ABSTRACT
Objective: The aim of this study is to describe our experience with cranioplasty plus using implantable biomaterials in repairing calvarial defect, and to highlight its necessity in treating this serious condition.
Methods: The authors retrospectively reviewed and analysed 107 patients who were operated at King Hussein Medical Centre, during the period between Jan. 2004 and Jan 2015, the final study included 84 patients with acquired skull defects of variable size from (3x4cm to 10x13 cm) and location.
Results: cranioplasty using titanium plate or bone cement procedure was technically successful and feasible. Defects were attributable to different pathologies: post depressed fracture 34 cases (40.5%), trauma with decompressive surgery 21 cases (25%), bone tumour 13 (15.5%), infected flap 7 (8.3%), growing skull fracture 9 (10.7%). The procedure achieved successfully the targets of providing protection for the regions of the brain in 85.7% of cases, by reconstructing the harmonic contours of the damaged cranium and give it anaesthetic appearance. However, the observed complication rate was 14.3% overall in our study (n=12), which included three cases of flap infection, sterile wound dehiscence one case, subgalial collection 4 cases, exteriozation of repair material 2 cases, and loosening of repair material 2 cases.
Conclusion: Cranioplasty using Titanium mesh and bone cement was found to be adequate in achieving the wanted goals by re-establishing the integrity of cranium defect, restoring the anatomic and aesthetic deformity, eliminating the risk of traumatic insult to the brain, and relieving the psychological stress of patients and families with a high success rate 85.7%.Cranioplasty is considered simple and safe surgery, however, associated with some complications. Titanium mesh graft repair seems to be easier surgical procedure.
Key words: calvarial defect, cranioplasty, skull defect.
JRMS Dec 2016; 23(4):54-60/DOI:10.12816/0032201
Introduction
Cranioplasty is the term for reconstructive surgery of the calvarial vault, either for acquired defects in the cranial regions or congenital deformity. The aim of this surgical intervention is not only to re-establish the
integrity of the skull defect, moreover, it contributes to the relief of self-esteem drawbacks and increases the social performances.
Defects in the skull usually arise from trauma, infection, tumour ablation or cerebral decompressive procedures.
The history of cranioplasty dates back to 7000 B.C.(1) chaeological findings proved that the use of inorganic materials for cranioplasty had begun before the organic materials.(1) Many different types of materials were used throughout the history of cranioplasty. The evolution of biomedical technology offered new materials to be used by surgeons.
Methods
The authors retrospectively reviewed and analysed 107 patients, operated at King Hussein Medical Centre, over an 11 years period. Demographic data and conditions leading to skull defects, as well as the procedure including the material used to reconstruct these defects, were analysed. Overall 107consecutive patients who underwent surgery for skull defect repair, due to different pathologies from Jan. 2004 to Jan. 2015 at our institute were reviewed. The final stage of the study included 84 patients. 23 patients were excluded after applying the inclusion-exclusion criteria: 15 patients who had missed after the one month follow up or the one-year follow-up, 2 patients were excluded due to small defects and finally 6 patients had no radiological images. 84 patients with acquired skull defect attributable to different pathologies (namely: trauma, infection, tumour ablation or cerebral decompressive procedures) were recruited from the neurosurgical department for this study. All patients were operated on by senior surgeons. Inclusion/ exclusion criteria were: 1) Sizable defect (>2cmx2cm). 2) Patients having radiological images pre-operatively and follow-up images. 3) A minimum clinical and radiologic follow-up of 12 months. While exclusion criteria included: 1) Inadequate documentation of follow-up. 2) Inadequate documentation of radiological follow-up. 3) Small size defects. All consecutive patients admitted and operated at our department and from Jan 2004 till Jan. 2015 were reviewed, follow-up obtained by the investigators. The medical records of patients were reviewed, along radiographic studies that include preoperative and postoperative radiographs images. Average patient age was 26.6 years (4-35 years), and there were 23 females and 61 males. Mean symptom duration before surgery was 2.3 years (9 months – 3.5 years), and patients were observed for an average of 32.3 months (12-85 months).
Demographic and operative data are summarized in Table. I
Operative details
In order to avoid new scarring or necrosis, we re-open the old surgical incision. In all cases, we used the allograft materials; Polymethylmethacrylate (PALACOS® R) and dynamic titanium mesh. Selection of allograft material was subject to many factors: defect size, location, availability and surgeon's experience. The allograft was further shaped as per the defect requirements to a size slightly larger than the defect so that it does not dip into the defect and produce a visible step in the contour. Implant edges were feathered to obtain a smooth contour to the surrounding bone or a high-speed drill may be used to create a shelf at the edge of the craniotomy defect. Additional moulding of the convexity can be achieved by bending the implant. Fixation was performed with titanium mini-plates and screws or polydioxan one sutures (Fig.2). In very large defects, dural hitch sutures are taken between the dura and pericranium/galea which will hold the dura tightly against the implant to prevent accumulation of fluids in the extradural space. All patients received pre-operative antibiotic prophylaxis. The antibiotic was continued for three days as intravenous, then orally seven more days post-operatively. The patients were followed up to observe for any complications or complaints related to the implant.
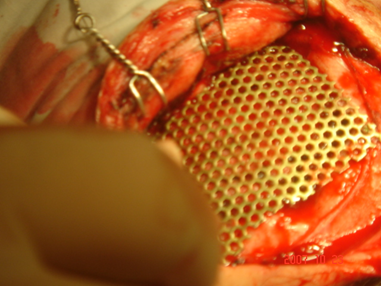
Fig.2:Intraoperative photograph taken during the late phase of the cranioplasty operation of a 14-year-old boy who had skull trauma. Nine months later, he underwent cranioplasty using Titanium mesh.
Fig.3: Intraoperative photograph of a 19-year-old man who had unilateral decompressive craniectomy during acute management of severe closed head injury and who survived with a good neurological outcome. Six months later, he had cranioplasty.
Fig.4:Intraoperative photographs performing cranioplasty using combination of biomaterials. a,b) Intraoperative photograph taken during the early phase of the cranioplasty operation, taken during the late phase of the cranioplasty operation after exposing the skull defect and measuring it's size. c)
Tetanium mesh stripes are placed and secured to the perimetry of the defect with titanium screws.d) The bone cement was placed over, a good shape match has been achieved.
Results
This study conducted at our centre showed that 72.6 % of the patients were males (61/84), mean age 17.4 years (range 4-29). While 23 patients were females 27.4%, mean age 19.6 years (range 7-35). Table. I
Analysis of the causes resulted in the defect revealed that; traumatic skull fractures found in 34 cases (40.5%), decompressive craniotomy surgery 21cases (25%), bone tumour 13 cases (15.5%), infected flap 7 cases (8.3 %), growing skull fracture (10.7%).
Evaluation of the material used in our cases indicated that; Titanium mesh applied in 46 cases, which entail (54.7%) of the whole population, while Polymethylmethacrylate(bone cement) was used in 38 cases (44.3%).
Examination of the Defect size revealed ranges between 12 cm2 and 130 cm.2 though
Mean operation time 63.5 min, in the range of 45 -94 min. The mean hospitalization time was 4.5 days ranging between 4-7 days. However, mean estimated blood loss was 123 cc, ranging between 100-250 cc.
Analysis of the morbidity and mortality also the complications associated with our surgeries showed no mortality from the cranioplasty procedure. However, the success rate was up to85.7% of our operations, as 72 cases had no complications at all. The observed morbidity rate is 14.3% in our study (n=12), which included 3cases of flap infection, sterile wound dehiscence one case, subgalial collection 4 cases, exteriorization of repair material 2 cases, and loosening of repair material 2 cases.Figure.1The patient group received titanium mesh present complications in 7 cases (15.2%), while the patient group, who received bone cement developed complications in 5 cases (13.1%).
Table I: Demographic and operative details
|
Characteristic
|
No. of
Patients
|
|
Male
Female
Type of allograft
Titanium
Methylmethacrylate
Mean length of stay (days)
Mean age (years)
Mean estimated blood loss ( cc)
Mean operation time (min)
|
61
23
46
38
2.5
26.6
123
63.5
|
Fig. 1: Material wise complication encountered
Discussion
Cranioplasty protects the brain, and provides cosmetic results but most importantly, improves the neurological deficits by a decrease of local intracranial pressure and correction of CSF dynamics. Also, the cranioplasty may affect postural blood regulation, cerebrovascular reserve capacity and cerebral glucose metabolism Fig (1).(1)
The vast majority of Patients with traumatic brain injury, stroke or cerebral oedema may undergo decompressive cranio-ectomy with subsequent skull defect. The removal of the bone flap might be associated with a midline shift to the opposite side. These changes are aggravated by the presence of a "syndrome of the sinking skin flap" (SSSF) is the result of the direct transmission of the atmospheric pressure to the intracranial cavity stimulated by CSF hypovolemia.(1-3) Another factor might be the increased incidence of hydrocephalus in patients after decompressive craniotomy, which could be explained by a disturbance of CSF flow around the convexities. Severe CSF hypovolemia can produce herniation syndrome .The definitive and most effective treatment of the SSSF is cranioplasty.(4,5)
Sakamoto et al. described a patient after decompressive craniotomy with the cerebral blood flow (CBF) measured by CT perfusion imaging, which increased to after cranioplasty.(6) Cranial defects determine not only aesthetic but also functional alterations.(5) The so-called "syndrome of the trephined” can be encountered in such patients.(4) The purpose of cranioplasty is to provide protection for the regions of the brain where the cranium is damaged and to reconstruct the harmonic contours of the damaged cranium and give it an aesthetic appearance (Fig. 2). Moreover, the incidence of epilepsy is shown to be decreased after cranioplasty. (7) In our observations the main indications for surgery were the cosmetic issue and addition to the protective role of cranioplasty from further brain damage.
Every time a cranial vault reconstruction is planned, the choice of materials is an important issue. To repair large, complex, skull defects one can choose either to reconstruct the vaults strictly intra-operatively or to prepare a so-called “custom-made cranial implant,” prior to the operation. The disadvantages of intra-operative repair are time-consuming, increasing the risk of infection to the patientand insufficient protection from trauma, often resulting in suboptimal cosmetic results.(8-11) On the other hand, Autografts have the advantage of better toleration and successful incorporation(Fig. 3).In this study the choice of allograft material was subject to many factors: defect size, location, availability and surgeon's experience, no material was preselected.
Contraindications for cranioplasty are the presence of hydrocephalus, infection, and brain swelling. In children below 4 years old, if there is an intact Dura mater, cranium can achieve self-closure. Waiting to perform cranioplasty is important to prevent the development of devitalized autograft or allograft infections. It is generally accepted to wait for 3 to 6 months before reconstructive surgery. In our practice we opt to wait at least 6 months before we perform this procedure.
The cranioplasty itself may result in complications due to brain dysfunction, a risk of fluid collection and subdural or intracerebral hematoma. Chun-Chih Liao et al. recommend that if there is a ventricular-peritoneal shunt, it has to be occluded several days before the cranioplasty to allow the expansion of the depressed area, eliminating the dead space between the bone and the Dura, lessening the risk of hematoma.(12) Moreover, another complication after brain surgery reported by Van Roost, who described a postoperative rapid, malignant, diffuse brain swelling, with a peek at the level of the basal ganglia and thalamus and symmetrical distribution. They called it "pseudo-hypoxic brain swelling" (PBS), a severe and sometimes fatal complication after uneventful intracranial surgery.(13) The clinical picture included signs of brain stem dysfunction in some patients, seizures, or persistent coma after the end of anaesthesia. The CT scans showed hypo-densities which resembled a hypoxic incident (which was ruled out) or severe brain swelling. MRI confirmed the CT changes, SPECT- CBF bilaterally reduced. The hypothesis was that excessive CSF loss via wound drainage and subsequent low ICP possibly triggered PBS, due to a massive negative pressure on the brain. Since they stopped removing the vacuum from the suction bottles and blocking the drains until the patient awakens, no new cases were observed.
Many different types of materials were used throughout the history of cranioplasty. An ideal cranioplasty material must have the following features: a-It must fit the cranial defect and achieve complete closure, b-Radiolucent, c-Resistance to infections d-Not altered with heat, e-Easily amendable and cheap. (14) With the evolving new biomedical technology, new materials are now available to be used by the surgeons. Although autogenous grafts are optimally biocompatible, the risks of donor site complications and increased operating time have limited their use. Acrylic in the form of methyl-methacrylate (polymethylmethacrylate) was first used in human in the first years of the World War II.(15) Methyl methacrylate was widely used after the article of Spence in 1954.(16) With time, aiming to prevent undesired breakings of this material, it was tried to give structural support with steel or titanium meshes. Although commonly used in combination with titanium or wire mesh,(15.16) may be associated with potential complications that include local tissue damage caused by the heat released during the exothermic reaction, release of a toxic monomer that has been associated with local and systemic reactions, and a prohibitively high rate of infection when used adjacent to contaminated sinuses.(17)
Titanium mesh is highly inert, non-toxic, non-antigenic, non-carcinogenic and easily shaped. The tissue biocompatibility of titanium is reflected in the low risk of infection, provided that the surrounding soft tissue is adequate to permit tissue integration.(18) Nevertheless, titanium produces image artefacts on post-operative CT and magnetic resonance imaging studies.
Titanium mesh, depending upon the size of the defect titanium mesh may be used alone or it may be combined with a hydroxyapatite cement for better contour. When used alone, the appropriate mesh is fashioned and cut so that it will extend beyond the actual defect on all sides. It is then fixed in place circumferentially with enough screws to ensure stability. Titanium is hard to shape, but relatively cheaper, bio-acceptable, and radiolucent after mixing with other metals.(19) It also showed good resistance to infection. However, it is not a good option in cases with bad skin viability (e.g.: multiple operations, radiotherapy, etc.).(20) One of the disadvantages of using titanium is the artefact it causes during MRI and CT scans. Acrylic was evolved into the use in cranioplasty. O (21) Acrylic has some advantages above metal substances; it is easy to shape, lighter in weight, radiates less heat, and radiolucent.
Today, alloplastic used most frequently are hydroxyapatite cement, acrylics (especially polymethylmethacrylate).(8-10) The main disadvantage of alloplastic materials is their high susceptibility to infection, but they allow the repair of large defects with no donor site morbidity and smaller costs.(22) Cranioplasty following decompressive craniectomy is associated with a high complication rate, Postoperative complications were recorded in 12 of our patients (14.3 %). Subgalia collection and flap infection were the two most common complications, affecting 4 (33.3 %) and 3 (25 %) patients, respectively, which were in line with the literature. (23,24)
Conclusion
Cranioplasty using Titanium mesh and bone cement was found to be adequate in achieving the wanted goals by re-establishing the integrity of cranium defect, restoring the anatomic and aesthetic deformity, eliminating the risk of traumatic insult to the brain, and relieving the psychological stress of patients and families with a high success rate 85.7%.Cranioplasty considered simple and safe surgery, however, associated with some complication. Titanium mesh graft repair seems to be easier in the surgical procedure.
Limitations: The retrospective study design of the present study. Patients with acquired pathologies were included, while patients with congenital defects were excluded.
Future work: To design one multicentric prospective study, which might include a larger number of patients and have more homogenous features. Also to try to include patients with congenital defects.
Moreover, to analyse different materials and technologies.
References
1.Han PY, et al. "Syndrome of the Sinking Skin Flap" Secondary to the ventriculoperitoneal shunt after craniectomy. J Korean Neurosurg Soc 43 51-53 2008.
2.Sanan A, Haines SJ. Repairing holes in the head: A history of cranioplasty. Neurosurgery 1997; 40:588–603.
3.Durand JL, Renier D, Marchac D. The history of cranioplasty. Ann Chir Plast Esthet 1997; 42:75-83.
4.Yamamura A, et al. Cranioplasty following decompressive craniotomy. Analysis of 300 cases. No Shinkei Geka 5:345-353, 1977.
5.Segal DH, et al. Neurosurgical recovery after cranioplasty. Neurosurgery 34:729-731, 1994.
6.Sakamoto S, et al. CT perfusion imaging in the syndrome of the sinking skin flap before and after cranioplasty. Clin Neurol Neurosurg Sep; 108(6):583-5, 2006.
7.Dujovny M, Aviles A, Agner C, et al. Cranioplasty: cosmetic or therapeutic? Surg Neurol;47:238-41, 1997.
8.Zeilhofer HF, Sader R, Fruh HJ, et al. Möglichkeiten und Indikationsbereiche der Kohlenstoffaserverstärkten Kunststoffe zur Herstellung individueller Implantate für die Rekonstruktion des Gesichts- und Hirnschädels. Biomedizinische Technik ; 42:361-2, 1997.
9.Van Putten MC Jr, Yamada S. Alloplastic cranial implants made from computed tomographic scan-generated casts. J Prosthet Dent 68:103-8,1992.
10.Rotaru AH. Avantajele si dezavantajele utilizarii modelelor tridimensionale medicale. In: Rotaru AH: Reconstructii si Modele Tridimensionale Medicale. Ed. Casa Cartii de Stiinta, Cluj-Napoca.99-100, 2001.
11.Dean D, Min KJ, Bond A. Computer aided design of large-format prefabricated cranial plates. J Craniofac Surg 14:819-32, 2003.
12.Liao, Chun-Chih, et al. Cranioplasty for patients with severe depressed skull bone defect after cerebrospinal fluid shunting. Journal of Clinical Neuroscience Volume 9, Issue 5, 553 – 555, 2002.
13.Dirk Van Roost, et al. Pseudohypoxic brain swelling: a newly defined complication after uneventful brain surgery, probably related to suction drainage. Neurosurgery 53:1315-1327, 2003.
14.Rubin JP, Yaremchuk MJ. Complications and toxicities of implantable biomaterials used in facial reconstructive and aesthetic surgery: a comprehensive review of the literature. Plast Reconstr Surg 100:1336–1353, 1997.
15.Janecka IP. New reconstructive technologies in skull base surgery: role of titanium mesh and porous polyethylene. Arch Otolaryngol Head Neck Surg 126:396–401, 2000.
16.Durham SR, McComb JG, Levy ML. Correction of large (>25 cm2) cranial defects with “reinforced” hydroxyapatite cement: technique and complications. Neurosurgery; 52:842-5, 2003.
17.Couldwell WT, Stillerman CB, Dougherty W. Reconstruction of the skull base and cranium adjacent to sinuses with porous polyethylene implant: preliminary report. Skull Base Surg 7: 57–63, 1997.
18.Blake DP. The use of synthetics in cranioplasty: A clinical review. Mil Med 159:466–9, 1994.
19.Kuttenberger JJ, Hardt N. Long-term results following reconstruction of craniofacial defects with titanium micro-mesh systems. J Craniomaxillofac Surg;29:75–81, 2001.
20.Sanus GZ, Tanriverdi T, Ulu MO, Kafadar AM, Tanriover N, Ozlen F. Use of Cortoss as an alternative material in calvarial defects: The first clinical results in cranioplasty. J Craniofac Surg;19:88–95, 2008.
21.Zoltán B, Gábor T, István H. [Substitution of skull defects with methyl acrylate] Magy Traumatol Orthop Helyreallito Seb;19:259–68, 1976.
22.Moreira-Gonzales A, Jackson IT, Miyawaki T, et al. Clinical outcome in cranioplasty: critical review in long-term follow-up. J Craniofac Surg 2003;14:144-53.
23.Brommeland T, Rydning PN, Pripp AH, Helseth E. Cranioplasty complications and risk factors associated with bone flap resorption. Scandinavian journal of trauma, resuscitation and emergency medicine 2015;23:75.
24.Gooch MR, Gin GE, Kenning TJ, German JW. Complications of cranioplasty following decompressive craniectomy: analysis of 62 cases. Neurosurgical focus 2009;26(6):E9