Spontaneous
biliary duct perforation is a rare yet important entity presenting in
infants. The usual presentation is jaundice and failure to thrive
occurring in a previously healthy infant. The diagnosis is usually the
function of hepatobiliary imaging. In this case report Tc99m-DISIDA
hepatobiliary imaging was an accurate tool to diagnose this surgically
correctable disease.
Key words: Common Bile Duct Perforation, Hepatobiliary scan, Tnfants, Tc99m-DISIDA.
JRMS June 2015; 22(2): 55-58 / DOI: 10.12816/0011371 IntroductionSpontaneous
perforation of the common bile duct in infancy is a rare disorder, but
it is second to biliary atresia as a cause of surgical jaundice in the
infant. First described in 1932, fewer than 150 cases have been reported
to date.(1-3) The etiology is unknown though distal obstruction and
congenital mural weakness in the bile duct wall have been postulated.
Trauma, ischemia, distal biliary obstruction, and pancreatic reflux
appear also to be causative etiologies.(1) We present a case of
Spontaneous common bile duct perforation (SBP) in a 5-month-old male
baby which was clearly demonstrated by Tc99m Disofenin (Tc99m- DISIDA)
hepatobiliary scan.
Case ReportWe report a
five-month-old male infant who was delivered by normal vaginal delivery
at 29 weeks of gestation. At birth he was admitted to the neonatal
intensive care unit with some respiratory complications due to
immaturity. He recovered completely and was discharged in good general
condition. He did well and was thriving till he presented at 5 months of
age with yellowish discoloration of the skin and sclera, clay colored
stool and severe distention of the abdomen, with deterioration in
feeding and weight. There was no history of trauma and the infant had
been in good health before this.
On physical examination, he was
afebrile but distressed. The abdomen was distended with shifting
dullness and 43cm girth. There was bilateral huge hydrocele.
Total
serum bilirubin was 17 mg/dl, direct bilirubin 7 mg/dl, alkaline
phosphatase (ALP) 1531 units/L, ALT 54 units/L, total protein 56 g/L,
albumin 33 g/L, cholesterol, and 0.7mmol/L. The prothrombin time (PT)
was 15s and the partial thromboplastin time (PTT) was 44s and the INR
1.2. Urine was dark color with normal analysis, and the stool was free
of bilirubin. His Hemoglobin was 9.1g/dl, WBC 7620/uL and platelets
700,000 /uL. A diagnostic peritoneal tap revealed greenish fluid.
Analysis of the ascitic fluid revealed WBC at 60 with 79%
polymorphonuclear cells, 18% lymphocytes, and cholesterol at 7.4 mM.
Gram stain and cultures for the blood and ascetic fluid were negative.
Finally Hepatitis B surface Antigen (HBs Ag) and Hepatitis C Virus
Antibodies (HBV Ab’s) were negative.
The infant’s chest X-ray was
normal. An ultrasound of the abdomen showed a large amount of free
fluid with a slightly small echogenic liver. Neither the gallbladder nor
the biliary tract were seen, both kidneys and spleen appeared normal.
Hepatobiliary
radionuclide imaging using an age-weight-adjusted dose of
Tc99m-Disofenin was done. Dynamic images with 1 second frames for 60
seconds followed by 1 minute frames for 60 minutes were obtained. Two, 4
and 24 hour delayed images were acquired. There was good prompt hepatic
perfusion and uptake of the radiopharmaceutical. In sequential images
and delayed images the activity was noted to accumulate in the paracolic
gutters bilaterally. On delayed images liver uptake was reduced and
there was no activity noted in the bowel, with prominent activity in the
peritoneal cavity indicating activity in the free ascetic fluid
accumulating in the paracolic gutters (Fig. 1). The impression of
biliary leak due to extrahepatic biliary perforation was suggested. This
was further proved by positive bilirubin tested in ascetic fluid
sample.
The patient was sent to laparotomy. About one liter of
ascetic fluid was drained from the abdominal cavity. A tear in the
proximal part of the common bile duct was identified and repaired. A
drain was inserted. Repair of small umbilical hernia and bilateral
inguinal hernias was done. Liver biopsy revealed macrovesicular fat
deposition with normal architecture consistent with moderate fatty
infiltration of the liver. Peritoneal biopsy was consistent with biliary
peritonitis.
The recovery of the patient was smooth during the
first few days post operation. The abdomen was soft and lax, his colour
was clearing. One week post operation, unfortunately, the child started
to deteriorate. He was febrile, distressed, fatigued, blood culture was
positive for Candidal infection. Prompt aggressive antibiotic and
antifungal treatment was started, but he rapidly deteriorated and
cardiopulmonary arrest caused death of the infant.
DiscussionSince
the first report describing spontaneous rupture of bile duct in an
infant, a number of cases have been reported.(1-4) The majority of cases
of this rare cause of biliary ascites occur in the first 5 months of
life;(1,5) few cases are reported in older infants, and it is extremely
rare in adults.(6-8) In adults the usual cause is secondary to
gallstones and almost always extrahepatic.(6,8) There are also reported
cases of spontaneous biliary duct perforation in pregnant females.(7,9)
The presentation may be as an uncommon acute form or a classic subacute
type, and might rarely present with acute abdomen and shock.(10) The
presenting symptoms, clinical features, and early course of the disease
in our patient match those reported earlier. (1,4,11) Typically, an
infant will develop mild jaundice and anorexia after a period of good
health. These symptoms are usually followed by progression to weight
loss and subsequent failure-to-thrive. During the next 3-6 weeks,
intermittent vomiting develops and the stool becomes pale.(10)
Progressive abdominal distention associated with umbilical and inguinal
hernias follow.(4)
Tc99m-DISIDA cholescintigraphy has been found to
be sensitive in demonstrating spontaneous biliary perforation.(4,7,11)
Disofenin has about 88% hepatic excretion. This radiopharmaceutical
enters the anion exchange pathway of bilirubin and share the same
hepatic uptake and excretion pathway. It is taken up by hepatocytes and
not conjugated prior to its excretion. In our patient we report a
distinct technetium disofenin imaging pattern of radioactivity leakage
into the mesenteric folds in the abdomen, and collecting in the
paracolic gutter areas, caused by the perforated extrahepatic bile duct.
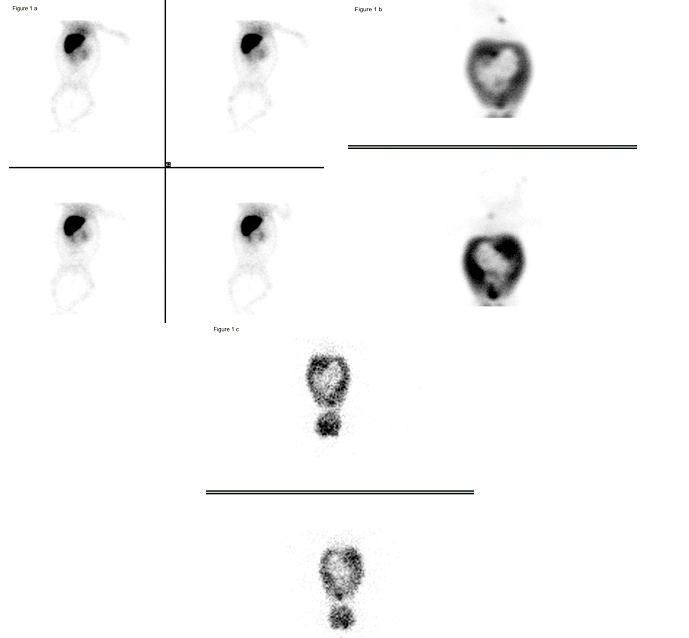
Fig. 1: Sequential Tc disofenin images and delayed 2, 24 hours scans (DISIDA scan):
a) Early flow images show prompt good hepatic uptake of tracer with no evidence of any excretion in the bowel.
b)
Delayed 2 hours images show progressive leakage of radioactivity along
the mesenteric root and mesocolon boundaries into the para-colic
gutters.
c) Filling of gutters filled by ascetic fluid with
radioactivity is noticeable at the periphery of the peritoneal cavity
even in 24 hour images with reduced uptake in the liver.
It
has been postulated that the pathogenesis of spontaneous common duct
perforation in infancy could be due to a localized embryogenic
malformation, congenital thinning (mural weakness) of the anterior bile
duct wall at the junction of the bile and cystic ducts,(1) or ischemia,
or gall stones.(6, 9) No common etiological factors have been
identified for the perforations, but they are almost always located near
the union of the cystic duct to the common bile duct, suggesting that
this junction may be particularly vulnerable to injury or errors in
development.(11)
The Hepatobiliary scan was diagnostic in our
patient. The lack of drainage of radioactivity into the bowel and the
presence of leakage from the common bile duct into the abdomen indicated
perforation. Intraoperative cholecystogram could be used when the size
of the perforation is too small to be identified visually during the
operation, which was not the case in our patient.(12)
The usual
course after surgery and repair of the perforation is recovery and
resolution of the jaundice, normal color of stool and urine and
improvement in the condition of the infant with regard to feeding and
thriving. Later, a repeat hepatobiliary scan shows adequate liver uptake
and biliary drainage to the bowel.(1-4,7,13) Unfortunately, the course
in our reported case was complicated, though transient improvement in
the condition occurred, by Candidal septicemia documented after a week
of operation. Eventually septic shock and death occurred. The long-term
prognosis is usually excellent when the clinicians are aware of this
rare surgically corrected entity, and the problems encountered are
usually due to complications of infection in a poorly thriving infant.
ConclusionSpontaneous
perforation of the common bile duct in infancy is a rare disorder, yet
second to biliary atresia as a cause of surgical jaundice in infancy.
Many lab and diagnostic tools are useful in the diagnosis of this
entity. We emphasize the importance of Tc99m Disofenin (Tc99m- DISIDA)
hepatobiliary scan in establishing the diagnosis of this rare, yet
surgically correctable disease.
References1.
Stringel G, Mercer S. Idiopathic perforation of the biliary tract in infancy. J Pediatr Surg 1983. 18(5): 546-550.
2.
Satish J, Monica J, Dalbir K, Lovesh S. Management of spontaneous
perforation of the bile duct in an infant in a semi-urban setup: a case
report. Malays J Med Sci 2012; 19(1): 73-75.
3.
Pereira ECMV,
Yan J, Asaid M, et al. Conservative management of spontaneous bile
duct perforation in infancy: case report and literature review. J
Pediatr Surg 2012. 47(9): 1757-1759.
4.
Shabib SM, Al-Rabeeahm
A, Rifai A, et al. Spontaneous bile duct perforation associated with
fatty liver in an infant. J Pediatr Gastroenterol Nutr 1996. 23(4):
466-469.
5.
Xanthakos SA, Yazigi MA, Ryckman FC, et al.
Spontaneous perforation of the bile duct in infancy: a rare but
important cause of irritability and abdominal distension. J Pediatr
Gastroenterol Nutr 2003; 36(2): 287-291.
6.
Ticehurst FM, Hutchins RR, Davidson BR. Spontaneous perforation of the bile duct. HPB (Oxford) 2001; 3(4): 285-287.
7.
Talwar N, Manoj A, Bina R, Kumar A, et al. Spontaneous biliary tract
perforations: an unusual cause of peritonitis in pregnancy. Report of
two cases and review of literature. World J Emerg Surg 2006; 1: 21.
8.
Yasar NF, Yasar B, Kebapci M. Spontaneous common bile duct perforation
due to chronic pancreatitis, presenting as a huge cystic retroperitoneal
mass: a case report. Cases J 2009; 2: 6273.
9.
Dabbas, N,
Abdelaziz M, Hamdan K. et al. Gallstone-induced perforation of the
common bile duct in pregnancy. HPB Surg 2008; 2008: 174202.
10.
Lilly JR, Weintraub WH, Altman RP. Spontaneous perforation of the
extrahepatic bile ducts and bile peritonitis in infancy. Surgery 1974;
75(5): 664-673.
11.
Carubelli CM, Abramo TJ. Abdominal distention and shock in an infant. Am J Emerg Med 1999; 17(4): 342-344.
12.
Sahnoun, L, Belghith M, Joun R, et al. Spontaneous perforation of the
extrahepatic bile duct in infancy: report of two cases and literature
review. Eur J Pediatr 2007; 166(2): 173-175.
13.
Murphy JT, Koral
K, Soeken T, et al. Complex spontaneous bile duct perforation: an
alternative approach to standard porta hepatis drainage therapy. J
Pediatr Surg 2013; 48(4): 893-898.