Objective: To evaluate the shoulder functional outcome in
children with obstetrical brachial plexus palsy after performing
latissimus dorsi muscle transfer and subscapularis muscle release.
Methods:
this is a retrospective analysis to fifty patients with 52 shoulders
underwent latissimus dorsi muscle transfer and subscapularis muscle
release for obstetrical brachial plexus palsy, between June 2008 and
April 2012. Reviewing patient’s files and pre-operative videos. Mallet
scoring system was used to evaluate the shoulder functional changes.
Results:
Fifty children with fifty two shoulders with a ranging age between 18
months up to 13 years were involved in this study, 1:1 male to female
ratio, the average birth weight was 3.89KG, the brachial plexus extent
of injury were ranging from upper injury 80% to total palsy 20%.
Regarding the affected limb the right side involvement was 60% the left
side 36% and bilateral involvement was 4%.there is significant
difference in the global upper limb function between younger age
group(below five years) when compare to older age group(above five years
of age). Five active ranges of motion around the shoulder joint
involved in the injury were analyzed with the following functional
outcome improvement: Global Abduction 46.6%, Global External Rotation
62.9%, Hand to neck 49%, Hand to spine 53.3%, Hand to mouth 57.2%
Conclusion:
we found that this type of surgery improves the global function of the
upper limb in patients with obstetrical brachial plexus palsy, this
improvement become less remarkable in older children(>5years of
age). And the majority of patients and their families were satisfied by
the achieved results.
Key words: Latissimus dorsi muscle transfer, Obstetrical brachial plexus palsy, Subscapularis release.
JRMS June 2015; 22(2): 45-50 / DOI: 10.12816/0011367IntroductionObstetrical brachial plexus palsy is a disabling condition resulting in permanent dysfunction of the upper limb,(1) with contracture deformities and muscle imbalance, usually causing a psychological impact. The severity of the deficit is determined by the extent of the injury and can be described as upper brachial plexus palsy, extended upper brachial plexus palsy, lower brachial plexus palsy and total involvement.(1,2)
Treatment is based on two pillars: the surgical management and the physiotherapy and rehabilitation program. Surgical management includes primary procedures that consist of reconstruction of the brachial plexus and secondary procedures directed to improve the function of the upper limb. These secondary procedures may include soft tissue release, muscle transfer, humeral osteotomy or shoulder arthodesis.(1,3-10) We present herein a retrospective study of the functional outcome of 52 shoulders with obstetrical brachial plexus palsy in 50 patients that underwent a transfer of the latissimus dorsi muscle to the infraspinatous tendon associated with a release of the subscapularis muscle.
The aim of this study is to functionally evaluate the improvement in active range of motion (ROM) after undergoing a secondary procedure, specifically including only patients who underwent latissimus dorsi muscle transfer and subscapularis muscle release using the Mallet Scoring to measure the outcome of improvement objectively.
Methods From June 2008 and April 2012 sixty seven patients were operated for obstetrical brachial plexus palsy. Seventeen patients were lost from the follow-up and were accordingly excluded from this review. In total, the data available from the medical records of fifty patients were collected for retrospective review and analysis with a mean follow-up of 4 years, ranging from 2 to 5.6 years. All shoulders had pre-operative limited external rotation associated with internal rotation contracture (positive trumpet sign). And no humeral head deformity, subluxation or dislocation as evaluated by CT scan, they all underwent a transfer of the latissimus dorsi muscle to the infra-spinatous tendon associated with a release of the sub-scapularis muscle by the senior author, as previously described in the literature(7) and shown in Fig. 1 and 2. Surgical procedure was regularly performed under general anaesthesia with lateral decubitus position. A pre-operative functional evaluation by the same occupational therapist specialized in obstetrical brachial plexus injuries was done for all patients, and
 Fig. 1:
Fig. 1: the lateral position of the patient on the operating table and the drawing of the incision on the lateral border of the scapula and extending up to the head of humerous posteriorly.
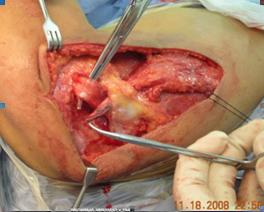 Fig. 2:
Fig. 2: the Latissimus Dorsi Muscle after complete release with preservation of the pedicle neurovascular supply transfer to the infraspinatous and teres minor muscles.

 Fig. 3:
Fig. 3: The mallet grading system used for pre and post operative evaluation.
repeated at 12 months post-operative and at the final follow-up. All evaluations were scored according to Mallet scoring system(8,11) and documented with video film registrations. In post-operative, the shoulder were immobilized in a spice at 90 degrees abduction and maximum external rotation for six weeks, followed by a night splint for an additional period of six weeks with regular physiotherapy visits.
The Mallet classification scoring system was used to evaluate the functional improvement having grade I as absent range of motion and grade V as normal range of motion. Fig. 3.
ResultsThe medical records of 50 patients with 52 shoulders presenting an obstetrical brachial plexus palsy were available for a retrospective analysis. Gender distribution was equal. The right side was affected in 30 patients (60%). The left side in 18(36%), and bilateral injury was present in 2 patients (4%). The birth weight ranged from 2.5 kg to 5.5 kg, with a mean of 3.89kg the mean age at the time of surgery was 5.2 years, ranging from 18 months to 13 years.
Each patient function was graded pre and post operatively and an increase in the function of one grade was given 25 % improvement having grade I as 0% and grade V as 100%. Interestingly there was an increase in the function outcome of the global abduction of 46.6%, global external rotation by 62.9%, hand to neck by 49%, hand to spine by 53.3% and hand to mouth by 57.2%.we can compare the result of patients under 5 years of age at time of surgery and those above 5 years as seen in Chart I to find significant difference in the all ROM functions. And the ROM much better with upper OBPP than with total palsy.
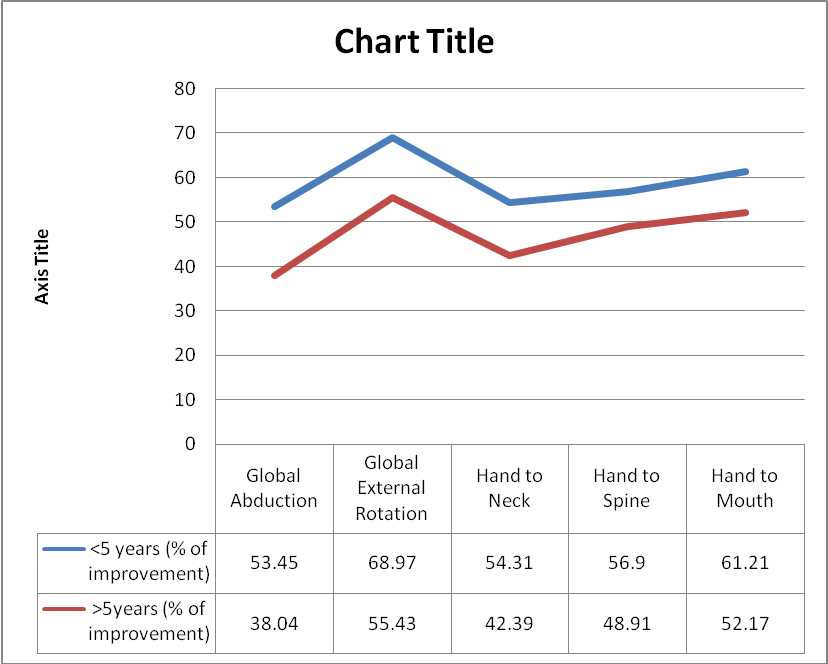
Chart 1: Shows the difference of improvement between the 2 main subgroups as explained by the graph.
DiscussionBirth-related upper limb paralysis was first described in a midwifery text by Smellie 1764(12) thought Erb localized the point of the lesion at the brachial plexus in which it bears his name now. Tachdjain et al describes that in
spite of the huge advancement in obstetrical medicine and the recognition of the risk factors during pregnancy going through delivery and the ability to induce labor or even to deliver a child by caesarian section and the introduction of ultrasonography all have succeeded in reducing the incidence of Obstetrical brachial plexus palsy.(13) Unfortunately all this advancement could not eliminate the occurrence of such a condition, and the incidence remains at 0.3 to 4.5 per 1000 live birth.(13,11)
The most common persistent and progressive deformity after obstetrical brachial plexus palsy is restricted external rotation of the shoulder joint, which is usually associated with internal rotation contracture leading to skeletal deformities such as coracoid elongation, hooked acromion, flattening of the humeral head resulting in a dysplastic joint liable to subluxation or even dislocation.(14,15,16)
The decision of undergoing a secondary procedure and the outcome depends on patient’s age, compliance to physiotherapy, type and extent of injury and carful assessment to the glenohumeral joint.
There is still no clear guidelines concerning the optimum management and timing for children with weakness around the shoulder resulting from obstetrical brachial plexus injuries, in most cases tendon transfer was recommended in the absence of glenohumeral incongruity or deformity.(17,6) In relation to the best age, in the hoffer and Phipps series the average age at surgery was 2.5 years.(18) Although if the glenohumeral joint is still congruent other authors advice tendon transfer up to the age of 10 years.(19) In our study we recommend the age for best results under 5 years though older age groups can benefit, as seen in Table I. El-Gammal et al,(17) evaluate 109 patients after tendon transfer around the shoulder, and he concluded that improvement of abduction and external rotation negatively correlate with the age at surgery, and were significantly higher in patients operated younger than 4 years. Terzis et al,(16) stated in her study that 35 out of 53 patient underwent latissimus dorsi transfer with long term follow-up (>5 years), and the results were remarkable for external rotation (mean 62º±22º) and
Table I: Patients Age, weight pre and post operative changes and method of measurement of improvement