ABSTRACT
Labial adhesions are seen in prepubertal girls. One theory for labial fusion is low prepubertal estrogen levels. Standard treatment for girls with labial fusion has included topical estrogen cream, manual separation, or surgery. Approximately 80% of labial adhesions resolve spontaneously at puberty as estrogen levels begin to increase. We report a 16- years old girl with atypical presentation of labial fusion.
Key words: Labial adhesions, Urine retention.
JRMS June 2016; 23(2):68-70/DOI: 10.12816/0027108
Introduction
Labial adhesions are not uncommon condition and usually seen in infants and pre-pubertal girls due to low pre-pubertal estrogen level. It is usually caused by low estrogen level, recurrent urinary infections, non specific vulvitis and sexual abuse. Pre-pubertal labial adhesions caused by low estrogen, resolve spontaneously when estrogen level increases at puberty.
Case history
A 16-years old sexually inactive, single girl presented to the emergency room in Prince Rashid Military Hospital with a chief complaint of severe supra-pubic pain associated with inability to pass urine over past two days. Gynecological consultation was sought.
Menarche was at the age 14 years. She used to have irregular menses with mild spasmodic dysmenorrhea, and, she had no menses over last 3 months. She has past history of bed wetting at night, dribbling, involuntary passage of urine all. She has no history of frequency or urgency and she hid her complaint from her family as she was embarrased. She has no significant past surgical or medical histories. She has no history of sexual abuse or trauma or similar condition in the past.
Examination:
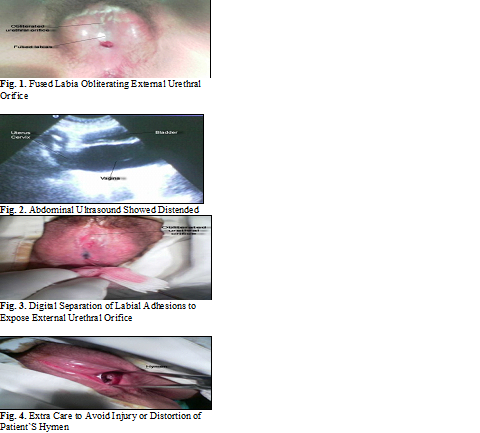
She was distressed, afebrile, stable vital signs, with lower abdominal tenderness. There was no rebound tenderness or supra-pubic swelling. Inspection of the vulva showed fusion of the labia minora obliterating external urethral orifice. Rectal (PR) examination revealed a bulge arising from and involving whole length of the vagina. Fig. 1
Abdominal ultrasound scan showed a grossly distended vagina with a normal uterus and bladder. Fig. 2
Kidney function test, Complete Blood Count (CBC), hormonal profile including plasma estrogen level were normal and urine culture was negative.
Patient was taken to the theatre. Under general anesthesia and complete aseptic condition digital separation of labial adhesions to expose external urethral orifice through the weakest transparent point of labial adhesions was done. About two to three liters of lightly bloody stained fluid were drained. There was no old blood or clots. Labial biopsy was also taken which revealed normal histopathology results with element of inflammatory cells. Fig. 3.
Extra care was taken to avoid injury or distortion of patient`s hymen (Fig. 4) and by end of procedure normal anatomy was restored. Fig. 5. Patient was given a course of antibiotics after taking a swab for culture and sensitivity from lower genital area. 3 days later, culture and sensitivity results were reported as negative and antibiotics were discontinued. Patient was given daily local estrogen cream for two weeks then twice weekly for two weeks and once weekly for one month. Two weeks post-operative, she was seen at Out Patient Clinic (OPC), she was generally well, feeling fine with no urinary symptoms. Examination of the external genitalia revealed normal anatomy. Fig. 6.
Discussion
Labial adhesion is defined as either partial or complete adherence of labial minora. It is an important pediatric and adolescent gynecological problem. Most cases being wrongly interpreted as vaginal agenesis.(1)
Labial adhesions after puberty are rare and usually occur due to chronic inflammation, urinary tract infection, hypoestrogenism or surgical procedures leading to vulval trauma.(1-3) Complete vulval fusion can rarely occur without any evidence of hypoestrogenism.(1)
Recurrence might follow any treatment modality. Surgical approach may be complicated by adhesions and fibrosis; therefore, patients should be evaluated well before starting treatment. Most appropriate method of treatment, is surgical intervention in cases presented with urinary outflow obstruction.(4,5)
Our patient presented with lower abdominal pain and symptoms which were suggestive of acute urinary retention. These symptoms are justified by the clinical finding of complete fusion of the labia (Fig. 1) and consequently the urine was entrapped inside the vagina and this lead to significant vaginal distention (Fig. 2) which apparently was a major cause of her pain. Surgical separation of both labia was done to relieve her acute symptoms. The drained fluid was bloody stained (Fig.3), it mostly represented the entrapped urine and the bloody stained color is explained by the mixture of urine and menstrual blood which also was entrapped inside the vagina. As revealed in the history that she used to have dysmenorrhea, her pain could also be secondary to her coincident menstruation at the same time of the event, the absence of old blood supported this justification. On the other hand, the urinary symptoms of bed wetting, dribbling and continuous spontaneous passage of urine was most likely to the entrapment of urine inside the vagina and as the labial fusion was progressing to complete fusion of the labia this consequently caused vagina distention and pain and inability to pass urine for her past two days. Additionally, she revealed previous history of irregular menstrual period and accordingly this would justify her three months of amenorrhea.

Though complete vulval fusion can rarely occur without any evidence of hypoestrogenism.(1) Despite that the patient was 16 year old and the estrogen level was normal, estrogen cream was used locally for two months.6-8 Estrogen in this case was preferred to betamethasone since the girl was 16 years old and there was no worry regarding side effects of its use.(6-8) The rationale behind using this treatment modality was to prevent possibility of post-surgical fibrosis and as emollient for the vaginal skin. Recurrence rate following topical estrogen is around 10 %. (6)
No definite cause could be found, and, there was no evidence of local inflammation or recurrent urinary tract infection.
Conclusion
Despite this rare presentation, this case showed that labial adhesion should be ruled out in pubertal girls with symptoms suggestive of acute urine retention and considered as part of the differential diagnosis. On the other hand, this rare entity might not be explained with the known risk factors; hypoestrogenic state, recurrent urinary tract infection or vulvovaginitis, genital trauma and sexual abuse. Apparently, the cause of labial fusion in this case could not be identified, and further research is recommended to find out possible other cuases and we recommend to do labial examination in cases with recurrent urinary tract infection.
Refernces
1.Kumar RK, Sonika A, Charu C, Sunesh K, Neena M. (2006): Labial adhesions in pubertal girls. Arch Gynecol Obstet 273: 243–245.
2.Murat Ozekinci, Selcuk Yucel, Cem Sanhal, Munire Erman Akar. (2013): Labial Fusion Causing Coital and Voiding Difficulty in a Young Woman. Advances in Sexual Medicine; 3, 11-13
3.Lambert B (2004): Complete adult vulvar fusion: a case report. J Obstet Gynaecol Can 26(5):501-502.
4.Nurzia MJ, Eickhorst KM, Ankem MK, Barone JG (2003): The surgical treatment of labial adhesions in prepubertal girls. J Pediatr Adolesc Gynecol 16:21-23.
5.Mayoglou L, Dulabon L, Martin Alguacil N, Pfaff D, Schober J. (2009): Success of treatment modalities for labial fusion: A retrospective evaluation of topical and surgical treatments. J Pediatr Adolesc Gynecol 22(4):247-250.
6.Schober J, Dulabon L, Martin-Alguacil N, Kow L, Pfaff D. (2006): Significance of topical estrogens to labial fusion and vaginal introital integrity. J Pediatr Adolesc Gynecol 19(5):337-339.
7.Tebruegge M, Misra I, Nerminathan V. (2007). Is the topical application of estrogen cream an effective intervention in girls suffering from labial adhesions? Arch Dis Child 92(3):268-271.
8.Palla L, De Angelis B, Lucarini L, Spallone D, Palla G, Cervelli V. (2010). A case of labial fusion and urinary pseudo-incontinence in an elderly woman. A surgical treatment and a review. Eur Rev Med Pharmacol Sci 14(5):491-493.