Abstract
Objective: To compare between
thoracoscopic debridement and/or decortication versus open decortication in the
management of thoracic empyema.
Methods: This retrospective study was conducted out at King Hussein
Medical Center,
during the period of December 2006 and November 2011.
Fifty-five patients with the diagnoses of stage two or three thoracic empyema were included in this
study. The patients were divided in two groups. Group A
included patients who underwent thoracoscopic debridement and/or decortication
and group B included patients who underwent open decortication. Efficacy of the
procedure, operative time, and postoperative blood loss, the need for
ventilator support, postoperative complications, postoperative hospital stay
and mortality were compared in both groups.
Results: Males constituted 61.8% (n=34)
of the studied patients. Twenty-nine patients (52.7%); underwent thoracoscopic
debridement and /or decortication while 26 patients (47.3%) underwent open
decortication. Mean age
(range) was 36.55±16.47 (16-70) years for group A, and 37.70±14.28 (17-67)
years for group B. There was no
statistical significant difference between both groups regarding postoperative
hospital stay (P=0.1012) and duration of air leak (P=0.1515). Duration of the
procedure was 209.29±20.93 minutes for group A patients, while it was
97.86±38.06 minutes for group B patients (P<0.001). Three out of the 26
patients (11.5%) who underwent open decortication died in the postoperative
period though the fatality was zero in group A patients.
Conclusion: Thoracoscopic debridement and/or decortication should be considered as the first surgical
option in the management of stage two and three thoracic empyema.
Key words: Empyema, Debridement,
Decortication, Thoracoscopy
JRMS September
2013; 20(3): 6-12 / DOI: 10.12816/0001034
Introduction
Pneumonia and parapneumonic effusion are still common causes of hospital
admissions.(1) Most parapneumonic effusions resolve with appropriate
antibiotic treatment with the resolution of the pulmonary infection. When bacteria invade the normally sterile pleural
cavity, empyema occurs.(2,3) According to the American
Thoracic Society, empyema thoracis is classified into three stages: The
exudative stage, the fibrinopurulent stage and the organized stage.(4)
Options of treatment change according to the phase of the disease, ranging from
antibiotic, thoracostomy tube drainage, to decortication.(5)
Open decortication, through open thoracotomy, is the conventional method
of surgical treatment of stage two and three thoracic empyema, which is
associated with significant post operative pain and morbidity.(6)
In the recent years, minimal invasive thoracic surgery has been accepted by
many thoracic surgeons as a safe and efficient alternative to open surgery in
the management of different thoracic diseases.(7) In this study,
we compared between thoracoscopic debridement and/or decortication versus open
decortication in the management of thoracic empyema at the Royal Medical
Services in Amman-Jordan.
Methods
This
retrospective study was conducted out during the period from December 2006
through November 2011 at the Thoracic Surgery Division, King Hussein Medical
Centre of the Royal Medical Services in Amman-Jordan. Approval from the Ethical
Committee was obtained to carry out the study. Data were retrieved from the Thoracic
Surgery Division computerized data base and from the patient’s files. The cases
that were subjected to minimal invasive decortication were performed when the
thoracoscopic instruments and an operating theatre with enough time is
available. But there was no selection according to the severity of the disease.
So this is just a retrospective collection of data. All the cases were operated
by two senior thoracic surgeons working as one team.
Fifty-five patients with stage two or three parapneumonic empyema were
included in this study. Exclusion criteria included: patients with stage one
disease, patients under the age of 14 years, and patients with empyema due to
other causes than pneumonia. The American Thoracic Society classification of empyema
was used to differentiate between the empyema stages. Stage 1- exudative phase,
stage - fibrinopurulent phase and stage 3-organised phase. Patients were
divided into two groups; those who underwent thoracoscopic debridement and/ or
decortication were named group A, while patients who underwent open
decortication were classified under group B. The patients were referred from
the pulmonology division of King Hussein Medical Centre and from different
peripheral hospitals of the Royal Medical Services. Diagnosis was based on the
clinical history and physical examination, chest X-Ray, pleural fluid analysis,
pleural fluid culture and chest CT scan. Fiberoptic bronchoscopy was done by
the pulmonologist prior to referral for decortication for all the cases. All
patients received intravenous antibiotics and thoracostomy tube drainage was
inserted as needed. The criteria for surgery were persistent septicaemia,
incomplete drainage of the pleural cavity and radiologic evidence of
multiloculated fluid and/ or entrapped lung. Routine Preoperative evaluation included a complete
history and physical examination, complete blood count with coagulation
profile, liver function and kidney function test, pulmonary function test and
arterial blood gases. Surgery was carried out under general endotracheal
anaesthesia using double lumen endotracheal tube for single lung ventilation. A radial arterial line, subclavian
catheter, and a Foleys catheter were inserted in all patients. The patients
were positioned in a complete lateral position according to the site with the
arm abducted on a special support.
Technique of open decortication:
A Standard Posterolateral thoracotomy incision was performed; layers
were opened in order without serratus anterior muscle splitting. Extra-pleural
dissection was carried out first to mobilize the whole lung en-block with the
pleura, the pleura is opened, then drainage of the empyema cavity and drainage
of any loculations till the whole lung is separate from the pleura, pleurectomy
done, then peeling of the entrapped lung is carried out to assure complete lung
expansion. Two chest tubes sizes 36 F were inserted then closure in layers.
Technique of Video-Assisted Thoracoscopic (VAT) decortication: Three
10mm incisions were used for the insertion of the trocars. The first trocar was
inserted at the 4th-5th intercostal space anterior
axillary line with blunt finger dissection technique then a 30 degree 10mm lens
is introduced through this port. Dissection is carried out using the lens
itself to separate the lung from the chest wall in a posterior direction
towards the tip of the scapula in order to create a clear and safe tract for
the insertion of the second port. The second trocar is inserted just below the
tip of the scapula. A 10mm suction tube is introduced through this trocar for evacuation of
loculations and
for mobilization of the lung in a direction towards the diaphragm. Then the
last trocar is inserted at the 8th intercostal space middle Axillary
line.
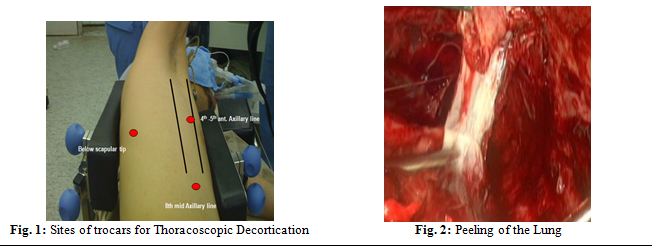
Sites of trocars
are shown in Fig. 1. Mobilization of the lung from the chest wall and
evacuation of any collection were carried out from the apex down to the
diaphragm. Then mobilization of the lung from the pericardium, mediastinum and
diaphragm is performed. After full mobilization of the lung, peeling of the
lung was done for stage 3 empyema (Fig. 2) and the fissures were opened. After
that, curettage of the parietal pleura is performed. The anesthesiologist then
inflates the lung and if it reaches the chest wall, the procedure is completed.
Two chest tubes size 36 F were inserted through anterior two port incisions and
the posterior incision was closed.
Post operative management: Post operatively the patients (in both
groups) were admitted either to the ward or to the Intensive care Unit
depending on the general condition of the patient. Prophylactic broad spectrum
antibiotics were given to all the patients till the time of chest tube removal.
Postoperative subcutaneous morphine was given for the first 48 hours regularly
for all the patients and if needed after that.
Intramuscular nonsteroidal anti-inflammatory drugs were used thereafter.
The chest bottles were connected to a continuous negative suction of - 20 cm water
till the air leak stopped. A test clamp for the chest tubes were done for 24
hours after the cessation of air leak, if the drained fluid is clear with a
production of less than 100 milliliter /24 hours with full lung expansion on
chest X-Ray. The chest tubes were removed thereafter if the follow-up chest
X-ray showed full lung expansion with no collection.
Demographic data,
co-morbidities, operative time, intraoperative details, postoperative
complications, postoperative blood loss, duration of air leak, post operative
hospital stay, and mortality were documented and analyzed. Due to the
retrospective nature of the study, Post operative pain was assessed by
comparing the amount of morphine needed in both groups after the first 48
hours. Follow up was done for
6 months after discharge. The student's
t test was used for statistical study. Continuous variables were expressed as
mean ± standard deviation, and categorical variables where expressed as
percentages. The level of confidence was defined as a P value of less than
0.05.
Results
Males
constituted 61.8% (n=34) of the studied patients. Twenty-nine patients (52.7%) underwent
Thoracoscopic debridement and /decortication, while 26 patients (47.3%)
underwent open decortication. Mean age (range) was
36.55+/-16.47 (16-70) years for the patients in group A, and 37.70+/-14.28
(17-67) for group B patients (Table I). Pleural fluid culture
results didn’t show any growth in 24 patients (43.6%) in both groups (Table II).
The stages of the empyema for both groups are shown in Table III (P= 0.8094). Right sided
surgery was carried out in 36 patients (65.5%) in both groups (Table IV).
Operative time was 209.29±20.93 (110-250) minutes for those who underwent
thoracoscopic decortication while it was 97.86±38.06 (70-150) minutes for group
B patients (P<0.001). Four out of the 29 patients (13.8%) who started by decortication
were admitted to the intensive care unit after the thoracoscopic procedure was
converted to the open technique. Twenty-one out of
the 26 patients (80.8%)
nderwent open procedure, and 11 of them (42.3%)
were kept on full ventilator support for less than 48 hours in the immediate postoperative period.Postoperative blood loss was less in group A (P <0.0001). The duration of air leak was more in group A patients (5.0±2.0 days, P=0.1515). Postoperative bleeding requiring blood transfusion and/or reopening, postoperative Atelectasis requiring fiberoptic bronchoscopy, wound infection and ventilator dependence were more in group B patients although no significant statistical difference were found. One out of the 29 patients who underwent thoracoscopic decortication developed postoperative atrial fibrillation that was managed medically. The total amount of morphine needed after the first 48 hours (as requested by the patients to control their pain) was 7.88±5.32 mg (0-25mg) in group A patients, while it was 13.85±7.25 mg (5-30 mg) in group B patients ( p=0.0014). Post operative hospital stay were 9.0±3.2 days for group A patients while it was 7.9± 4.5 days for group B patients (P=0.1012). Postoperative complications and events are shown in Table V.
Table
I: Demographics and preoperative characteristics
|
Variable
|
Group
A*
|
Group
B**
|
P
value
|
|
Number
|
29
(52.7%)
|
26
(47.2%)
|
|
|
Male/female
|
18/11
|
16/10
|
N.S
|
|
Age
|
36.55+/-16.47
|
37.70+/-14.28
|
N.S
|
|
Smokers
|
12
(21.8%)
|
11
(20.0%)
|
N.S
|
|
Diabetes mellitus
|
3
(5.6%)
|
4
(7.3%)
|
N.S
|
|
Hypertension
|
3
(5.6%)
|
4
(7.3%)
|
N.S
|
|
Chronic renal failure
|
0
(0%)
|
1
(1.8%)
|
N.S
|
|
Post liver resection
|
0
(0%)
|
1
(1.8%)
|
N.S
|
|
Ischemic heart disease
|
0
(0%)
|
2
(3.6%)
|
N.S
|
|
Epilepsy
|
1
(1.8%)
|
0
(0%)
|
N.S
|
*Thoracoscopic
decortication group *Open
decortication group N.S= not
significant
Table II: Culture results of
the aspirated pleural fluid
|
Culture result
|
Group
A*
|
Group
B**
|
P
value
|
|
No
growth
|
14(25.6%)
|
10(18.2%)
|
N.S
|
|
Mixed
growth
|
5(9.1%)
|
4(7.3%)
|
N.S
|
|
Staphylococcus
aureus
|
5(9.1%)
|
4(7.3%)
|
N.S
|
|
Streptococcus
pneumonia
|
2(3.6%)
|
1(1.8%)
|
N.S
|
|
Klebsiella species
|
2(3.6%)
|
1
(1.8%)
|
N.S
|
|
Pseudomonas species
|
1(1.8%)
|
4(7.3%)
|
N.S
|
|
Haemophilus species
|
0(0%)
|
2(3.6%)
|
N.S
|
*Thoracoscopic decortication
group **Open decortication group N.S= not significant
Table III: The stages of
parapneumonic empyema for the patients who underwent thoracoscopic and open
decortication
|
Group
|
Stage 1
|
Stage 2
|
Stage 3
|
Total
|
|
Group A*
|
0 (0%)
|
18 (32.7%)
|
11 (20.0%)
|
29(52.7%)
|
|
Group B**
|
0 (0%)
|
14 (25.5%)
|
12 (21.8%)
|
26 (47.3%)
|
|
Total
|
0 (0%)
|
32 (58.2%)
|
23 (41.8%)
|
55 (100%)
|
*Thoracoscopic
decortication group **Open
decortication group
Table
IV: Site of the performed surgery
|
Site
|
Group
A*
|
Group
B**
|
Total
|
|
Right
|
20
(36.4%)
|
16
(29.1%)
|
36
(65.5%)
|
|
Left
|
9
(16.3%)
|
10
(18.2%)
|
19
(34.5%)
|
|
Total
|
29
(52.7%)
|
26
(47.3%)
|
55
(100%)
|
*Thoracoscopic
decortication group **Open
decortication group
Table
V: Postoperative events and complications
|
Variable
|
Group
A*
|
Group
B**
|
P
value
|
|
Postoperative ICU
admission
|
6/29(20.7%)
|
21/26(80.8%)
|
0.0343
|
|
Ventilator support
< 48 hours
|
2/29(6.9%)
|
11/26(42.3%)
|
0.0452
|
|
Blood
loss (ml)
|
390±30.0
|
850±85.5
|
< 0.0001
|
|
Air
leak
|
5.0±2.0
(2-9
days)
|
4.0±2.0
(1-7
days)
|
0.1515
|
|
Bleeding/blood
transfusion
|
5/29(17.2%)
|
8/26(30.8%)
|
0.5134
|
|
Bleeding/
reopening
|
0/29(0%)
|
1/26(3.8%)
|
0.7586
|
|
Atelectasis
requiring bronchoscopy
|
1/29(3.8%)
|
2/26(7.7%)
|
0.7464
|
|
Ventilator
dependence
|
0/29(0%)
|
3/26(11.5%)
|
0.6938
|
|
Arrhythmias
|
1/29(3.8%)
|
0/26(0%)
|
0.8781
|
|
Wound
infection
|
0/29(0%)
|
1/26(3.8%)
|
0.7586
|
Three out of the 26
patients (11.5%) who underwent open decortication died in the postoperative
period due to adult respiratory distress syndrome though the fatality was zero
in group A patients. At three and six months follow up, all the patients in
both groups showed full lung expansion with no residual space or collection.
Discussion
The term empyema, according to medical dictionaries,
is a Greek word meaning in or within accumulation of pus.(8)
In general, treatment of empyema thoracis is achieved by draining the pus from
the pleural cavity to achieve full lung expansion and to treat the infection
with antimicrobial agents.(9) In the organized stage of
empyema thoracis, fibrin is deposited on pleural surfaces, forming a thick peel that restricts the underlying lung from
expansion. At this stage, the aim of treatment is to increase the lung
expansion by peeling the trapped lung (surgical removal of the thick peel). (10,11)
In the mid eighties and early nineties many reports had been published
discussing the use of Video-Assisted Thoracic Surgery (VATS) in the management
of early stages of empyema.(12,13) In the year 2001, Waller
and Rengarajan described the use of VATS successfully for the management of
stage three empyema thoracis.(14) In our study males constituted
most of the studied population, which is an agreement with many other authors, (5,7,14)
though, most of our patients were in the fourth decade of life, which
doesn’t match the results of other authors studies,(10-15)
which showed a 6th decade predominance, and this is attributed to
the fact that, as a military hospital, a lot of our insured patients are a
military personnel in a relatively young age groups. Although Tong et al.,
Waller et al. and Shahin et al.(7,14-15)
reported a shorter operative time in patients who underwent thoracoscopic
decortication as compared to the open method, in our study, there was a
statistical significant difference regarding the operative time in favor of the
open decortication group. Our explanation for this discrepancy in this result
is that it was our early experience in doing thoracoscopic decortication, in
addition we included stage 3 empyema in our study, in which, peeling of the
lung was mandatory, and this needed an extra time. Our rate of conversion from
Thoracoscopic procedure to open decortication was comparable to others such as Solaini et al. and Cardillo et al.(16,17) The postoperative
course showed marked advantages of thoracoscopic decortication over open
decortication, in which, postoperative pain was less in patients underwent the
thoracoscopic procedure (as confirmed by the amount of morphine needed), less
patients needed a postoperative intensive care unit admission and less patients
needed a ventilator support for the first 48 hours (with a statistical
significant difference). Also, the post operative blood loss was significantly
less in patients underwent thoracoscopic decortication. These results were
comparable to the results of many other authors. (7,9,12,15-18)
The need of blood transfusion postoperatively or reopening due to bleeding,
respiratory complications (mainly atelectasis requiring bronchoscopy),
ventilator dependence and wound infection were higher in patients underwent
open decortication (though not statistically significant), and these results
were an agreement with the results of Cardillo et al. and Melloni et
al. (17,18)
Shahin et al., Luh et al. and Bhatnagar et al.(15,19,20)
emphasized the value of thoracoscopic decortication in means of less air leak
post operatively and less hospital stay. In our study, the duration of air leak
and hospital stay was slightly higher in patients underwent thoracoscopic
decortication (although, not statistically significant). And this is attributed
to the fact that during our early experience, minor lung injury occurred during
peeling of the lung, and this caused more air leak and therefore more hospital
stay. One patient out of the 29 patients who underwent thoracoscopic decortication
developed slow atrial fibrillation in the first postoperative day, which was
managed medically, and this complication was attributed to mobilization of the
adherent lung from the pericardium during surgery. Although no mortality was
reported in the thoracoscopic decortication group, three fatalities occurred
among patients who underwent open decortication; and all fatalities were
attributed to Adult Respiratory Distress Syndrome after prolonged ventilator
dependence.
Limitation of the Study
1. The number of the studied sample is relatively small as compared to
other international studies.
2. No other local or regional studies were found discussing the same
subject to be compared with.
3. The retrospective nature of the study.
Conclusion
Both thoracoscopic and open decortication are efficient in the treatment
of stage two and three parapneumonic empyema. Thoracoscopic decortication
should be considered as the first surgical option in the management of these
stages as it results in less postoperative morbidity and mortality.
References
1.Restrepo M, Mortensen E, Rello J, et al. Late Admission to the
ICU in Patients With Community-Acquired Pneumonia Is Associated With Higher
Mortality. Chest 2010;
137: 552-557.
2.Mandal A, Thadepalli
H, Mandal A, et al. Outcome of Primary Empyema Thoracis:
Therapeutic and Microbiologic Aspects. Ann Thorac Surg 1998;
66:1782–1786.
3.Colice GL, Curtis A,
Deslauriers J, et al. Medical and surgical
treatment of parapneumonic effusions: an evidence-based guideline. Chest 2000;
118:1158 –1171.
4.Light R. Parapneumonic effusions
and Empyema. Proc Am Thorac Soc 2006; 3: 175-180.
5.Wurnig P, Wittmer V, Pridun N, et al. Video-Assisted
Thoracic Surgery for Pleural Empyema. Ann Thorac Surg 2006;81:309 –313.
6.Renner H, Gabor S, Pinter H, et al. Is aggressive surgery in pleural empyema
justified? Eur J Cardiothorac Surg 1998; 14: 117–122.
7.Tong B, Hanna J,
Toloza E, et al. Outcomes of
Video-Assisted Thoracoscopic Decortication. Ann Thorac Surg 2010; 89:220 –225.
8.Christopoulou-Aletra H, Papavramidou N. “Empyemas” of the
Thoracic Cavity in the Hippocratic Corpus. Ann Thorac Surg 2008; 85:1132–1134.
9. Molnar T. Current surgical
treatment of thoracic empyema in adults. Eur J Cardiothorac Surg 2007; 32 (3): 422-430.
10.Weissberg
D, Refaely Y. Pleural empyema: 24- year
experience. Ann Thorac Surg 1996;62:1026-1029.
11.Gokce M, Okur E, Baysungur V, et al. Lung decortication for chronic empyaema:
effects on pulmonary function and thoracic asymmetry in the late period. Eur
J Cardiothorac Surg 2009; 36(4): 754—758.
12.Hutter J, Harari D, Braimbridge M. the Management of Empyema Thoracis by Thoracoscopy and Irrigation. Ann
Thorac Surg 1985;39:517-520
13.Ridley P, Braimbridge M. Thoracoscopic debridement and pleural irrigation in the management of empyema thoracis. Ann
Thorac Surg 1991 ;51(3):461-464.
14.Waller D, Rengarajan A. Thoracoscopic decortication: a role for video-assisted surgery in chronic postpneumonic pleural empyema. Ann Thorac Surg 2001; 71(6):1813-1816.
15.Shahin Y, Duffy J,
Beggs D, et al. Surgical management of primary empyema of the
pleural cavity: outcome of 81 patients. Interact CardioVasc Thorac Surg
2010; 10 (4): 565-567.
16.Solaini L, Prusciano F, Bagioni P. Video-assisted thoracic
surgery in the treatment of pleural empyema. Surg Endosc 2007;
21:280–284.
17.Cardillo G, Carleo F, Carbone L, et al. Chronic postpneumonic
pleural empyema: comparative merits of thoracoscopic versus open decortication.
Eur J Cardiothorac Surg 2009; 36:914–918.
18.Melloni G, Carretta
A, Ciriaco P, et al. Decortication for
chronic parapneumonic empyema: results of a prospective study. World J Surg
2004; 28:488–493.
19.Luh SP, Chou MC,
Wang LS, et al. Video-assisted thoracoscopic surgery in the
treatment of complicated parapneumonic effusions or empyemas: outcome of 234
patients. Chest 2005; 127:1427–1432.
20.Bhatnagar R, Maskell NA. Treatment of complicated pleural effusions in 2013. Clin Chest Med 2013; 34: 47-62.