Introduction
A benign tumor or neoplasm is a non-cancerous
(non-malignant) abnormal mass of tissue that forms when cells in a localized area
reproduce at an increased rate. Peri-ocular area is a common site for benign and
malignant lesions in all age groups.(1) Peri-ocular structures
that include the eyelids, eyebrows, lacrimal sac, conjunctiva, and cornea
epithelium are derived from the surface ectoderm and congenital anomalies can
present as tumor or tumor-like lesion at birth or soon after birth. For
example, choristomas, which are normal tissues in abnormal location, such as
dermoid are usually found at birth,(2) while capillary
hemangiomas, which are hamartomas i.e. benign tumor-like growth with abnormal,
localized proliferation of vascular endothelial cells, usually appear soon
after birth.(3) Other tumors appear during adolescence such
as conjunctival nevi that are usually amelanotic during childhood and present
cosmetic and sometimes functional problems when they start to grow and gain
melanin pigments during adolescence. These tumors are benign and it is
extremely rare to undergo malignant transformation at an early age, (4)
although they might become inflamed thus urging excision to rule out
malignant transformation.(5) The primary malignant lesions are usually due
to prolonged sun exposure(6) and seen more frequently in
elderly patients(7) or patients with chromosomal
abnormalities that lead to formation of skin cancers such as Gorlin- Goltz
syndrome.(8) However; metastasis
from distant sites or invasion from adjacent structures may occur.(1)
In clinical practice,
eye tumors and tumor-like lesions can be classified into extra- and intra-ocular.(9)
In this study, only extra- ocular tumors that are located outside the eye
were investigated. In most of the cases the clinical diagnosis is obvious and
does not need histopathological investigations such as, chalazion, pterygium
and nevus unless there are suspicious signs of malignancy.(1,4-5)
For example, recurrent chalazion after excision in an elderly patient, abnormal
vessels, bleeding, or elevated mass from a pterygium or a nevus, all
necessitate a diagnostic biopsy.(10)
Prince Rashid Bin
Al-Hassan is a general district hospital with a bed capacity of about 300 beds.
The ophthalmology clinics cover all aspects of ophthalmology including
oculoplastic and pediatric specialities. Benign lesions and malignant tumors that
do not need major reconstruction after excision are usually treated locally without
referral to King Hussein Medical
Center. After tumor
excision, all specimens, even if the diagnosis is obvious clinically, are sent
to pathology laboratory for histopathological examination fixed in 10% buffered
formalin solution where it takes two weeks to collect the results. Review of literature revealed some data available
from Jordan Cancer Registry about the eye malignant lesions in Jordan
but not peri-ocular malignant lesions.(11)
The aim of this
study was to analyze the histologically proven peri-ocular tumors at Prince
Rashid Bin Al- Hassan military hospital in the North of Jordan.
Methods
This was a
hospital-based, non-comparative, retrospective study, conducted at Prince
Rashid Bin Al-Hassan military hospital in the North of Jordan over a period of
4 years between January 2008 and January 2012. Medical records of patients who
underwent excisional biopsy of a tumor or tumor-like lesion, or incisional
biopsy when complete resection was impossible and proven by histopathology
during that period, were reviewed and included in the study.
Exclusion
criteria include patients who were not Jordanian, patients with intra-ocular
tumor, eviscerated or enucleated globe, and patients with incomplete medical
records. Descriptive statistics like mean, average, frequency, and percentages
were used.
The ethical
committee of the Royal Medical Services approved the study.
Results
A total of 105 medical records were reviewed. There
were 58 males (55.2%) and 47 females (44.8%) with a male to female ratio of
1.2: 1. The distribution of the lesions with regards to gender and age are
shown in Table I with the age group of 11 - 20 years being most frequently
affected. The median age of the patients was 27 years with a range of 10 months
to 94 years. Histopathological examination revealed that 87 (82.9%) cases were
benign, six (5.7%) premalignant, and 12 (11.4%) malignant. The eyelids were the
most common site for the lesions and accounted for more than half of the cases.
Table II demonstrates the distribution
of the tumors and tumor-like lesions in the peri-ocular structures and its
malignant potential and it shows that the eyelid was the commonest site for benign, premalignant, and malignant tumors and cornea was the least site for benign lesions. Table III summarizes the histological results of the lesions and their distribution in the peri-ocular area. Of the benign lesions the most frequent was nevus and the most common malignant tumor was basal cell carcinoma (BCC), however the least common benign tumors were lacrimal gland pleomorphic adenoma, nonspecific inflammation and benign lymphocytic hyperplasia, and sebaceous hyperplasia, and the least common malignant tumors were eyelid sebaceous gland carcinoma and conjunctival malignant melanoma.
Discussion
Jordan cancer registry (JCR) showed that eye cancer
incidence in Jordan
in 2009 was 0.3%, with females being slightly more affected than males. The
incidence of cancer in the governorate of Irbid was 13.2%, but the incidence of
eye cancer in this governorate was not determined.(11) None
of the eye cancers occupied the top ten cancers in Jordan though, and the peri-ocular
tumors are under diagnosed in Jordan.(11)
In comparison
with JCR,(11) our cohort showed that males were affected more
frequently than females and this can be explained by the following: first, this
study included benign and malignant tumors, and tumor-like lesions, second,
intra-ocular tumors were excluded, and third, some of these tumors are related
to prolonged exposure to sunlight(6) which is more frequent
in male military personnel.
In contrast to
Reddy et al.(9) who found males in
the first decade to be more frequently affected, the commonest age group to be
affected in our study was 11-20 years with female preponderance (24.8%) probably
related to the cosmetic worries of female patients and their parents,
especially at this age. This is followed by those below the age of 10 years
where peri-ocular congenital anomalies and acquired lesions might lead to
amblyopia due to visual obscuration or astigmatism and parents' anxiety and
these findings are comparable with previous studies presented in literature.(12)
In general, the main indication for excision was cosmetic below the age of 40
years and suspicion of malignancy after that age. In our study, none of the
malignant lesions were discovered in the younger age groups. These cases are
usually referred to King
Hussein Medical
Center where they can
receive further more complicated management after excision in collaboration
with other specialties.
Malignant lesions
formed 11.4% of the lesions with basal cell carcinoma affecting the eyelids
(83%) being the commonest tumor which is slightly less than previously reported
studies.(1) Malignant tumors affecting the conjunctiva were
encountered in 16.7% and the conjunctiva was the commonest site to encompass
benign lesion such as nevus and this was comparable to Amoli et al.(13)
study but different from Luiz et al.(14) study who
found conjunctival intraepithelial neoplasia to be the most frequent lesion. The
chronic exposure to sunlight was blamed to be the main risk factor for
peri-ocular malignant lesion and the risk is usually decreased by protective
measures such as using sunglasses and sunscreen(15) and this may
explain why two thirds of malignant lesions in
men (8/12) who usually had more outdoor activities.(6)
Sebaceous gland carcinoma of the eyelid is a very rare
tumor that frequently involves the upper eyelid. It originates from either the
meibomian glands or glands of Zeis. The upper eyelid contains more meibomian
glands than the lower eyelid which explains the higher frequency of the upper
eyelid involvement.(7,16-17) It is more common in middle aged
women.(16) Sebaceous gland carcinoma may spread
intraepithelially to invade the conjunctiva and the cornea (pagetoid spread).(17)
Conjunctival malignant melanoma is a rare tumor that accounts for 2% of all
ocular malignancies, that is frequently seen in elderly patients.(4,13-16,18,19)
It is treated by excision and cryotherapy or Mitomycin.(18-19)
If orbital recurrence occurs then exenteration is an option if cannot be
controlled with other methods, although it does not improve the survival rate.(19)
Our case was 73- year old male patients with recurrent conjunctival malignant
melanoma and orbital invasion with no metastasis (Fig. 3). Peri-ocular malignant tumors need long-term
follow to rule out early recurrence or new primary tumors. A study conducted in
UK showed the recurrence rate after complete excision of BCC tumors with five
years follow up to be 0.26%.(20)
Premalignant tumors were seen in 5.7% of patients.
Recently some premalignant lesions, such as kerato-acanthoma, were considered
histologically as a low grade malignancy.(13,21) Conjunctiva
and corneal intra-epithelial neoplasia is an uncommon conjunctival and/or
corneal disease that has a low malignant potential.(13)
Characterized by mild to severe epithelial dysplasia with dysplastic cells
(carcinoma in situ).(18) These tumors are usually seen in
patients above the age of 50 years who had outdoor activity, history of human
papilloma virus, and patients with low immunity disorders.(22) Our
four patients were between 30 and 50 years and all of them were males, treated
with surgical excision with or without cryotherapy. Solar keratosis is by far
the most common benign tumor of the eyelids that usually seen in fair- skin
elderly patients with excessive exposure to ultraviolet light and the immune
system is important in its development and pathogenesis.(1,23)
Histologically characterized by focal to confluent parakeratosis overlying an
epidermis and atypia in the keratinocytes. Treatment of kerato-acantoma of the
eyelid is with excision because spontaneous involution may lead to an ugly
residual scar. (1, 21)
Benign lesions were encountered in about 83% of the
tumors and tumor- like lesions and 45% of them were found in the eyelids and followed
by the conjunctiva (27.6%). The frequency was slightly higher than Reddy et
al.(9) but lower than Sanjay et al.(24)
studies. This might be due to inclusion of extra-ocular tumors only. All these
lesions were seen in young patient below the age of 40 years. On contrary to previous studies where dermoid
cyst was the most frequent benign tumor,(9,24) in our study
the most frequently encountered benign growth was the nevus (22/87) (Table III),
eight nevi were seen in the eyelids and 14 in the conjunctiva. All conjunctival
nevi were compound type while eyelid nevi, five of them were compound, two
intradermal and one junctional. Most of the conjunctival nevi were encountered
in the second and third decade of life and the main indication for excision was
cosmetic and this was less than that encountered in Saudi population with
regard to age and indication.(25) The conjunctival nevus is
usually melanotic, amelanotic (30%), or mixed with various shapes and sizes. It
usually contains micro-cysts that can easily be seen with slitlamp
biomicroscopy, (Fig. 4) malignant transformation is usually seen in less than
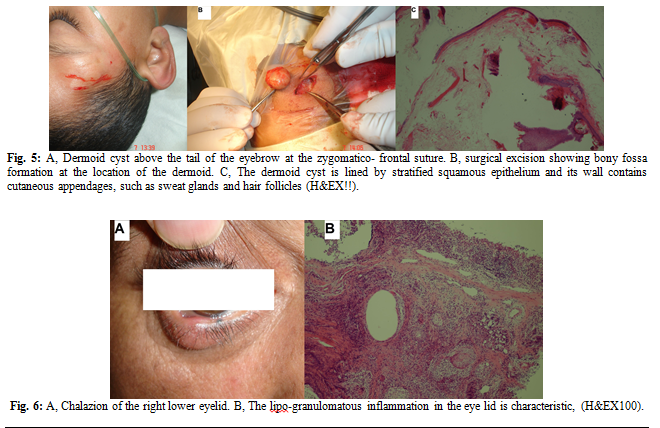
1% of conjunctival nevi.(4) Dermoid cyst, which is a
choristoma,(2) was encountered in 13 (12.4%) cases; the
majority (8/13) was seen in the eyelids (above the lateral canthus at the
zygomatico-frontal suture, (Fig. 5), and above the medial canthus at the
fronto-ethmoidal suture), three cases above the tail of the eyebrow, and two
cases epibulbar. In the other similar studies dermoid cysts were the commonest
tumors and of all them were located above the outer canthus.(9,24)
These lesion were found in pediatric age group and presented since birth. All
peri-ocular demoid cysts were completely excised and found to be lined with
stratified squamous epithelium containing cutaneous appendages. Ruptured
dermoid cyst may lead to severe inflammation that may mimic rhabdomyosacroma at
pediatric age group,(2) that is why we always try to excise
the tumor before the child starts to walk that might lead to rupture of the
dermoid cyst if the child falls down or receive a trauma to the cyst. Ten
patients between 30 and 50 years had peri-ocular sebaceous cysts. All were
completely excised and most of them were found in the medial canthal area.
These lesions are very common and usually result from minor trauma or surgery
and contain pasty contents.(1) The cyst is lined by
keratinized squamous epithelium and filled with keratin material. Pilomatrixoma
is a benign tumor of the hair follicle that is usually seen in the young age
group with the upper eyelid and eyebrow as favorable sites.(26)
Seborrheic keratosis was diagnosed in four elderly
patients and this was almost the same as Sanjay et al.(24)
They are light to dark, well demarcated plaques, with granular cobblestone
surface. Histologically, proliferation of bland epidermal cell and formation of
horn cysts are seen. There are few variants of these lesions and the treatment
is usually with curettage.(1) Conjunctival retention cyst,
which is a cystic dilatation of a mucin gland secondary to obstruction of its
duct,(14) was present in 4(3.8%) patients and this was less
than Reddy et al (5.6%) findings;(9) one of them was in the
vicinity of a pterygium. Pyogenic granuloma contains endothelial proliferation
of blood vessels with associated stromal eosinophilic infiltrates, ulceration
and granulation. While Reddy et al.(9) cases were seen after chalazion and pterygium
excision our cases were associated with chalazion in patients below the age of
30 years, two in the eyelids and two in the conjunctiva.
Capillary hemangioma is a hamartoma, a benign tumor-
like growth lesion, which is usually congenital or appears after birth as in
our three cases. The early lesions are lobulated masses of small tight
capillaries with plump endothelial lining cells.(3) These
lesions should be allowed to regress unless there is a risk of amblyopia then
surgical excision can be done if tumor is small and localized.(12)
Nowadays treatment with beta blockers is a promising modality and should be
tried as long as there are no contraindications.(3,27)
A
chalazion is a localized, chronic, sterile, lipo-granulomatous inflammatory
lesion of sebaceous (meibomian) gland secondary to its duct blockage.(10)
Diagnosis of chalazion is obvious clinically in young patients but
recurrent or suspicious chalazion in elderly patients should be biopsied to
rule out sebaceous gland carcinoma. In our study three chalazia in elderly female
patients (all above the age of 65 years) were biopsied and proved
histologically to be none malignant (Fig. 6).
Apocrine hydrocystomas are benign cystic lesions that
are seen along the eyelid margin with white precipitates at the bottom
secondary to blockage of glands of Moll ducts.(1) They were
seen in three middle aged women and in contrast to Sanjay et al.(24)
study none of them were eccrine hydrocystoma. Lacrimal gland pleomorphic
adenoma is the most common benign tumor of the lacrimal gland that needs
complete surgical resection to decrease the risk of malignant transformation or
recurrence after incisional biopsy.(28) It was encountered in
a 16- year female patient.
Limitations of the Study
Our study suffers from few limitations. First, not all
histopathologic reports of patients with peri-ocular tumor could be found in
the medical files. Second, this was a
hospital-based review and it does not represent the true prevalence of
peri-ocular tumor in the North of Jordan, so there should be a cooperation
between all the hospitals in the North of Jordan (governmental, military,
university, and private sector) to detect the true incidence and prevalence. Third,
because this hospital is a general district hospital so advanced malignant
tumors were not involved, and finally, only extra-ocular tumor was included, so
our data cannot be compared with the JCR and other studies accurately.
Conclusion
Peri-ocular tumors appear to be frequent but the true
prevalence in the North of Jordan cannot be determined by this study. Male to
female ratio of peri-ocular tumors was different from that reported in
literature. The frequency of malignant and pre-malignant tumor lesions was
17.1% and this percentage should be taken seriously. Any suspicious lesion
should be biopsied particularly in elderly patients, after the fifth decade of
life.
References
1.Bernardini FP. Management of malignant and benign eyelid lesions. Curr Opin Ophthalmol 2006; 17(5):480-484.
2.Moin M, Ihtesham UD, Nazeer A. Ocular and periocular dermoid cysts; a clinico-pathological study. Biomedica 2005; 21: 113-116.
3.Peralta RJ, Glavas IP. Ophthalmic Pearls: Pediatrics. Review of Capillary Hemangioma. Eye Net Magazine. 2009. Online publication: http://www.aao.org/publications/eyenet/200902/pearls.cfm.
4.Shields CL, Fasiuddin AF, Mashayekhi A, Shields JA. Conjunctival nevi: clinical features and natural course in 410 consecutive patients. Arch Ophthalmol 2004; 122(2):167-175.
5.Zamir E, Mechoulam H, Micera A, et al. Inflamed juvenile conjunctival naevus: clinicopathological characterisation. Br J Ophthalmol 2002; 86(1):28-30.
6.Li G, Ho VC, Berean K, Tron VA. Ultraviolet radiation induction of squamous cell carcinomas in p53 transgenic mice. Cancer Res 1995; 55: 2070-2074.
7.Wali U, Al-Mujaini A. Sebaceous gland carcinoma of the eyelid. Oman J Ophthalmol 2010; 3(3): 117–121.
8.Amezaga AO, Arregui OG, Nuño SZ, et al. Gorlin-Goltz syndrome: Clinicopathologic aspects. Med Oral Patol Oral Cir Bucal 2008; 13(6):E338-43.
9.Reddy SC, Das PK. Tumours and tumour-like lesions of the eye: A clinicopathological study from Hospital University Sains Malaysia. Malaysian J Pathol 1996; 18(2): 113 – 120.
10.O¨ zdal PC, Code` re F, Callejo S, et al. Accuracy of the clinical diagnosis of chalazion. Eye 2004; 18:135–138.
11.The Hashemite Kingdom of Jordan, Ministry of Health, Non- Communicable Disease Directorate, Jordan Cancer Registry. Cancer Incidence in Jordan 2009. http://www.moh.gov.jo/MOH/arabic/publications.php.
12.Slaughter K, Sullivan T, Boulton J, et al. Early surgical intervention as definitive treatment for ocular adnexal capillary haemangioma. Clin Experiment Ophthalmol 2003; 31(5):418-23.
13.Amoli FA, Heidari AB. Survey of 447 Patients with Conjunctival Neoplastic Lesions in Farabi Eye Hospital, Tehran, Iran. Ophthalmic Epidemiology 2006; 13:275–279.
14.Alves LF, Fernandes BF, Burnier JV, Zoroquiain P, et al. Incidence of epithelial lesions of the conjunctiva in a review of 12,102 specimens in Canada (Quebec). Arq Bras Oftalmol 2011; 74(1):21-3.
15.Coroneo M. Ultraviolet radiation and the anterior eye (Review). Eye and Contact Lens 2011; 0(0):1- 11.
16.Kale SM, Patil SB, Khare N. Clinicopathological analysis of eyelid malignancies - A review of 85 cases. Indian J Plast Surg 2012; 45(1):22-28.
17.Zürcher M, Hintschich CR, Garner A, et al. Sebaceous carcinoma of the eyelid: a clinicopathological study. Br J Ophthalmol 1998; 82(9):1049-1055.
18.Saornil MA, Becerra E, Méndez MC, Blanco G. Conjunctival Tumors Tumores. Arch Soc Esp Oftalmol. 2009; 84: 7-22.
19.Damato B, Coupland S. Management of Conjunctival Melanoma. Expert Rev Anticancer Ther 2009; 9(9): 1227-1239.
20.Ho SF, Brown L, Bamford M, Sampath R, Burns J. 5 Years review of periocular basal cell carcinoma and proposed follow-up protocol. Eye (Lond) 2013; 27(1):78-83.
21.Leibovitch I, Huilgol SC, James CL, et al. Periocular keratoacanthoma: can we always rely on the clinical diagnosis? Br J Ophthalmol 2005; 89: 1201-1204.
22.Waddell KM, Newton R. The aetiology and associations of conjunctival intraepithelial neoplasia: further evidence. Br J Ophthalmol. 2007; 91(1): 120–121.
23.Lebwohl M, Dinehart S, Whiting D. Imiquimod 5% cream for the treatment of actinic keratosis: results from two phases III, randomized, double-blind, parallel group, vehicle-controlled trials. J Am Acad Dermatol 2004; 50(5):714-721.
24.Sanjay CC, Sejal SJ, Amul PB, et al. A Histopathological study of ophthalmic lesions at a teaching hospital. National Journal of Medical Research 2012; 2(2): 133-137.
25.Alkatan HM, Al-Arfaj KM, Maktabi A. Conjunctival nevi: Clinical and histopathologic features in a Saudi population. Ann Saudi Med 2010; 30(4):306-312.
26.Kumar S. Rapidly growing pilomatrixoma on eyebrow. Indian J Ophthalmol 2008; 56(1): 83–84.
27.Balma-Mena A, Chakkittakandiyil A, Weinstein M, et al. Propranolol in the management of infantile hemangiomas: clinical response and predictors. J Cutan Med Surg 2012; 16(3):169-173.
28.Rose GE, Wright JE. Pleomorphic adenoma of the lacrimal gland. Br J Ophthalmol 1992; 76(7): 395-400.