ABSTRACT
Objectives: To study the incidence and technique for repair of lacrimal canalicular laceration at the Royal Medical Services military hospitals in Jordan.
Methods: A retrospective chart review of patients who underwent mono-canalicular or bi-canalicular laceration microscopic repair with or without stenting consecutively between May 2003 and March 2014 at Royal Medical Services Military hospitals was conducted. Collected data included: age, gender, cause of injury, time between injury and surgical treatment, affected canaliculus, other adnexal injury, coexisting ocular injury, type of stent used, duration of stenting, anatomical and functional success after removal of stent.
Results: Forty- four patients were included in this study. The mean age was 18.2 years (range 1.5- 63 year). Males represented 88.6% of the patients and females 11.4% with a ratio of 7.8:1. The lower canaliculus was injured in 68.2%, the upper canaliculus in 27.7%, and both upper and lower in 4.5% of cases. Associated ocular injuries were seen in 29.5% of cases. The most common cause of injury was falling down with direct injury to the canaliculus, 47.7%. Mini-Monoka stent was used in 75% and Mono-stent in 25% of cases. Premature stent extrusion was noticed in 18.2% of cases. The stent was removed between 3 and 6 months in 81.8% of cases. All cases had patent lacrimal drainage system after removal of stent. Postoperative epiphora not subjectively annoying to the patient was found in 61.4% of cases. Duration of follow up after stent removal ranged between 3 and 12 months, mean 6.4 months.
Conclusion: The study showed that Mono-canalicular stent for canalicular laceration is a suitable alternative to bi-canalicular stent. It is easy to perform, avoids risk of uninvolved canaliculus damage, avoids the nasal manipulation, and has no risk of punctal and canalicular cheese-wiring that lead to upper lacrimal drainage system slitting.
Key words: Canaliculus laceration, Mini-Monoka, Mono-stent.
JRMS March 2016;23 (1): 47-53 / DOI: 10.12816/0023360
Introduction
The upper lacrimal drainage system is located in the medial aspect of the lids and has a close relationship with the medial canthal tendon and the orbicularis oculi muscle.(1,2) The upper and lower canaliculi of lacrimal drainage system are mucosal ducts through which tears are drained from the lacus lacrimalis to the lacrimal sac.(3)
Each canaliculus starts with a distal opening called the punctum, the upper punctum is closer to the medial canthus, and then runs vertically for 2 millimeters and then reflects horizontally toward the lacrimal sac for another 8 millimeters. In few cases the upper horizontal canaliculus joins the lower to form a common canaliculus.(4) Because of the obvious difference between their lengths the horizontal canaliculi are more frequently injured than the vertical.(5) With the advantage of the gravity, the lower canaliculus is believed to drain 70% of the tears.(6,7) Their close relationship to the medial canthal tendon make them particularly vulnerable to shearing, avulsion, and stretching forces. Canalicular injury could be due to direct and penetrating trauma by sharp objects such as a tree branch, a dog bite or scratch, indirect trauma by a blunt object, such as a fist, resulting in avulsion of the canaliculi along with the medial canthal tendon, or diffuse trauma across the entire mid-face with multiple forces acting in several directions for injury, as might happen in road traffic accident, and this is usually associated with soft tissue and sometimes bone injury. Both the indirect and the diffuse mechanisms result in avulsion of the canalicular system.(5,7-10)
Canalicular lacerations occur infrequently and they are the most common type of traumatic injury to the lacrimal drainage system with the young adult males being more affected than females.(7-9,11,12) The horizontal limb of the inferior canaliculus is affected in more than half of the cases.(8,11-13) To prevent the risk of troublesome post-traumatic epiphora the canalicular laceration should be diagnosed, meticulously repaired, and stented early to encourage mucosal healing.(11,14) It is prudent to exclude globe injury in any patient with peri-ocular soft tissue laceration. There are controversies regarding the repair of a mono-canalicular laceration with bi-canalicular stent because of the risk of iatrogenic damage to the uninvolved canaliculus but with the advent of mono-canalicular stent such as Mini-Monoka® canalicular stent it is prudent to repair all canalicular lacerations.(8, 9)This study was conducted retrospectively to report the epidemiology of canalicular laceration and its management at the Royal Medical Services hospitals of Jordan.
Methods
Charts of patients who underwent mono-canalicular or bi-canalicular laceration microscopic repair with or without stenting consecutively between May 2003 and March 2014 at Royal Medical Services Military hospitals were reviewed. The study was approved by the local ethical committee of the Royal Medical Services. Collected data included: age, gender, cause of injury, time between injury and surgical repair, affected canaliculus (upper, lower, or both), other adnexal injury, co-existing ocular injury, type of stent used, duration of stenting, anatomical and functional success after removal of stent, length of follow-up duration. Patients with lacrimal sac and nasolacrimal duct injury were excluded.
Simple statistics such as mean, average, frequency, and percentages were used. Authors have no financial interest in products used in this study.
Surgical technique
After induction of anaesthesia (general or local), the wound is examined and appropriate debridement is done under the operating microscope. The punctum is dilated using Nettleship punctal dilator, and the mono-canalicular stent is inserted and retrieved from the distal canalicular severed end and the mono-canalicular stent is securely anchored at the punctum by the plug. The proximal end of the severed canaliculus usually needs 4- hands to find and if it is difficult to be identified. Different techniques can be used such as air, fluorescein, methylene blue, or viscoelastic injection, but these are rarely needed especially when the repair is done immediately as the lacerated canaliculus is paler than the surrounding fleshy red orbicularis oculi muscle. The stent is then introduced into the proximal severed end of the canaliculus. The medial canthal tendon is repaired with 5/0 vicryl suture and 2 to 4 peri-canalicular 8/0 vicryl sutures are used to approximate the ends of the canaliculus. Finally, the skin is sutured with 6/0 vicryl. Topical antibiotic eye-ointment is instilled, and the eye is padded for 24 hours. The patient is seen in the second day, 1 week, 1 month, and every 3 months postoperatively. The patient is given topical antibiotic and steroid eyedrops and topical eye-ointment for 1 week. The stent is removed after 3 to 12 months if it has not extruded spontaneously.
Results
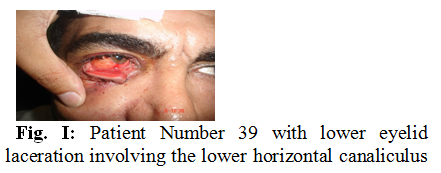
Forty- four patients with canalicular laceration were included in this study. The mean age was 18.2 years (range 1.5- 63 year). Thirty- nine (88.6%) of the patients were males and 5 (11.4%) were females with a ratio of 7.8:1. The right side was affected in 56.9% and the left side in 43.1%. The lower canaliculus was injured in 30 (68.2%) cases (23of them was due to laceration, one patient had 2 lacerations in the same canaliculus, and 7 cases was due to avulsions). The upper canaliculus was injured in 12(27.7%) cases (11 were due to laceration and 1 due to avulsion). Unilateral upper and lower canalicular injury was found in 2(4.5%) cases. Associated lid laceration(s), in addition to the primary canalicular laceration, were seen in 5(11.4%) cases. Fig.1 shows an example of associated lower canalicular and eyelid margin laceration, patient number 39. Associated ocular injuries such as corneal abrasion and retinal hemorrhage were seen in 13(29.5%) cases (8 patients had lower canalicular laceration, 3 had upper canalicular laceration, and 2 had unilateral bi-canalicular laceration).
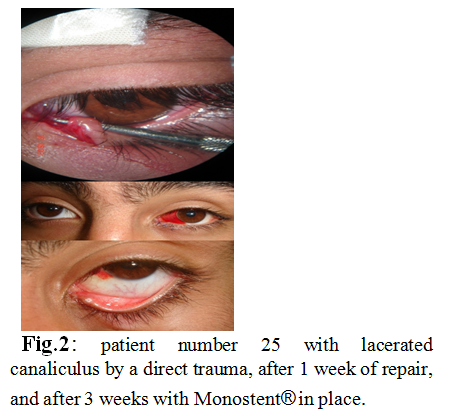
None of the patients had associated penetrating globe injury. The injuries were caused by direct trauma with sharp object in 6 (13.6%) cases, falling down on sharp or blunt objects in 27 (61.4%) cases, road traffic accident in 7 (15.9%) cases, and sport or physical assault in 4 (9.1%) cases, Table I. An example of lacerated canaliculus caused by a direct trauma is shown in patient number 25, Fig.2.
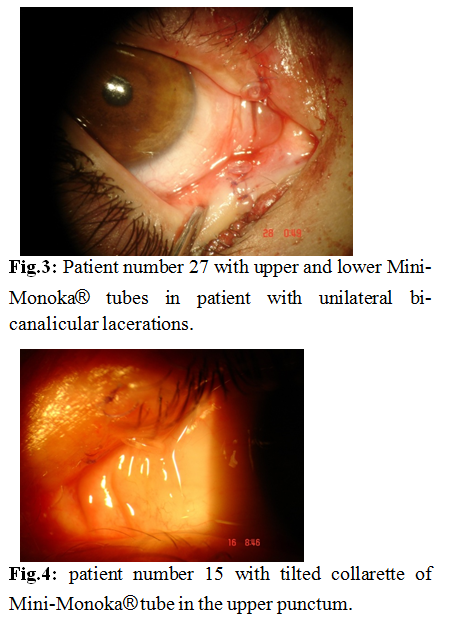
Mini-Monoka
stents (FCI Ophthalmics, Marshfield Hills, MA) were used in 33 (75%), 2 of them
had upper and lower lacerations as seen in Fig.3. Mono-stent (Eagle Vision
Inc., Memphis, TN) were used in 11(25%) cases. No patient had bi-canalicular stent.
Premature stent extrusion was found in 8 (18.2%) cases all of them had mono-stent
repair (7 cases extruded after 3 weeks, and one after 4 weeks) and all required
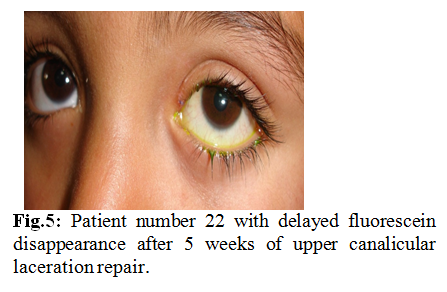
reinsertion of another stent, Table I. One case of Mini-Monoka® stents patients had conjunctival granuloma and 2 cases with
upper stents had corneal erosion because the tube collarettes were tilted
toward the cornea and required repositioning of the stents. Fig.4 shows
case number 15 with tilted collarette of Mini-Monoka tube in the upper punctum.
Duration of stenting ranged between 3 months and 1 year with the majority being
removed from 3 to 6 months (81.8%) after repair, Table II.
Canalicular syringing with normal saline, with or without fluorescein stain, revealed patent lacrimal drainage system after removal of stent in all cases. Insignificant epiphora, not interfering with daily activities or visual acuity in patients with delayed fluorescein disappearance was seen in 27(61.4%) cases, 2 of them had upper and lower laceration and 2 had premature extrusion of stent, Table I. Delayed fluorescein disappearance after 5 weeks of repair is shown in patient number 22, Fig.5. Duration of follow up after stent removal ranged between 3 and 12 months, mean 6.4 months.
Table I: Mechanism of injury, time between
injury and repair, type of stent, and functional and anatomical success of
surgery.
|
Mechanism of trauma
|
Number of patients
|
Time of surgery
|
Type of stent
|
Success
|
|
Mini-Monoka
|
Monostent
|
Anatomical
|
Functional
|
|
Direct trauma with sharp object
|
6
|
All at the same day of injury
|
4
|
2
|
6
|
4
|
|
Falling down with direct injury
|
21
|
All at the same day of injury
|
17
|
4
|
21
|
7
|
|
Falling down with indirect injury
|
6
|
5 same day and 1 second day
|
3
|
3
|
6
|
3
|
|
Road traffic accident
|
7
|
2 same day and 5 second day
|
7
|
0
|
7
|
2
|
|
Assault or sport
|
4
|
1 same day and 3 on the 3rd day
|
2
|
2
|
4
|
1
|
|
Total
|
44
|
35 1st Day, 6 2nd Day, 3 3rd Day
|
33
|
11
|
44
|
17
|
Table II: Duration of stenting, lacerated
canaliculus, and type of stent.
|
Duration
of stenting
|
Lacerated Canaliculus
|
Type of stent
|
|
Lower
|
Upper
|
Both
|
Mini-monoka
|
Monostent
|
|
3-6
months
|
26
|
10
|
0
|
25
|
11
|
|
6-9
months
|
2
|
2
|
0
|
4
|
0
|
|
9-12
months
|
2
|
0
|
2
|
4
|
0
|
|
Total
|
30
|
12
|
2
|
33
|
11
|
Discussion
The canalicular laceration is easily overlooked when associated with eyelid laceration by the treating ophthalmologist at emergency unit. This may explain why the canalicular laceration was infrequent in our study with an average of 3.7 cases per year. Canalicular lacerations occurred predominantly in young males (88.5%) with median age of 18.2 years and this agrees with most of previous studies where the majority of cases occurred in children and in patients below 30 years of age with a median age of 20 years.(7-9,11-14)
The lower canaliculus was the most commonly affected 68.2% of cases followed by upper in 27.7%, then both upper and lower in 4.5%. It compares well with the results of Kennedy and associates (66.2%, 27.5%, and 6.3% respectively) but slightly different from Naiket al (54.1%, 33.3%, and 12.5%). (8,11)
The cause of canalicular laceration in children varies between regions and ethnic groups. While the most common cause in Kennedy and associates (11) study was due to dog bites or scratches, in Naik et al, (8)study it was due mothers’“blouse hook fastener” during breast feeding. In our study the most common cause was due to falling down on sharp or blunt objects with direct trauma to the canalicular system during playing in children and road traffic accidents, sport activity or assault in adult (25%).
The majority of patients had single lid laceration or avulsion involving the canalicular system and only 11.4% of cases had multiple lid lacerations, most of them were due to road traffic accidents. The associated ocular injuries were found in 29.5% of cases and this agrees with previous studies were the incidence ranges from 20% to 40%.(8,13,15) Other studies showed that ocular injuries are more frequently associated with upper canalicular laceration.(8,13) On contrary, in our study associated ocular injuries were more frequent with lower canalicular laceration (61.5%) especially blunt trauma. Both cases of bi-canalicular laceration had associated ocular injury and this may be related to the strength and mechanism of injury.
Most of the cases were treated in the same day of injury (79.5%), 6 (13.6%) cases in the second day, and 3 (6.8%) cases in the third, all of the last group were due to physical assault and presented late because they were concerned to get involved legally. In comparison with other studies the duration between injury and repair in our study was longer than Herzum and associates(15) (3.3 hours) and shorter than Naik et al, (32 hours).(8)
In spite of the considerable debate on treatment of lacerated canaliculus the second author, oculoplastic surgeon, prefers to treat all patients with mono-canalicular stent to decrease the morbidity that may ensue if left untreated as most of the affected patients are young.(7-9,11-15) Although bi-canalicular stent has the privilege of bringing the avulsed medial canthal tendon into its normal anatomical position, helps approximating lacerated ends, and has better lacrimal drainage while it is in the lacrimal drainage system but it has the disadvantages of being technically demanding procedure and risks the uninjured canaliculus. In our center we prefer to use mono-canalicular stent to repair lacerated canaliculus because it is easy to perform, avoids the nasal and uninvolved canaliculus manipulation, and has no risk of punctal and canalicular cheese-wiring that lead to slitting and may lead to further functional epiphora. Three quarters (75%) of patients had mini-Monoka® stents and (25%) had Monostent®.
Previous studies found anatomical canalicular patency with no epiphora when mono-canalicular stents were used for bi-canalicular laceration.(8,16-18) In this study, 2 patients had bi-canalicular mono-canalicular stents, one in each canaliculus, both had anatomical patency with insignificant epiphora that does not interfere with daily activities or visual acuity.
Previously reported premature stent loss was 11% and 29% in two different studies that occurred between 2 to 3 weeks after repair.(8, 13, 15) Premature stent extrusion in this study was found in about one fifth of patients, all had Monostent® after 3 to 4 weeks that required insertion of another stent. None of the patient with mini-Monoka stents had premature extrusion and this may be because the stent is securely anchored at the punctum by the plug.
Two cases with upper mini-Monoka stents had corneal erosion and required re-positioning of the stent and properly anchoring the plug to the puncta. There is a considerable debate on how long should the lacerated canaliculus be stented but in general the duration of stenting ranged from 3 months to 1 year in most of the studies.(8, 16, 20, 21) In this report stents were left for one year, only removed earlier if complicated. The majority of stents (81.8%) were removed between 3 and 6 months.
Patency of the lacrimal drainage system after removal of stent does not necessarily mean absence of epiphora, which could be due to partial obstruction or stricture of the injured canaliculus or improperly positioned punctum (punctual ectropion). In this study, anatomical lacrimal drainage system patency was found in all cases but 61.4% of them had postoperative epiphora not subjectively annoying to the patient. Those patients had delayed fluorescein disappearance and usually had more tearing in the affected eye with outdoor activities. Only 2 patients with early stent extrusion had epiphora which was insignificant, and this agrees with Smit and Mourits(22) who proposed that re-anastomosing the lacerated canaliculus is not required to prevent epiphora in single lacerated canaliculus.
This study has limitations such as being a retrospective with relatively small number of patients over a long period of time, and lack of sophisticated investigations such as dacryocystography to assess the anatomy of the lacrimal drainage system after removal of the stent.
Conclusion
This is a report of the Royal Medical Services Hospital 11 year experience in repair of severed lacrimal canaliculi. Mono-canalicular stent for canalicular laceration is a suitable alternative to bi-canalicular stent. It is easy to perform, avoids risk of uninvolved canaliculus damage, avoids the nasal manipulation, and has no risk of punctal and canalicular cheese- wiring that lead to upper lacrimal drainage system slitting.
References
1.Wormald PJ,Van Renen G,Perks J, et al. The effect of total intravenous anesthesia compared with inhalational anesthesia on the surgical field during endoscopic sinus surgery. Am J Rhinol 2005;14:514-520.
2.Boezaart AL,Van Der Merwe,Coetzee A. Comparison of sodium nitroprusside and esmolol induced controlled hypotension for functional endoscopic nasal surgery. Can J Anesth 1995;42:373-376.
3.Balseris S,Martin Kenas JL. Complications of functional endoscopic sinus surgery. Medicinos Teorija Ir Praktika 2000;2:34-37.
4.Jacobi KE,Bohm BE,Richauer AJ, et al. Moderate controlled hypotension with sodium nitroprusside does not improve surgical conditions in endoscopic sinus surgery. Clin Anesth 2004;12:202-207.
5.Athanasiadis T,Beule AG,Wormald PJ. Effects of topical randomized controlled trial. Am J Rhinol 2007;21:737-742.
6.Guice NL. Hot water in epistaxis. Miss Valley Med Month 1884;4:3-4.
7.Stangerup SE,Dommerby H,Lau T. Hot water irrigations as a treatment of posterior epistaxis. Rhinology 1996;34:18-20.
8.Ahmed S,Mohammed SI,Mohammed HAEF. Topical tranexamic acid versus hot saline for field quality during endoscopic sinus surgery. The Egyptian Journal of Otolaryngology 2014;30(4):327-331.
9.Stangerup SE,Thomsen HK. Histological changes in the nasal mucosa after hot water irrigation:an animal experimental study. Rhinology 1996;34:14-17.
10.Snyderman CH,Pant H,Carrau RL, et al. What are the limits of endoscopic sinus surgery?The expanded endonasal approach to the skull basa. Keio Journal of Medicine 2009;58(3):152-160.
11.Ozmen S,Ozmen OA. Hot saline irrigation for control of intraoperative bleeding in adenoidectomy:a randomized controlled trial. Otolaryngol Head Neck Surg 2010;142:893-897.
12.Gan EC,Alsaleh S,Manji J, et al. Hemostatic effect of hot saline irrigation during functional endoscopic sinus surgery:a randomized controlled trial. Int Forum Allergy Rhinol 2014;4(11):877-884.