecting both adults and
children. However,
defining the true extent of the problem is difficult and not really known since
no global study has been carried out. It
is clear from individual country studies that counterfeiting is a major world problem,
but the variety of information sources makes compiling and comparing statistics
a difficult task, also some countries and drug companies keep information they
have strictly confidential so as not to lose their reputation.(2) In
this respect, the capacity now to collect and analyze data has improved since the WHO launched a campaign to fight
drug counterfeiting and a task force called International Medical Products
Anti-Counterfeiting Task force (IMPACT) which was set up in 2006. For almost 20
years, the WHO has been fighting drug counterfeiting since it was first known
around 1990 and it appears to be a growing problem in both developing and
developed countries. No country is free of this problem. The phenomenon has
been growing in recent years due to the fact that counterfeiting methods are
becoming more sophisticated.(3) Counterfeit medicines are
estimated as more than 10% of the global medicines market and in some
developing countries it is thought to be as high as 50% as a result of lack
legislations, poor enforcement of drug law, weak national drug regulatory
authorities and shortage of drugs. One prediction is that global counterfeit
drug sales will reach $75 billion by 2010 more than 90% since 2005.(4)
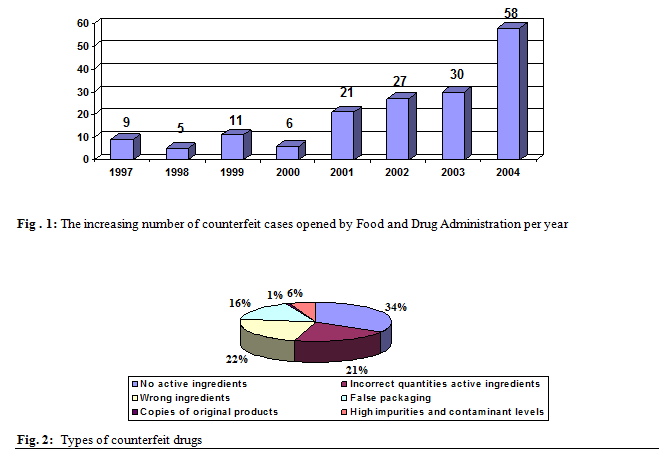
Figure 1 shows the increasing numbers of counterfeit cases reported in FDA
Counterfeit Drug Task Force Report: 2006 update.
Counterfeiting can be applied to both branded and generic products;
counterfeit products could include products without active ingredients (32.1%);
with incorrect quantities of active ingredients (20.2%); wrong ingredients
(21.4%); with correct amounts of active ingredients but false packaging
(15.6%); copies of original products (1%) and products with high impurities and contaminant levels (8.5%) .(5) These classes represent the different types of counterfeit drugs as shown in Figure 2.
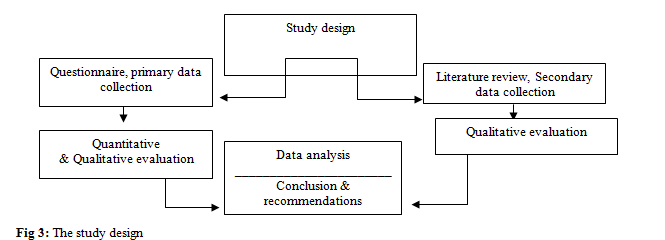
Table I: The field of work of the
respondents
|
Respondents field
|
No. of respondents
|
%
|
|
Community pharmacist
|
47
|
75.8
|
|
Industrial pharmacist
|
11
|
17.7
|
|
Quality control pharmacy
|
4
|
6.5
|
|
Total no. of questionnaire
|
62
|
100
|
There is no
universal definition of counterfeit drugs; the definition varies from country
to another, this limits the exchange of information between countries and
limits the understanding of the true extent of the problem globally.(6)
As a consequence
of this the WHO drafted a definition in 1999 which provides common universally
accepted basis for drug counterfeiting to enhance understanding of the problem
at global level: "А counterfeit medicine is one which is deliberately
and fraudulently mislabelled with respect to identity and/or source.
Counterfeiting can apply to both branded and generic products and counterfeit
products may include products with the correct ingredients or with the wrong
ingredients, without active ingredients, with insufficient active ingredients
or with fake packaging."
Therefore, this study was conducted to identify
pharmacist awareness and the contributing factors of drug counterfeiting in Jordan.
Methodology
The
study was designed to identify pharmacist awareness and the contributing factors
of drug counterfeiting in Jordan and to suggest possible ways to combat
the problem. One of the most efficient ways to address this objective is to
complete a questionnaire, in addition to collecting information from the Jordanian
Food and Drug Administration (JFDA). However, there was difficulty in
collecting the required information from the JFDA, in addition to the limited
published data related to the actual situation in Jordan.
The study design was based on qualitative and quantitative evaluation
collected from the questionnaire, then the data collected was analysed to come
up with results and conclusions as shown in Figure 3.
The questionnaire consisted of open ended and close
ended questions; a first draft of the questionnaire was piloted and tested on
four respondent pharmacists from Jordan. The questionnaire is shown
in Appendix 1. The validity of the tool
was assessed by experts in the field of the pharmacy with no modification. The
study was conducted in Amman. The method of data collection was by a self
reported questionnaire through distribution of the questionnaire to the
participants in the field.
The sample size for this study was a total of 100
pharmacists selected from three different fields of pharmacy including
community, industrial and quality control.
Table II: Are there penalties for drug counterfeiting?
|
Respondent’s opinions
|
|
No. of respondents
|
%
|
|
|
Yes
|
39
|
62.9
|
|
No
|
20
|
32.3
|
|
Total
|
59
|
95.2
|
|
|
Missing
|
3
|
4.8
|
|
Total no. of questionnaires
|
62
|
100.0
|
Table III: Penalties
for drug counterfeiting
|
Respondent’s answers
|
No.
of respondents
|
%
|
Penalty
|
|
Identified
Not
identified
|
9
53
62
|
14.5
85.5
100
|
Closure
of the pharmacy
Total
|
|
Identified
Not
identified
|
12
50
62
|
19.4
80.6
100
|
Prison
for a period of time
Total
|
|
Identified
Not
identified
|
12
50
62
|
19.4
80.6
100
|
Payment
of a certain range of fine
Total
|
Most respondents were working in community pharmacies
as shown in (Table I) and 51.6% of respondents were males and 48.4% were
females. Their mean age was 35 years. The
questions were analyzed by using the SPSS system. The open ended questions were
summarized first as shown in Appendix 2, and the most common answers were taken
as variables as shown in Appendix 3.
Ethical Consideration
The proposal was submitted to the ethics committee of
the Ministry of Health in Jordan
for their formal permission and approval was secured.
Results
One hundred copies of the questionnaire were
distributed by personal delivery with the assistance of four colleagues in Jordan. Sixty-
two copies were completed and returned making the study response rate 62%.
Participant
awareness of the drug counterfeiting laws and regulations:
The data analysis showed that 76% of respondents are
aware of drug counterfeiting problems and the current laws and regulations in Jordan.
However, there are differences in opinions about whether the regulations are
extensive enough or not; 54.8% of respondents thought that they
are while 43.5%
thought that they are not enough. Of the 15 respondents out of 27 respondents
that did not think that the current laws and regulations are enough made suggestions
to improve the situation. They suggested
improving regulations on borders and performance of quality control tests, in
addition to increasing the penalties (10 participants), increase the public
awareness (3 participants), coordination between control bodies and more
international efforts (1 participant), and finally fight favouritism (1
participant).
Around 63% of the respondents did not come across any
case of counterfeiting themselves, on the other hand, 37% come across
counterfeit cases of which more than 50% had come across several cases. Despite
the pharmacists’ awareness about the drug counterfeiting laws and regulations being
good, it is not reasonable that around one third of them after excluding the
missed answers (Table II), believe that there are no penalties on trading of
counterfeit drugs in Jordan and this could be a serious situations for these
pharmacists, especially when we know that most of the respondents were
community pharmacists which are the main target for counterfeiters. If the
spread of such an idea is popular among a large group of pharmacists, there
should be an urgent need for more efforts to increase the general awareness about
the problem and its implications.
Table IV: The degree
of seriousness of drug counterfeiting
|
Respondent’s opinions
|
No. of respondents
|
%
|
|
Very serious
|
30
|
48.4
|
|
Least serious
|
32
|
51.6
|
|
Total
|
62
|
100.0
|
Table V: The
vulnerability of invasion by counterfeit drugs
|
Respondent’s opinions
|
No. of respondents
|
%
|
|
Very easy
|
3
|
4.8
|
|
Easy
|
22
|
35.5
|
|
Difficult
|
34
|
54.8
|
|
Very difficult
|
2
|
3.2
|
|
Total
|
61
|
98.4
|
|
Missing
|
1
|
1.6
|
|
Total
|
62
|
100.0
|
The respondents who knew that there are penalties for
drug counterfeiting gave different ranges of penalties that varied from the
closure of the pharmacy to prison for a certain period of time and payment of a
certain range of fine (Table III), but without giving the exact range of
penalty for both time and fine payment. For the respondents who know that there
are penalties for drug counterfeiting, around 61% of them believe that the
existing penalties are enough while around 39% thought that they are not
enough. Eight pharmacists, out of 22 respondents that did not think that the
existing penalties for drug counterfeiting are enough, made suggestions to
improve the situation by increasing fine payments and the period of imprisonment
(4 participants), withdrawal of the licence of pharmacists who are involved in
drug counterfeiting and not allowing them to work in this field again (3
participants), and finally only one pharmacist made a suggestion that the
existing penalties are enough, but there is lack of strong commitment to their
implementation.
Factors that might encourage drug counterfeiting:
The three major causes of drug counterfeiting
according to the respondents were high prices of drugs (48%), lack of
supervision and poor quality control lab tests (35.5%), and poor public
awareness (16.5%). Regarding the degree of seriousness of the problem and vulnerability
of invasion, the majority of the respondents thought that drug counterfeiting
is a less serious problem (51.6%) while 48.4% thought it is a very serious
problem. In addition to that, 54.8% thought that it is difficult to invade Jordan by counterfeit drugs while 35.5% thought
that Jordan
could be invaded easily (Table IV & V). These
variations in opinions may be due to the differences of pharmacists' experience
and exposure to drug counterfeiting. Drugs that are susceptible to be
counterfeited varied between three major groups of drugs: most of the answers
showed that the drugs used for chronic diseases such as hypertension,
diabetes and hyperlipidemia are more susceptible for counterfeiting, followed
by expensive drugs such as sex enhancers, antiplatelets,
Central Nervous System drugs, anticancer and antipsychotic drugs, and finally
fast moving drugs such as analgesics, Non Steroidal Anti Inflammatory Drugs (NSAID)
and antibiotics.
Discussion
Drug counterfeiting is a global problem; it has been
reported in developing countries such as India, Peru, Niger, Nigeria, Southeast
Asia and Pakistan as well as first world countries such as Unites States which
resulted in establishing the Counterfeiting Drug Task Force.
Drug counterfeiting is a major health problem and has
a major impact worldwide on the public, pharmaceutical companies as well as
governments.
The FDA estimates that counterfeits make up more than
10% of the global market. Developing
countries seem to be most affected,and counterfeiters invade most drugs, especially those which are used for the treatment of serious diseases. Jordan like many other countries has this problem; however its size is below the world average.
Table IV: Recent examples of counterfeit medicines:
|
Counterfeit medicine
|
Country/Year
|
Report
|
|
1. Avastin (for cancer treatment)
|
United
States of America, 2012
|
Affected 19 medical practices in the USA. The drug
lacked active ingredient
|
|
2. Viagra and Cialis (for erectile
dysfunction)
|
United
Kingdom, 2012
|
Smuggled into the UK. Contained
undeclared active ingredients with possible serious health risks to the
consumer
|
|
3.Truvada and Viread (for HIV/AIDS)
|
United
Kingdom, 2011
|
Seized before reaching patients. Diverted
authentic product in falsified packaging
|
|
4. Zidolam-N (for HIV/AIDS)
|
Kenya, 2011
|
Nearly 3,000 patients affected by
falsified batch of their antiretroviral therapy
|
|
5. Alli (weight-loss medicines)
|
United
States of America, 2010
|
Smuggled into the USA.
Contained undeclared active ingredients with possible serious health risks to
the consumer
|
|
6. Anti-diabetic traditional medicine
(used to lower blood sugar)
|
China, 2009
|
Contained six times the normal dose of
glibenclamide. Two people died, nine people were hospitalized
|
|
7. Metakelfin (antimalarial)
|
United Republic of Tanzania,
2009
|
Discovered in 40 pharmacies. The drug
lacked sufficient active ingredient
|
Jordan like many other countries has a smuggling problem of counterfeit
drugs; however no accurate statistics appear to be available; for example in a presentation for stakeholders
Meeting of Transparency Alliance (MeTA) in London last year Nuseirat
(7) (Head of National Drug Unit in JFDA) said that problems with counterfeit drugs was less than 5% of
the world average and that no accurate statics were available but that it could
be a growing problem. Arab Reporters for Investigative Journalism (ARIJ)
mentioned that it is below the world average by 15% and pointed out that it is a decreasing
problem due to the efforts from all concerned parties like MOH, JFDA,
Jordanian Pharmaceutical Association (JPA), law enforcement agencies in
collaboration with public security, Customs and health agencies. However, on these figures smuggling and counterfeit drugs on the
Jordanian pharmaceutical market are below the world average.(7)
Overall, the
problem does not lie in the exact percentage numbers, but in the harm caused by
these counterfeit drugs through dangerous effects ranging from minor problems
to death especially when they are given to those in dire need of a medical
intervention and in saving lives.(5-8) For example, a
total of 192,000 Chinese patients are reported to have died in 2001 from fake
drugs and in the same year Chinese authorities closed 1.300 factories while
investigating 480,000 cases of counterfeit drugs worth 57 million USD and in
2004, Chinese authorities arrested 22 manufacturers of grossly substandard
infant milk powder and closed three factories after the death of over 50
infants.(9)
In Europe, counterfeit medicines available originally
focused upon ‘lifestyle’ medicines, including erectile dysfunction and weight
loss medicines. Counterfeiters are now also focusing on ‘lifesaving medicines’
including cancer and heart medicines. The European Union's 2007 pharmaceutical
counterfeiting data shows that almost 40 per cent of counterfeit medicines
seized by the EU originated in Switzerland,
making the country the biggest importer of counterfeit medicines into the EU; India and the United Arab Emirates were second
and third, respectively. The total volume of counterfeit pharmaceuticals seized
by EU officials rose 51% in 2007. The highest numbers of items were seized in Belgium, France,
Britain,
and Spain.(10)
Weight and hair loss tablets, antidepressants, painkillers,
anabolic steroids worth more than a quarter million pounds ($350,000 USD) worth
of counterfeit, unlicensed, withdrawn, and controlled drugs were seized in England by the
Medicines and Healthcare products Regulatory Agency (MHRA). The drugs are
believed to be linked to an illegal online pharmacy selling prescription-only
medicines around the globe. A further 250,000 pounds worth fake drug stash
seized in an undercover operation.(11) The problem of
counterfeit drugs was addressed internationally in Nairobi at the WHO Conference of Experts on
the Rational Use of Drugs in 1985 for the first time.(12) Recent
examples of counterfeit medicines are shown in Table VI.
Conclusion and
recommendations
From the questionnaire and the information found, it
is possible to propose the following recommendations and implications of
findings for future research:
·
More statistical databases and national research
on the percentage of drug counterfeiting in Jordan are needed to analyze and
facilitate monitoring the size of problem.
·
There needs to be strong commitment, shared
responsibility and coordination from all control bodies with special emphasis
on the three major diseases in Jordan
namely, hypertension, diabetes and hyperlipidimia.
·
There should be improved international
collaboration to help in combating counterfeiting problem especially that the
situation is not so good in the neighboring countries which have close borders
with Jordan.
·
It would be beneficial to have improvement in
the quality control departments, but this would require increasing resources
and the use of new technologies to facilitate detection of counterfeit drugs.
· A review
should take place which determines whether the existing laws and regulations
are extensive enough and the penalties are appropriate.
· The JFDA
should consider increasing the pharmacists and public awareness in this field
by making better advertising campaigns.
Joint efforts of authorities
at country level in Jordan have been increased recently including making
regular raids not only on pharmacies but also on beauty salons, increasing the
number of inspectors and making new amendments on the law of circulating drug
counterfeiting by increasing penalties, all these contribute to the drop of
drug counterfeiting in Jordan recently. However, it is suggested that the fight against drug counterfeiting is a
shared responsibility between all parties to include: authorities, the industry,
distributors and consumers and not the authorities’ responsibility only. To
achieve this goal an increase in awareness through campaigns is needed to
target all concerned parties with special emphasis on the general public who
presently have little knowledge on detecting counterfeit medicines.
The public should then be
encouraged to inform responsible authorities such as the JFDA and police,
particularly when there is an adverse reaction after taking medication or when
they suspect any person to be selling or supplying drugs illegally.
References
1.World Health Organization. Substandard and
Counterfeit Medicines. World Health Organization, 2003; Fact Sheet No. 275.
2.Wertheimer, IA,
Santella, MT, Chaney, MN. Counterfeit
Pharmaceuticals – Update on Current Status and Future Projections. Business
Briefing. Pharmageneric 2004; pp. 1-9.
3.World Health Organization. WHO launches taskforce
to fight counterfeit drugs, Geneva,
Switzerland,
2006.
4. Food
and Drug Administration. Combating Counterfeit
Drugs: A report of the Food and Drug Administration. U.S. Department
of Health and Human Services, 2006.
5.World Health Organization. Counterfeit Drugs Kill.
IMPACT final brochure updated May, 2008.
6.World Health Organization. General information on
counterfeit medicines. World Health Organization, Geneva, Switzerland,
2006c.
7. Nuseirat A. Jordan presentation
towards a medicines transparency. Available on line from www.dfidhealthrc.org/MeTA/documents/17%20april%20documents/Jordan%20presentation%20on%2017%20April.ppt, 2008. [Accessed 25th June 2009]
8.World Health Organization Jordan. Country cooperation
strategy Available on line from: www.who.int/countries/jor/en/.2007, [accessed 1st
July 2009].
9.Cockburn,
R, Newton, PN,
Agyarko, KE, et al. The Global Threat of Counterfeit Drugs: Why
Industry and Government Must Communicate the Dangers. Public Library of
Science 2005; 2 (4).
10.Taylor N.
40% of EU counterfeit drugs seizures of Swiss origin: In-pharm.technologist.com.
2008.
11.Primo-Carpenter J. Matrix of drug Quality Reports in USAID-assisted countries,
U.S Pharmacopoeia Drug Quality and Information Program Updated June, 2009.
12.Shahverdi SH, Hajimiri M,
Pourmalek F, et al. Iranian pharmacists’ knowledge, attitude and practice regarding
counterfeit drugs. Iranian J Pharm Res 2012; 11(3): 963-968.
Appendix 1
Questionnaire on
drug counterfeiting designed to study the current status and the size of
problem in Jordan,
I would therefore be grateful for you help by completing this questionnaire:
Please answer each
question by placing a tick in the appropriate box. (The estimated time for
completing the questionnaire is 15 minutes).
1. What field of
pharmacy do you work on?

 Community pharmacist Industrial pharmacist Quality control pharmacy
Community pharmacist Industrial pharmacist Quality control pharmacy
2. Are you aware of the current law and regulations of drug
counterfeiting?

 Yes
No
Yes
No
3. Have you come across any direct experience of drug counterfeiting?
Yes
No
If yes please give details:
One
case two cases several cases substandard drugs
4. What factors do you think that might encourage drug counterfeiting?
5. Do you think the current law and regulations of drug counterfeiting
are enough?
Yes
No
 If no, and if you have a chance to improve the
situation or make any changes, please give suggestions for improvement
If no, and if you have a chance to improve the
situation or make any changes, please give suggestions for improvement
6. What do you think the degree of seriousness of drug counterfeiting
problem in Jordan?
Very serious least
serious
7. What types of drugs or diseases are more likely susceptible to drug
counterfeiting?
8. How vulnerable do you think Jordan can be invaded by drug
counterfeiting?
 Very
easy Easy Difficult Very difficult
Very
easy Easy Difficult Very difficult
9. Are regulations for drug counterfeiting the same for imported and
local manufactured drugs?
Yes
No
10. A. Are there penalties for drug counterfeiting?
Yes No
If yes, do you know different ranges of penalties?
10. B. Do you think that they are enough?
Yes
No
If no, please give suggestions

Thanks for your time.
Appendix 2
Questionnaire
open questions
|
Questionnaire
Number
|
Factors
that encourage drug counterfeiting
|
Suggestion
to improve situation
|
Types
of counterfeit drugs
|
Ranges
of penalties
|
Suggestion
to improve penalties
|
|
1.
|
Lack of supervision. Expensive drugs.
|
-
|
Hypertension drugs. Psychiatric drugs.
|
-
|
-
|
|
2.
|
No
public awareness.
|
-
|
Heart disease
drugs.
|
Closing the pharmacy. Paying fine penalties.
|
-
|
|
3.
|
Weak regulations.
High prices of drugs.
|
-
|
Expensive drugs.
|
|
|
|
4.
|
-
|
-
|
-
|
-
|
-
|
|
5.
|
Corruption,
to make money.
No
supervision.
Weak
borders.
|
-
|
Cardiovascular
diseases.
Expensive
drugs.
|
-
|
-
|
|
6.
|
Lack of
public awareness.
Invasion
of pharmaceutical field by non certified persons.
Variations
of medicines prices.
|
Fighting
favouritism
|
Sexual
enhancers.
Analgesics.
Psychiatric
drugs.
|
-
|
-
|
|
7.
|
Poor
awareness.
|
-
|
Pain
killers, Analgesics.
Antibiotics.
|
-
|
-
|
|
8.
|
High
prices of drugs.
Absence of
applications of law.
|
-
|
Heart
disease drugs.
|
-
|
-
|
|
9.
|
-
|
-
|
-
|
-
|
-
|
|
10.
|
High
prices of drugs.
To make
money.
Corruption
(lack of commitment of existing law).
|
-
|
Sexual
enhancers.
Heart
disease drugs.
Drugs used
for chronic diseases.
|
Fine
penalties.
Jail.
|
-
|
|
11.
|
Invasion
of pharmaceutical field by non certified people.
Lack of
supervision.
The
increase in the no. Of pharmacies opened to public.
|
-
|
-
|
-
|
-
|
|
12.
|
Lack of
pharmacist awareness.
Poor QC
tests of each batch.
|
-
|
-
|
-
|
-
|
|
13.
|
Lack of
pharmacist awareness.
|
-
|
Analgesics
and cold preparations.
|
-
|
-
|
|
14.
|
Expensive
drugs.
Rapid gain
of money.
|
More
regulations on borders. More control
on the internet.
Public education.
|
Expensive
drugs.
|
Closing
the pharmacy.
Withdrawal
of licence.
Payments
of penalties and jail.
|
-
|
|
15.
|
-
|
-
|
Antibiotics.
|
-
|
-
|
|
16.
|
The
increase in the no. Of pharmacists.
High
margin profit.
Poor
community culture.
|
-
|
Chronic
disease drugs (antihyperlipidemia, hypertension).
Expensive
drugs.
Cosmetics.
|
-
|
-
|
|
17.
|
High
prices of drugs.
Poor QC
lab. Tests.
Poor
control from health authorities.
|
Improvement
of QC lab. Performance.
Monitoring
of imported products.
|
Chronic
diseases (diabetes, hypertension).
Antibiotics.
NSAID.
|
Closing
the pharmacy.
|
Make
more international efforts.
Treat
drug counterfeiting as narcotics.
|
|
18.
|
High
prices of drugs.
To gain
money.
Implementation
of TRIPS doesn’t allow local industry to produce new drugs.
|
International
efforts.
Treat drug
counterfeiting as narcotics.
|
Diabetes
drugs.
Antiplatelet.
Hypertension.
NSAID.
|
Jail.
|
Make
more international efforts.
Treat
drug counterfeiting as narcotics
|
|
19.
|
High
prices of drugs.
Quick
profits.
Lack of
awareness.
|
-
|
Chronic
diseases.
Expensive
drugs.
Weight reduction
products.
|
-
|
Increase
the penalties up to 50,000 JD.
Increase
prison period to 3 years.
|
|
20.
|
High
prices of drugs.
Lack of
awareness.
|
-
|
Hypertension
and heart diseases
|
-
|
-
|
|
21.
|
High
prices.
Low
availability of drugs in the market.
|
-
|
Diabetes.
Hypertension.
Chronic
heart diseases.
|
-
|
-
|
|
22.
|
Lack of
supervision.
Profits.
Lack of
ethical awareness of some pharmacists.
|
-
|
Expensive
drugs.
Hypertension,
antilipids.
Cardiovascular
diseases.
Erectile
dysfunction
|
Closing
the pharmacy.
|
-
|
|
23.
|
Expensive
drugs.
|
-
|
Imported
drugs.
|
Penalties,
withdraw of licence.
Jail.
|
-
|
|
24.
|
To make
money.
|
Increase
the penalties.
Increase
awareness.
|
Chronic
disease medications.
|
-
|
-
|
|
25.
|
Lack of
supervision.
|
-
|
-
|
-
|
-
|
|
26.
|
Expensive
drugs.
|
-
|
-
|
-
|
-
|
|
27.
|
Lack of
supervision.
Low
availability of drugs.
|
-
|
-
|
-
|
-
|
|
28.
|
Lack of
supervision.
|
-
|
-
|
-
|
-
|
|
29.
|
Lack of
supervision.
|
-
|
-
|
-
|
-
|
|
30.
|
Drug
abuse.
Poly
pharmacy.
|
Increase
awareness.
|
Hypertension.
Vitamins.
|
-
|
-
|
|
31.
|
To make
money.
High taxes
of drugs make it expensive for pharmacists.
|
Close
pharmacies.
|
Hypertension.
Antilipids.
Cardiac
diseases and diabetes.
|
-
|
-
|
|
32.
|
Not enough
penalties and law.
|
-
|
Antibiotics.
Chronic
diseases (HT and hyperlipidemia).
|
Pay money
200-1000 JD.
Close
pharmacy from 1 week -6 months.
|
Withdraw
licence and not allow the pharmacists to work again.
|
|
33.
|
Lack of
supervision.
Low QC standards.
Expensive
drugs.
|
Increase
penalties.
|
HT,
antilipids.
Antibiotics.
|
Payments.
Jail.
|
Withdraw
licence and not allow the pharmacists to work again.
|
|
34.
|
-
|
-
|
Antibiotics
and cold preparations.
|
-
|
-
|
|
35.
|
Lack of
supervision.
High prices
of drugs.
Lack of
awareness.
|
-
|
Sexual and
impotency drugs.
Chronic
diseases and CVS drugs.
CNS drugs.
|
Pay money.
Jail.
|
-
|
|
36.
|
High
prices of drugs.
Fast
movement of drugs.
|
More
control for imported drugs.
|
HT,
diabetes, CVS, obesity drugs and hyperlipidemia.
|
--
|
-
|
|
37.
|
-
|
-
|
-
|
-
|
-
|
|
38.
|
High
prices.
Poor
awareness.
|
-
|
Antibiotics.
Analgesics.
|
-
|
-
|
|
39.
|
-
|
-
|
Antibiotics.
Diabetes.
|
-
|
-
|
|
40.
|
Limitations
on generics
|
-
|
Expensive
drugs.
|
-
|
-
|
|
41.
|
Drug
smuggling.
Limitations
on generics.
|
Make
generics more elastic and join agreements.
|
Expensive
drugs.
|
-
|
Implementation
of penalties must be restricted.
|
|
42.
|
Profits.
Lack of
supervision.
|
-
|
Antiplatelets (plavix).
Sexual drugs (cialis).
Antihyperlipid
and diabetes.
|
-
|
-
|
|
43.
|
Profits.
Lack of
supervision.
|
-
|
Expensive
drugs (plavix, cialis).
|
-
|
-
|
|
44.
|
Profits.
Lack of
supervision.
|
More
control.
Withdraw
of pharmacist licence.
|
Expensive
drugs.
HT,
diabetes.
|
-
|
-
|
|
45.
|
Lack of
supervision.
|
-
|
Sexual
drugs.
Expensive
drugs.
|
-
|
-
|
|
46.
|
-
|
-
|
Expensive
drugs.
|
-
|
-
|
|
47.
|
Lack of
awareness.
Low of QC.
Profits.
|
-
|
Expensive
drugs.
Chronic
disease medications.
|
-
|
-
|
|
48.
|
-
|
-
|
Expensive
drugs (cialis).
|
-
|
-
|
|
49.
|
Lack of
supervision.
Profits.
|
-
|
Diabetes.
HT.
|
-
|
-
|
|
50.
|
Profits.
|
-
|
-
|
-
|
-
|
|
51.
|
-
|
-
|
-
|
-
|
-
|
|
52.
|
Lack of
supervision.
High
benefits.
|
-
|
-
|
-
|
-
|
|
53.
|
High
prices of drugs.
|
More
supervision by the government.
|
Cosmetics.
Drugs for
weight loss.
|
-
|
-
|
|
54.
|
Law QC.
|
-
|
CNS drugs.
OTC drugs.
Cancer
drugs.
|
-
|
Closing
the pharmacy for longer time.
|
|
55.
|
High
prices of drugs.
|
To be more
serious in applying penalties.
|
Antiplatelet
(plavix).
HT,
antidepressants
|
-
|
-
|
|
56.
|
High prices.
|
-
|
NSAID.
HT.
|
-
|
-
|
|
57.
|
Lack of
coordination between control bodies.
Public
awareness.
High
prices of drugs.
Lack of
supervision.
|
-
|
Chronic
CVD.
Sexual
enhancers.
High sales
items (analgesics).
Anticancer.
Antibiotics.
|
3-5 years
prison.
100-5000
JD fine.
Penalty to
pay double the price of original packs.
Both
penalties in addition to 3rd penalty determined by court.
|
-
|
|
58.
|
High
prices of drugs.
|
Regular
raids and checking of pharmacies.
|
Cardiac
disease drugs.
|
Close
pharmacy.
Fine
payment.
|
Treating
drug counterfeiting as narcotics.
|
|
59.
|
Lack of
control.
High
prices of drugs.
|
-
|
HT.
Expensive
drugs.
|
Jail.
Payment of
fine.
Both.
|
-
|
|
60.
|
To make
money.
High
prices of drugs.
Lack of
supervision.
|
Increase
fine payment.
Withdraw
of licence.
|
HT,
diabetes.
Analgesics.
Expensive
drugs.
|
Prison.
Payment of
fine.
|
Increase
the period of prison and payment.
Withdraw
the licence.
|
|
61.
|
Lack of
inspection.
High
prices of drugs.
|
-
|
Antibiotics.
Analgesics.
NSAID.
Chronic
disease drugs.
|
Closure of
pharmacy.
Jail.
|
-
|
|
62.
|
Poor QC.
To make
money.
|
-
|
HT.
Expensive
drugs.
Sexual
enhancers.
Weight
reduction drugs.
|
Payment of
fine.
Jail.
Closing
the pharmacy.
|
-
|
Appendix
3
|
The open question
|
The most common answers among respondents
|
|
Factors that encourage drug counterfeiting.
|
1-
Lack of supervision and poor QC lab. Tests.
2-
Prices:
high prices of drugs and profits.
3-
Poor public awareness.
|
|
Suggestions to improve the situation.
|
1-
Improvement of regulations on borders,
increasing penalties and performance of QC lab tests.
2-
Increase public awareness.
3-
More international cooperation.
4-
Fighting favouritism.
|
|
Types of counterfeit drugs.
|
1-
Drugs used for chronic diseases.
2-
Fast moving drugs.
3-
Expensive drugs.
|
|
Ranges of penalties.
|
1-
Closure of the pharmacy.
2-
Jail.
3-
Payment of certain fine.
|
|
Suggestions to improve penalties.
|
1-
Increase fine penalties and the period of
prison.
2-
Withdrawing the pharmacists licence and not
allowing them to work in this field again.
3-
More commitment to implement the existing
penalties.
|