Abstract
Objective: To review the spectrum of metallic foreign
bodies among Jordanian soldiers and the efficacy of treatment.
Methods: A retrospective review was
conducted at Prince
Rashid Bin
Al-Hassan Hospital
between August 2011 and March 2012. File and photographs review of 55 patients who attended the ophthalmology
clinic and found to have corneal metallic foreign body were included in this
study. The following data were
extracted and analyzed: age, gender, past ocular history, mechanism and time of
injury and whether any eye protective measures were taken for those who were exposed
to trauma during work, time to receive treatment, method of corneal foreign
body removal, number of foreign bodies, location, depth of foreign body in the
cornea, whether the eye was patched or not after removal of corneal foreign
body, associated ocular injury, presence of Bell’s phenomenon, complications,
and duration of absence from work.
Results: All patients were
males and the age ranged between 17 and 55 years (mean 31.3 years). Eighty- two percent of eye trauma occurred
during work and all of them did not use any protective measure during their
work activity. The mid third of the cornea was involved in 39% of patients
followed by the paracentral zone in 27%. Corneal foreign bodies were removed by
27 gauge needle in 68% of patients. Eye patch was not used in 48% of patients
after removal of foreign body. The most common associated finding was corneal
rust in 63% of cases. Absence from work ranged between two to nine days.
Conclusion: Corneal foreign
bodies are potentially sight threatening that occurs mostly as a result of
occupational accidents in male workers who do not comply with the use of eye
protection. Educational and safety programs and patient counselling on proper eye protection are
essential and must be implemented in the work places to prevent serious eye injuries
and work loss.
Key words: Cornea, Metallic,
Foreign body, Jordanian patients.
JRMS September
2013; 20(3): 21-26 / DOI: 10.12816/0001036
Introduction
Corneal foreign body (FB) is
usually a preventable work- related cause of visual morbidity and blindness in
developing countries.(1) It is one of the important causes of
attendance at the ophthalmic emergency clinic in the military hospitals of Jordan.
Once it is diagnosed it should be
removed immediately to prevent the adverse impacts on the cornea that may be
sight threatening as a result of corneal scarring, infectious keratitis and endophthalmitis.(2)
These adverse impacts may lead to loss of productive power as well as social
and medical costs.(3) Most of the corneal foreign bodies are
metallic in nature and occur during work at industrial facilities or constructionworkshops.(4) The metallic FB may be adherent
superficially to cornea or embedded in the corneal layers and if not removed,
rust ring may develop within hours that may cause permanent staining and
scaring of the cornea.(5-7) Management of corneal FB injuries includes
detailed history about the mechanism of trauma and thorough examination of the
eye to rule out eye penetrating eye injury. Removal of the FB is attempted
initially, if it is located superficially on the cornea, by using a
cotton-tipped swab soaked in saline after instilling topical anesthesia, if
this fails or if the FB is embedded deeply in the cornea it can be removed by
using 27 gauge needle followed by antibiotic eye ointment, as a soothing agent
and prophylaxis, with or without eye patching.(8,9) The aim of this study was to review the
spectrum of metallic foreign bodies among Jordanian soldiers and the efficacy
of treatment.
Method
A retrospective review was conducted
at Prince Rashid Bin Al-Hassan Military
Hospital between August
2011 and March 2012. File and
photographs review of 55 patients who attended the ophthalmology clinic and found to
have corneal metallic foreign body were included in this study. The following data were extracted and
analyzed: age, gender, past ocular history, mechanism and time of injury
and whether any eye protective measures were taken for those who were exposed
to trauma during work, time to receive treatment, method of corneal foreign
body removal, number of foreign bodies, location, depth of foreign body in the
cornea, whether the eye was patched or not after removal of corneal foreign
body, associated ocular injury, presence of Bell’s phenomenon, complications,
duration of sick leave. Exclusion criteria included patients with corneal non -
metallic FB, penetrating eye injuries, rust ring without FB, patients who were
treated in other hospitals and came for regular follow up at Prince Rashid Bin
Al Hassan Military Hospital, and patients with incomplete information records. The local ethical committee of the Royal
Medical Services approved the study.
Results
All patients were males and
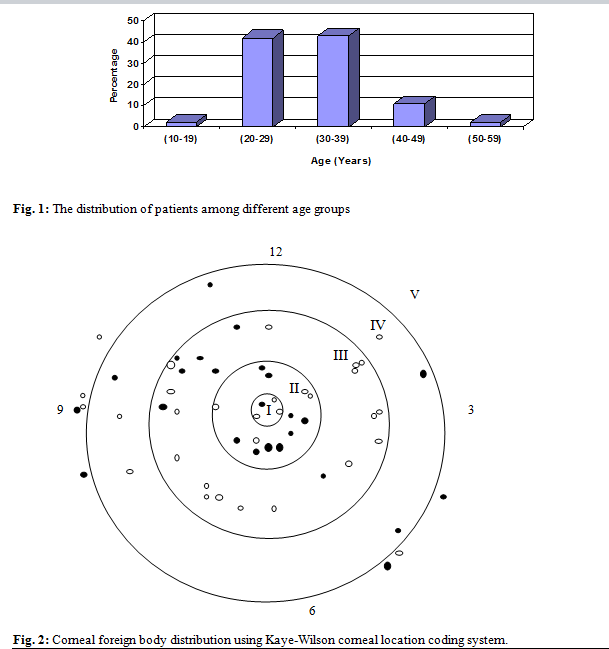
the age ranged between 17 and 55 years (mean 31.3 years). Figure 1 summarizes
the distribution of patients among different age groups. One patient had
multiple FBs on the same cornea and one had bilateral FBs while the remaining
patients had only one FB (Fig. 2).
The time from the onset of FB
symptoms to attendance to the eye emergency clinic ranged between three hours
and four days; 30.9% of patients attended within few hours, 52.7% in the first
day and the remaining patients attended between second and fourth day. Table I
shows the presenting symptoms. Table II shows the place where the trauma occurred. Table III
demonstrates the causes of trauma. All patients who had trauma at work sites did
not use any protective measure during their work activity.
The best corrected visual acuity
ranged from 6/6 to 6/12 and after one week of treatment it improved to normal
in all patients.
Kaye - Wilson corneal location
coding system(10) was used for the distribution of FBs on the
cornea among the patients, where zone I represents the central part of the
cornea, zone II represents the paracentral third of the cornea, zone III
represents the mid third of the cornea, zone IV represents the peripheral third
of the cornea, zone V represents the limbal area, the black filled circles
represent the right eyes foreign bodies and the black empty circles represent
the foreign bodies in the left eyes (Fig. 2).
In both eyes the commonest
site for corneal foreign bodies was in zone III (39%) followed by zone II
(27%), zone IV (14%), zone V (13%) and zone I (7%). If we draw an imaginary
line between two and 10 o’clock and another line between four and eight o’clock,
the cornea will be divided into three parts; zone A above the 1st line, zone B
between the two lines (inter-palpebral fissure) and zone C below the two line.
The foreign bodies were
located in zone B in 63% of cases, zone C in 23%, and zone A in 14%. Most of
the embedded corneal FBs extended from the epithelial layer to the anterior
stromal layer (60%), and the remaining 40% were located within the epithelial
layer of the cornea. The associated findings are summarized in Table IV.
Corneal infiltrates were noticed in 30% of patients and all of them had
associated rust ring on the cornea. Rust ring was present in 63% of patients. Bell's
phenomenon was negative in six (11%) patients, three of them the foreign body
was located in zone III, two in zone II and one in zone IV. And if we use the
horizontal planes for distribution of foreign bodies; three of them were in
zone A and two in zone C. Corneal foreign bodies were removed by cotton swabs
in 32% of patients while the remaining foreign bodies were removed by 27 gauge
needle. Eye patch was used in 52% of patients after removal of the FB and
remaining 48% were left unpadded.
Table I: The presenting
symptoms
|
Presenting symptom
|
%
|
|
Pain
|
100
|
|
Lacrimation
|
43.6
|
|
Redness
|
56.4
|
Table II: The place where the trauma occurred
|
Place Where The Trauma Occurred
|
Constructive Workshops
|
Walking Activity
|
Patients Did Not Report Or Remember How They Got the Eye Trauma
|
|
Percentage
|
82
|
9
|
9
|
Table III: The causes of trauma
|
Cause of Trauma
|
Grinding
|
Drilling
|
Welding
|
Nailing
|
|
Percentage
|
51
|
21.9
|
18.2
|
9.1
|
Table IV: The associated
corneal findings
|
%
|
Associated
finding
|
|
27
|
None
|
|
4
|
Old corneal scar from old
foreign body
|
|
9
|
Corneal abscess
|
|
30
|
Corneal infiltrates
|
|
63
|
Rusting
|
Table V: Shows the relationship between the locations of the
corneal foreign bodies within the corneal layers, duration of healing with and
without eye patch use and of sick leaves
|
FB location within the corneal layers
|
Number
(Percentage)
|
Healing period
(days)
|
Sick Leave Duration
(days)
|
|
Eye Patch Use
|
No Eye Patch Use
|
|
Epithelial
|
22 (40)
|
22 (40)
|
2
|
2
|
2
|
|
Epithelial and anterior stromal
|
33 (60)
|
12 (22)
|
2
|
2
|
2-4
|
|
17 (31)
|
3- 7
|
3- 7
|
4- 8
|
|
4 (7)
|
8- 9
|
8- 9
|
9
|
|
Total
|
55 (100)
|
55 (100)
|
|
|
None of the patients who did
not use eye patch had significant eye pain after removal of FBs and the healing
rate was the same as those who did not use eye patch, Table V. Patients were given sick leave and followed up
after two days. The duration of treatment ranged from two to nine days (mean 3
days). After removal of the foreign body, complete healing of corneal erosion
was noticed in 62% of patients in two days, 93% in seven days, and 100% in nine
days. The absence from work ranged from two to nine days with an average of
four days (Table V).
Discussion
Corneal FB injury is
responsible for about 26% of the worldwide 55 million eye injuries that occur
annually.(11) It is usually a preventable work- related
cause of visual morbidity and males are usually more affected than females. In
our study all affected patients were males who did not use protective eyewear
and their age ranges between 20 and 40 years in more than 80% of cases (Fig. 1),
and the majority occurred during work.
This is because most of the people who work in military workshops are
males and belong to this age group while females usually work in medical and
administrative fields. These findings agree with other previous studies,
which reported that males are affected in more than 90%
of the cases between the third and fourth decades of life and most of them
occurred during work.(2,10) Smith et al.(12) hypothesized that differences in protective eyewear
use between men and women may contribute to differences in eye injury rates. Eighty-two percent of eye trauma occurred at
industrial facilities or constructive workshops during grinding, drilling,
welding or nailing. Ninety percent of them did not use any protective measure
during their work activity, and the remaining 10% did not use proper glasses
with side shields. The presenting symptom was pain in the majority of patients
and 83% of them attended the clinic within two days from the onset of pain.
This can be explained by the location of the FB on and within the cornea. Two thirds of the FBs were located in zone II
and III, which have higher density of sensory nerve fiber endings than zones IV
and V, and 61% were embedded deep in the cornea and reaching the anterior
stromal layer where nerve endings located and these will cause more pain
sensation. Although the commonest site for corneal foreign bodies was zone III
(39%), the central and para-central zones (I and II) represented 41% of cases,
which means that vision was threatened in these cases. Regarding foreign bodies
distribution in the horizontal planes 63% of the foreign bodies were located in
zone B, 23% in zone C and 14% in zone A, this means that in most of the cases
foreign bodies were located within the palpebral fissure area and this reflects
the major protective role of the eyelids. We found that there was a
proportional relationship between the depth of the FBs within the cornea and
the duration of sick leave. The deeper the FB embedded in the cornea the longer
the duration of absence from work as these cases need longer time to heal after
the removal of the corneal foreign body and there is a higher possibility of
corneal scarring that may interfere with vision. All patients with epithelial
layer FBs healed within 2 days, in comparison with 22% of patients with
epithelial and anterior stromal FBs. About 7% of patients with epithelial and
anterior stromal FBs had a sick leave for 9 days due to delayed healing after
removal of the FBs and scar formation.
The most common associated
finding was rust ring which was found in about two thirds of cases, this was
not surprising because rust ring usually develops within few hours as a result
of oxidation of ferrous containing foreign bodies.(5,6,8) It
is recommended to remove rust from the cornea as early as possible to prevent
tissue permanent staining, necrosis, and scarring.(13) Rust
ring can be removed with chelating agent, desferrioxamine, eye ointment but this
method proved to be less effective than surgical removal.(5)
Another method is the use of electric drill which is very effective,(6)
but, unfortunately, it is not available in our hospital, so removal by 27 gauge
needle remains the treatment of choice. Corneal abscess was found in 9% of
patients and it was treated aggressively to prevent permanent corneal opacity
or endophthalmitis.(2) Bell's
phenomenon was negative in 6 patients and the most common site of corneal
foreign bodies was in zone III (50%) followed by II (33%) and IV (17%). This
distribution was very similar to that found in Bell's positive patients. When horizontal
planes distribution was studied the commonest site for foreign bodies in Bell's
negative patients was in zone A (50%) followed by zone C (33%) and zone B
(17%), while in Bell's positive patients, 63% foreign bodies were found in zone
B, 23% in zone C and 14% in zone A, this emphasizes the importance of Bell's
phenomenon in protecting the cornea. Eye patch was not used in almost half of
the patients and there was no difference in rate of corneal erosion healing or
decrease of pain after removal of the foreign bodies between this group and the
group of patients who used eye patch, Table V. On the contrary patients who did
not use eye patch were more satisfied as they had better binocular vision.(9)
A meta-analysis of seven studies
was done by Turner and Rabiu,(14) by searching the Cochrane
Central Register of Controlled Trials and they concluded that treating simple
corneal abrasions with a patch does not reduce pain, it results in a loss of
binocular vision, and they discourage the use of eye patch for simple corneal
abrasions. Complete healing was noticed in 62% of patients after two days of
complete surgical
removal of corneal foreign
bodies while 36% of patients were still complaining of pain; two thirds of them
was due to incomplete healing of the corneal erosion and one third was mostly
due to incomplete removal of the rust and to a lesser extent due to the
presence of corneal abscess. At the end of treatment, 82% of patients were
treated successfully without any residue on the cornea while 18% of patients
had faint corneal opacity that did not interfere with best corrected visual
acuity. Efficient prevention can prevent
irreversible damage to the eye, loss of wages and work, and it saves the cost
of the health care to be presented to those injuries. In our study the absence
from work ranged from two to nine days. Fong et al.(13)
in his survey of all eye injuries in Australia, found that the use of
safety eyewear resulted in annual cost savings of $59 million.
Conclusion
This study showed that corneal
metallic foreign bodies are potentially sight threatening that occurs mostly as
a result of occupational accidents in male workers who do not comply with the
use of eye protection. Educational and safety programs and patient counselling on proper eye protection are
essential and must be implemented in the work places to prevent serious eye injuries
and work loss. Further studies are needed to find out why workers do not comply
with safety measures to protect the eyes in work.
References
1.Oluyemi F. Epidemiology of penetrating eye injury in Ibadan: a 10-year hospital-based review. Middle East Afr J Ophthalmol 2011; 18(2):159-163.
2.Macedo Filho ET, Lago A, Duarte K, et al. Superficial corneal foreign body: laboratory and epidemiologic aspects. Arq Bras Oftalmol 2005; 68(6):821-823.
3.Alexander MM, MacLeod JD, Hall NF, Elkington AR. More than meets the eye: a study of the time lost from work by patients who incurred injuries from corneal foreign bodies. Br J Ophthalmol 1991; 75(12):740-742.
4.Jafari AK, Bozorgui S, Shahverdi N, et al. Different causes of referral to ophthalmology emergency room. J Emerg Trauma Shock 2012; 5(1):16-22.
5.McGuinness R, Knight-Jones D. Iron-containing corneal rust rings treated with desferrioxamine. Br J Ophthalmol 1968; 52(10):777-780.
6.Liston RL, Olson RJ, Mamalis N. A comparison of rust-ring removal methods in a rabbit model: small-gauge hypodermic needle versus electric drill. Ann Ophthalmol 1991; 23(1):24-27.
7.Peate WF. Work-related eye injuries and illnesses. Am Fam Physician 2007; 75(7):1017-1022.
8.Newell SW. Management of corneal foreign bodies. Am Fam Physician 1985; 31(2):149-156.
9.Kaiser PK. A comparison of pressure patching versus no patching for corneal abrasions due to trauma or foreign body removal. Corneal Abrasion Patching Study Group. Ophthalmology 1995; 102(12):1936-1942.
10.Kay-Wilson LG. Localisation of corneal foreign bodies. Br J Ophthalmol 1992; 76(12):741-742.
11.Jones NP, Hayward JM, Shaw PT, et al. Function of an ophthalmic 'accident and emergency' department: results of a six-month survey. BMJ 1986; 292:189-191.
12.Smith GS, Lincoln AE, Wong TY, et al. Does occupation explain gender and other differences in work-related eye injury hospitalization rates? J Occup Environ Med 2005; 47(6):640-648.
13.Fong LP, Taouk Y. The role of eye protection in work-related eye injuries. Aust N Z J Ophthalmol 1995; 23(2):101-106.
14.Turner A, Rabiu M. Patching for corneal abrasion. Cochrane Database Syst Rev 2006; (2):CD004764.