Introduction
Congenital heart diseases considered one of the most common birth defect that cannot be overlooked in the advanced childhood nor adulthood ages. However, it is sometimes hard to detect such lesions or defects via the ordinary postnatal routine studies.
These anomalies could be either stenotic congenital lesions (obstruction to Right Ventricular (RV) or Left Ventricular (LV) outflow, subvalvualr, valvular, supravavular, obstruction to LV inflow (congenital mitral stenosis, cor triatrium), and narrowing in the great vessels (aortic coarctation, branch Pulmonary Artery (PA) stenosis, or it could be congenital regurgitant lesions, atrioventricular communications (Shunts), Abnormal chambers and great vessels connections and many others. Only those that either can safely or silently continue without treatment untill late ages are slightly limited to a smaller group such as bicuspid aortic valve, Ventricular Septal Defect (VSD) or Patent Ductus Arteriosus (PDA). To predict the future burden of congenital heart defects in adults on health care systems, various studies have made to evaluate the size of this group of patients. Various methods have been used to predict this such as calculation, evaluation of birth rates, prevalence of congenital heart diseases, and survival estimates, or by collecting all CHD cases from administrative database.(1-3) All of these methods have pitfalls and the ideal method to estimate the prevalence of adults with CHD has not been yet determined.
Method
This was a retrospective study looking at catheterization and surgical records of all adult patients (18 years or older) with congenital heart disease who were treated at QAHI between January 2004 and April 2014. All cases with acquired cardiac diseases were excluded from our study. Their demographic characteristics, mode of presentation, investigations, and subsequent management were looked at.
Results
We had 517 patients who had adult congenital heart diseases, with 51% males and 49% females. The age ranged from 18 - 62 years with a mean of 29.5 years. The commonest presenting symptoms encountered were effort intolerance, which was seen in 360 patients (70%). An incidental finding of a heart murmur on cardiac auscultation was seen in 88 patients (17%). 78 patients (15%) had palpitation, 41 (8%) had cyanosis, 15 (3%) had chest pain, 5 (1%) had hypertension, one patient had migraine and another had atrial fibrillation. One hundred and fifty patients (26%) had previous cardiac surgery, 11 patients (2%) had previous catheter based interventions and three patients (0.6%) had both.
The commonest congenital heart disease diagnosis encountered was Atrial Septal Defect (ASD) Fig.1, which was seen in 114 patients (22%) and in 8 patients it was associated with Partial Anomalous Pulmonary Venous Connection (PAPVC). 61% of these cases were treated by device closure in the catheterization lab, while the rest were closed surgically because they were either too large or with deficient rims that cannot hold a device. Two ASD cases were managed medically because patients presented late and already had severe pulmonary hypertension, contraindicating any closure. All cases with PAPVC were closed surgically. One patient who had migraine and a small ASD had device closure in the catheterization lab.
Three patients had Patent Foramen Ovale (PFO). Two were closed by a device because of history of Transient Ischemic Attach(TIA) and one were managed medically as there was no indication to close his defect. One patient had AtrioVentricular Canal (AVC) defect, which was closed surgically. Ventricular Septal Defects (VSD) are not uncommon CHD that can be seen in adults. We had 41 cases (7.9%) in our study, four of them had surgical or interventional correction for other CHD before. Seven were closed by cardiac catheterization; two by surgery as part of a repair for other defects and the rest were managed medically because of no hemodynamic effects or due to the presence of severe Pulmonary Hypertension (PHTN) which will not be reversed by closure.
Forty three patients (8.3 %) had Coarctation of Aorta (COA) and 30 of them were managed by cardiac catheterization (either by balloon dilatation or stenting). Four other cases were catheterized because of suspicion of re-coarctation as they had previous coarctation repair or balloon and had clinical evidence of coarctation (hypertension). No coarctation was found and all were managed medically. Patent ductus arteriosus (PDA) Fig.2 was found in 15 patients (2.9%). One was surgically closed because the shape is inappropriate for device closure, 12 were closed by devices while two of them were managed medically.
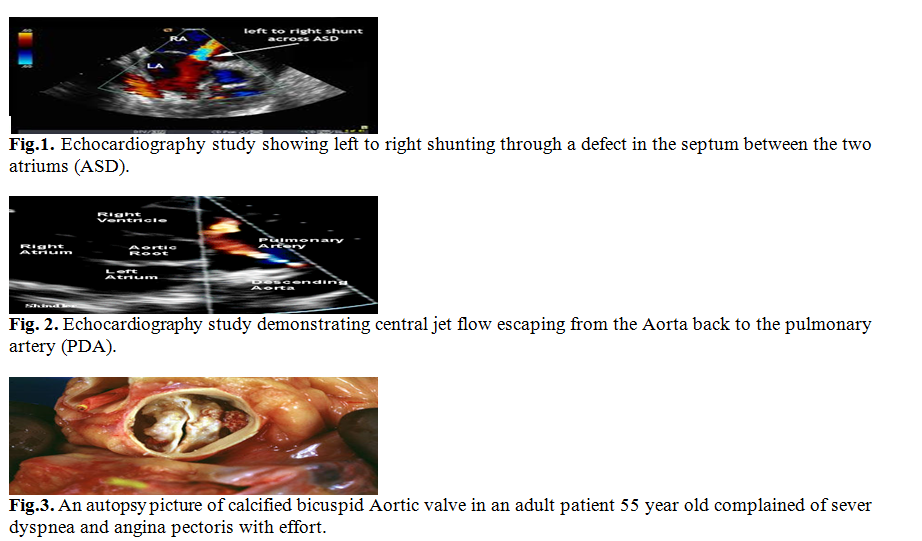
Table I: Types of defects found in patients with CHD and their fate.
Case | Total no. | Previous Surgery or intervention | Fate |
Surgery | Intervention | Medical Rx |
ASD | 114 | 0 | 43 | 70 | 1 |
PFO | 3 | 0 | 0 | 2 | 1 |
ASD + PAPVC | 8 | 0 | 8 | 0 | 0 |
AVC | 1 | 0 | 1 | 0 | 0 |
VSD | 41 | 4 | 2 | 7 | 32 |
COA | 43 | 4 | 9 | 30 | 4 |
PDA | 15 | 0 | 1 | 12 | 2 |
PS | 30 | 8 | 2 | 24 | 4 |
PR | 85 | 80 | 85 | 0 | 0 |
SAM | 9 | 4 | 5 | 0 | 4 |
MR | 30 | 8 | 25 | 0 | 5 |
AR | 20 | 8 | 14 | 0 | 6 |
AS | 16 | 0 | 6 | 4 | 6 |
DCRV | 4 | 0 | 4 | 0 | 0 |
TR | 6 | 3 | 0 | 0 | 6 |
Complex CHD | 20 | 6 | 9 | 0 | 11 |
S/P TCPC | 22 | 22 | 0 | 14 | 8 |
PHTN | 41 | 3 | 0 | 0 | 41 |
Coronary aneurysm | 2 | 0 | 0 | 0 | 2 |
AVMs | 3 | 0 | 0 | 3 | 0 |
Rupture SOV | 3 | 0 | 3 | 0 | 0 |
Vascular ring | 1 | 0 | 0 | 0 | 1 |
| | | | | |
Total | 517 | 150 | 217 | 166 | 134 |
Percent (of 517) | | 29% | 42% | 32% | 26% |
Pulmonary valve Stenosis (PS) is another condition faced in adults with CHD. We had 30 patients (5.8%) with PS, 8 had previous cardiac surgery. 24 were managed by balloon angioplasty; two by surgery because of associated branch pulmonary stenosis and four were followed up because of mild stenosis.
Eighty five (16.4%) patients had significant Pulmonary valve Regurgitation (PR). In the majority, it was due to previous surgeries (80); especially tetralogy of Fallot or balloon angioplasty.(2) All were managed by surgical pulmonary valve replacement using Contegra or Hancock valves.
Nine patients (1.7%) had SubAortic Membrane (SAM). Five were excised surgically and the other four did not cause a significant pressure gradient or aortic incompetence to warrant any intervention.
Aortic or mitral valvular lesions are also encountered in adult population because of either congenital or previous surgery. Significant Mitral Regurgitation (MR) was found in 30 patients (5.8%) who were all managed by surgical replacement of the valve. Eight of them had previous surgery. Aortic Regurgitation (AR) was found in 20 patients (3.9%). Eight of them had previous surgery for the aortic valve or other associated congenital heart disease. Fourteen were replaced surgically and six were managed medically due to insignificant regurgitation. Sixteen patients (3.1%) had Aortic Stenosis (AS) Fig. 3. Six were managed surgically, four were managed by balloon aortic Valvuloplasty and the rest were followed up.
Double Chamber Right Ventricle (DCRV) was seen in four patients and all were surgically repaired.
Tricuspid valve Regurgitation (TR) as part of Ebstein anomaly or because of other associated CHD was seen in 6 patients (1.1%) and all were managed medically because there was no indication for repair. Twenty patients (3,9%) had complex cyanotic CHD. Six of them had previous palliative procedures and were not amenable for total surgical repair.
Twenty two patients (4.2%) had Fontan surgery (TCPC) for single ventricle, 14 of them had transcatheter closure of significant fenestra. Pulmonary hypertension was found in41 patients (7.9%). Thirty one were found to have primary Pulmonary Hypertension (PHTN) and 10 were found to have cardiac cause of their PHTN.Three of them previous repair. All were managed medically.
Two patients had coronary aneurysms; three patients had arteriovenous malformations,Three patients were found to have ruptured Sinus of Valsalva (SOV) and were repaired surgically. One patient was found to have incomplete vascular ring. The distribution of cases and their fate is illustrated in Table I.
Discussion
Accurate data on the proportion and composition of adult population with CHD are still lacking. This is the first study looking at adult population with CHD in our center. The marked advances in surgical and interventional techniques have made the population of adults with CHD larger and more diverse. In addition, some congenital lesions may be diagnosed for the first time when the patient is in his adulthood such as ASD, Aortic Coarctation, Ebstein anomaly and corrected transposition of Great vessels. More than 90% of children born with congenital heart disease survive into adulthood due to successes of cardiac surgery and medical management.(4)
The 32nd Bethesda Conference reported in 2000, that the estimated ratio of congenital heart diseases in the United States could reach about 2800 adults per 1 million populations, with more than half of them having moderate or high complexity of their defect.(2)In Europe the estimated number of adults with CHD are about1.2 million patient while in the USA about one million.(5-7) In a study by Gurvitz et al,(8) it was found that gaps in medical care were more common to occur by age 19 years when the transition from pediatric to adult care has completed. These gaps were more common in patients with mild to moderate lesions and in particular locations. A 3-year gap in medical care was found in 42% of patients, with 8% having gaps longer than a decade.
Although there have been major advances in interventional cardiology to treat adults with CHD nowadays, surgery remains an important treatment option, with about of 20% of hospital admissions for adults with CHD being for cardiovascular surgery.(9-11)
A majority of patients (70%) who required surgery in adulthood were operated for the first time ever. In concordance with current literature, these patients were mostly adults with atrial septal defect and aortic stenosis.(12)
Many adults with congenital heart disease will require cardiac surgery or intervention for their heart defects. In a study by Zomer et al, 20% of adults required surgery during a 15-year period; in 40%, the surgery was a reoperation. Males with CHD had a higher chance of undergoing surgery in adulthood and had a consistently worse long-term survival after reoperations in adulthood compared with females. Most reoperations in adulthood were seen in tetralogy of Fallot patients (20%); in those patients, 37% of reoperations were pulmonary valve replacements.(13)
In our study, 217(38%) required open-heart surgery. 26% were reoperations. Patients with pulmonary valve replacement especially post Tetralogy of Fallot repair, mitral and aortic valve replacement constituted most of cases requiring surgery. One hundred sixty patients (29.1%) needed intervention by cardiac catheterization. Most of these were patients with ASD, coarctation of aorta and pulmonary valve stenosis. The highest rate of catheter- based intervention was noticed in the last five years of our study and this is why we have over all higher rate of surgical management.
The rest of patients (23.5%) are under medical treatment because of mild defects or untreatable illness. These are hoped to decline in the future by the advances in surgical and interventional procedures.
Conclusion
Adults with CHD are being encountered more commonly nowadays. Due to the rapid development in methods of detection, congenital heart diseases become easily discovered. A high index of suspicion should be present for any patient with effort intolerance or previous cardiac intervention or surgery regardless of the age. Interventional cardiac catheterization is increasingly taking over cases as the mode of treatment for cases that were managed surgically before.
Study limitations
There are no current estimates of the prevalence of CHD in adults in Jordan. In this study, we tried to get general idea from our catheterization and surgical records as most of the adults with significant defects would undergo either cardiac catheterization or cardiac surgery at our center. We could not track all patients especially the non-Jordanian with CHD because there is no such registry that contains the records of these patients up to date so we are advocating for development of such a registry at the national level. Although most cases of CHD and adults were managed in our center, a small proportion was managed in the private sector and university hospitals and were not included in this study.
References
1.A.J. Marelli, A.S. Mackie, R. Ionescu-Ittu, et al. Congenital heart disease in the general population: changing prevalence and age distribution. Circulation, 115 (2007), pp. 163–172
2.C.A. Warnes, R. Liberthson, G.K. Danielson, et al. Task force 1: the changing profile of congenital heart disease in adult life. J Am Coll Cardiol, 37 (2001), pp. 1170–1175
3.D. van der Linde, E.E.M. Konings, M.A. Slager, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol, 58 (2011), pp. 2241–2247
4.Asp A, Bratt EL, Bramhagen AC. Transfer to Adult Care-Experiences of Young Adults with Congenital Heart Disease. J Pediatr Nurs. 2015 Jul 18. pii: S0882-5963(15)00213-4.doi: 10.1016/j.pedn.2015.05.025.
5.Hoffman JI, Kaplan S, Liberthson RR. Prevalence of congenital heart disease. Am Heart J. 2004;147:425– 439.
6.Moons P, Engelfriet P, Kaemmerer H, et al. Delivery of care for adult patients with congenital heart disease inEurope: results from the Euro Heart Survey. Eur Heart J. 2006;27: 1324–1330.
7.Brickner ME, Hillis LD, Lange RA. Congenital heart disease in adults: first of two parts. N Engl J Med. 2000; 342:256 –263.
8.Michelle Gurvitz, Anne Marie Valente, Craig Broberg, et al. Prevalence and Predictors of Gaps in Care Among Adult Congenital Heart Disease Patients. Journal of the American College of Cardiology. Vol. 61, No. 21, 2013.
9.Somerville J. Management of adults with congenital heart disease: an increasing problem. Annu Rev Med. 1997;48:283–293.
10.Stellin G, Vida VL, Padalino MA, et al. Surgical outcome for congenital heart malformations in the adult age: a multicentric European study. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;7:95–101.
11.Billett J, Majeed A, Gatzoulis M, et al. Trends in hospital admissions, in-hospital case fatality and population mortality from congenital heart disease in England, 1994 to 2004. Heart. 2008;94:342–348.
12.Vida VL, Berggren H, Brawn WJ, et al. Risk of surgery for congenital heart disease in the adult: a multicentered European study. Ann Thorac Surg. 2007;83:161–168.
13.A.C. Zomer, C.L. Verheugt, I. Vaartjes, et al. Surgery in Adults with Congenital Heart Disease. Circulation. 2011;124:2