Methods: From August-1998 through
August-2000, we performed Tc99m -MIBI scintigraphy (MIBI) and neck
ultrasonography in 35 patients who were clinically and biochemically
suspected of having hyperparathyroidism. All patients underwent
surgical neck exploration. Before surgery, blood intact parathyroid
hormone and serum calcium level were measured peripherally. Early and
delayed cervical images of MIBI scans and neck ultrasonography were
interpreted by two radiologists. The findings were compared to
ultrasonography and scintigraphic results. The sensitivity and positive
predictive values of both modalities for localizing the diseased glands
were determined by comparing scan findings with pathological findings,
which were considered the gold standard.
Results: All
resected glands were abnormal. They belonged to 25 patients with a
single adenoma, two patients with ectopic glands, two patients with
double adenomas and 6 patients with hyperplastic parathyroid glands. The
sensitivity and positive predictive values for localizing the diseased
glands in patients with hyperparathyroidism were 91% and 97%,
respectively for Tc 99m MIBI. The values were 74% and 100%,
respectively, for ultrasonography. Tc 99m MIBI sensitivity was higher in
patients with parathyroid adenomas (96%) than that in patients with
parathyroid hyperplasia (67%).
Conclusion: Our results
demonstrate that Tc99m sestamibi scintigraphy is highly accurate in
identifying parathyroid adenoma when performed by an experienced
radiologist. It is helpful in preoperative localization of parathyroid
adenoma in patients with suspected ectopic glands. Nevertheless, because
of the greater accessibility, lower costs and simplicity,
ultrasonography could be used as a screening modality for parathyroid
adenoma localization.
Key words: Scintigraphy, Technetium99m sestamibi, Ultrasonography, Parathyroid adenoma.
JRMS June 2003; 10(1): 6-11
Introduction
Primary hyperparathyroidism (HPT) is a common condition mostly due to either a solitary parathyroid adenoma or, less commonly, parathyroid hyperplasia, for which the only effective treatment is surgery (1).
Various methods have been proposed for the preoperative localization of parathyroid adenoma or hyperplasia, in order to simplify and shorten the surgical procedure. Some of these methods are not invasive, such as ultrasonography, computerized tomography, nuclear magnetic resonance and isotope scanning (2). The sensitivity of the majority of them is too low to justify their routine use (3).
Radioisotope techniques, like other imaging procedures, have been used for the detection of parathyroid glands. Dual radionuclide imaging using a combination of Thallium-201 (201Tl) with either Technetium Pertechnitate-99m (Tc99m O4) or Iodine-123 (123I) is recognized as a useful procedure in the preoperative localization of abnormal parathyroid glands (4,5). In recent years, Technetium-99m-sestamibi (Tc99m -MIBI) scintigraphy, which has been used as a cardiac imaging for many years (6,7), was introduced for the localization of abnormal parathyroid glands as an alternative method to 201Tl/ Tc99m subtraction scintigraphy (8).
The usefulness of Technetium (Tc99m -MIBI) in patients with hyperparathyroidism has been evaluated extensively. A comparison with many procedures such as 201TI/99m Tc-subtraction scintigraphy, F-18 Fluorodeoxyglucose (18F-FDG) with positron emission tomography (PET), ultrasonography (US), computerized tomography (CT) scan and magnatic resonance imaging (MRI) has been made (2,9).
A simplified approach to parathyroid scintigraphy using a double-phase procedure after intravenous injection of MIBI had been proposed. After the injection (first or thyroid phase), MIBI concentrates in the thyroid and parathyroid tissues; in the second or parathyroid phase, its activity decreases in the normal thyroid while residual uptake persists in the presence of parathyroid adenomas or hyperactive tissue. The results will be extracted from visual comparison of early (15-minutes) and late (120-minutes) images (10,11).
Our aim in this study was to establish the effectiveness of double-phase MIBI scintigraphy in the anatomical localization of abnormal parathyroid glands in patients with primary hyperparathyroidism and to compare this method with high-resolution ultrasonography.
Methods
This study was performed at King Hussein Medical Center, from August 1998 to August 2000. We studied 35 patients, 21 women and 14 men with a mean age of 54.5 years (range, 32-67). They presented with clinical symptoms and biochemical parameters of primary hyperparathyroidism. In all patients, ultrasound of the neck and scintigraphy with intravenous Tc99m -MIBI, 20 mCi per 70 kg of body weight, were performed. Serum calcium and intact parathyroid hormone (iPTH) levels were measured. All patients underwent parathyroidectomy with histopathological examination for the entire gland.
a. Tc99m -
MIBI parathyroid scintigraphy The patients were injected I.V. with 740 Mbq (20 mCi) of Tc99m -sestamibi.
Anterior views of the neck and the upper thorax were taken with the patient in the supine position. Images were obtained at 15 min (initial or thyroid phase) and 2 hours (delayed or parathyroid phase) after the administration of the radiotracer (10). A digital gamma (GE Millenium) camera with a low energy, high
resolution, and parallel-hole collimator was used.
The images were visually evaluated for abnormal focal areas of increased tracer localization in the neck and mediastinum. We defined a 'focal positive study' when we observed one or more clearly defined areas of abnormal uptake in relation to the surrounding tissue, placed in the thyroid area, visible in early images and persisting on late images (washout). The study was 'negative' when it did not correspond to the previous situation.
b. Neck ultrasonographyThe ultrasonography study was performed with a 7.5 MHz duplex-Doppler (color) transducer, with the patient in the supine position with hyperextension of the neck. The ultrasound examination (axial and longitudinal scans) including the thyroid region and the areas above and below the thyroid gland was used to identify the parathyroid glands even in an atypical location. Normal parathyroid glands are not visualized with the equipment currently available. When pathological glands were observed, the echostructure (hypoechoic, homogeneous, inhomogeneous, calcifications), size (longitudinal and anteroposterior diameters), and vascularity (hypovascular, normal or hypervascular) were assessed.
c. Surgical evaluationAll patients underwent bilateral surgical neck exploration. Criteria for surgery were independent of the MIBI and ultrasonography results. The surgeon decided which gland to remove according to the palpation of a suspicious gland.
d. Histopathological and laboratory evaluationHistological examination of enlarged parathyroid glands was performed in all the glands. Intact parathyroid hormone and calcium levels from peripheral blood were measured from one blood sample.
e. Statistical analysis Technetium 99m sestamibi scintigraphy and ultra-sound were performed on the 35 patients with hyperparathyroidism, and their accuracy was determined on the basis of surgical and histopathology of parathyroid glands. Scan results were correlated with serum calcium and iPTH levels, and with associated thyroid abnormalities. Sensitivity and positive predictive values were calculated by the standard methods.
A statistical analysis was performed using the student's t-test. A P value ≤ 0.5 was considered the level of significance.
Results
a. Scintigraphic ResultsMIBI scintigraphy was positive (Fig. 1) in thirty two
patients (Table I). Among them, two patients with two foci of increased tracer uptake in the neck were consistent with two parathyroid adenomas and another two patients with a focus of increased tracer uptake in the mediastinum (Fig 2) were consistent with ectopic parathyroid gland. In one patient, the focus of tracer uptake in the neck was in the contralateral side to the abnormal removed gland. This was the only false positive case in a patient with concomitant multinodular disease of the thyroid.
b. Echographic Results High-resolution ultrasound was positive in 26 patients with hyperparathyroidism (Fig 3). One of the patients with a double adenoma had a negative ultrasound. Ultrasound examination was negative in nine patients.
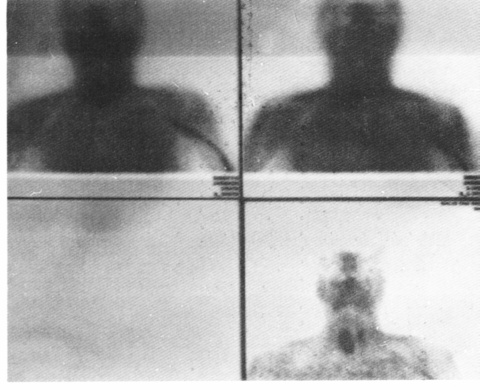
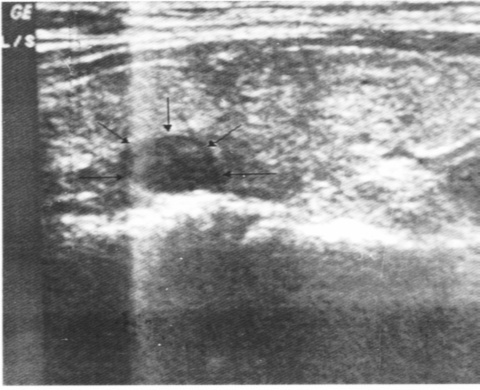
Fig 3. Ultrasonography showing a well-defined hypoechoic lesion posterior to the thyroid gland representing a para thyroid adenoma.
c. Operative FindingsThe surgeon tried to identify all enlarged parathyroid glands. Surgery revealed 25 solitary parathyroid adenomas, 2 parathyroid adenomas in two patients; and 6 patients with hyperplastic parathyroid glands. Two ectopic lesions removed from the mediastinum were sestamibi-positive and, in this case, the scintigraphic result was a direct indication of the need for mediastinal surgery.
d. Histopathological and Laboratory ResultsIn all cases an abnormal parathyroid gland was found and hyperparathyroidism was due to adenomatous disease or hyperplasia.
Histological diagnosis of the excised parathyroid gland showed a solitary adenoma in 25 patients (71%), double adenoma in two (6%) and multiple hyperplastic glands in 6 (17%). Associated thyroid disease was present in 2 (6 %) patients.
The mean adjusted PTH level for the whole group was 373 ± 124 pg/ml (range, 89 to 578). (Normal range: 12-72 pg/ml)
The mean serum level of calcium for the whole group was 10.9 ± 0.7 mg/dL (range, 8.6 to 13.2 mg/dL). (Normal range: 8.5-10.4 mg/dL).
e. Technical Aspects Ultrasonography is available in all of the radiology departments of the Royal Medical Services hospitals. The examination could be performed immediately upon request or in one week. While for MIBI scan, it was only available at Al- Hussein Hospital upon prior arrangement.
The cost of ultrasound ranges from 10-30 Jordan Dinars (JD) per examination while for MIBI, it ranges from 70-150 JD per exam.
f. Data AnalysisThe interpretation of the parathyroid images was relatively easy; however, the depth of the adenoma could not be predicted, based on the scan alone. 99m Tc-MIBI radionuclides scan was positive in 32 patients and negative in 3 patients. Apart from one case, anatomical location disclosed by positive scintigraphy was concordant with the surgical findings.
The Tc99m -MIBI radionuclide scan was positive in 23 out of 25 patients with a cervical solitary adenoma. Two patients with a double adenoma had a localization image consistent with two enlarged glands. Two other patients with the ectopic adenomas were identified preoperatively by Tc99m sestamibi imaging, which contributed significantly to the surgical approach. Four patients out of six patients with parathyroid hyperplasia had Tc-99m-sestamibi imaging consistent with diffuse hyperplasia, although delineation of individual enlarged glands was not possible. There were two patients that had associated nodular thyroid disease, leading to one false positive result.
Overall sensitivity and positive predictive values for Tc-MIBI scintigraphy were 91% and 97%, respectively, increasing to 96% and 97% in the patients with adenoma. The sensitivity and positive predictive values for patients with parathyroid hyperplasia were 74% and 100%, respectively.
There were no observable differences in sensitivity between the upper and the lower pathological gland groups.
Ultrasonography was positive in 26 patients and negative in 9 patients. It was positive in 22 patients with solitary adenomas, in one of the patients with two adenomas and in 3 patients with hyperplastic glands. The ultrasonography was negative in 3 patients with solitary adenomas, in two patients with ectopic glands, and in 3 patients with hyperplasia. Overall sensitivity and positive predictive values of sonography were 74% and 100%, respectively.
The sensitivity of MIBI (91%) was greater than that of ultrasonography (74%), with a very close positive predictive value (97% and 100%, respectively). The diagnostic sensitivities for detection of parathyroid adenomas was 96% for dual-phase sestamibi and 79% for ultrasonography, which were significantly different (p ≤ 0.05). In two cases, MIBI scintigraphy revealed the presence of ectopic adenomas not detected by ultrasonography.
Both imaging modalities, dual-phase sestamibi and ultrasonography, correctly identified 28 of 29 (97%) histologically confirmed adenomas, and 4 confirmed hyperplastic glands; with concordant results in 26 patients and discordant results in 9 patients. MIBI and ultrasonography were not negative in 3 patients. The overall sensitivity and positive predictive values for both imaging procedures, when they were considered as one test, were 91 and 100%.
Preoperative mean total calcium was 10.6 + 0.8 mg/dL (range, 8.5 to 13.3 mg/dL) and (iPTH) was 373 + 124 pg/ml (range, 91 to 542) for patients with adenomas.
For patients with hyperplasia, the mean total calcium and iPTH were 10.7 + 0.6 mg/dL (range, 8.6-13.0), and 365 + 118 (range, 95 to 501) pg/ml, respectively.
The mean total calcium and intact parathyroid hormone were 10.9 mg/dL (range, 10-14.4) and 332 pg/ml (range, 88.1-551), respectively for patients with positive scan and 11.2 mg/dL (range, 10-15) and 153 pg/ml (range, 83.1-551) for patients with negative scan.
Discussion
The inability to predict the location and number of diseased parathyroid glands in patients with primary hyperparathyroidism, has precluded the wide acceptance of bilateral neck exploration for primary hyperparathyroidism. Intraoperative identification of abnormal parathyroid glands is challenging and may require extensive dissection of the neck and mediastinum. The experience of the surgeon and precise localization of parathyroid glands determine the success rate of surgery for HPT. Ectopic glands and anatomic variations, not diagnosed by standard methods, are causes of surgical failure. The appropriate identification of all the pathological tissue is important in order to avoid future recurrence and surgical interventions (1,12).
The preoperative localization of the hyperfunctioning glands is still a subject of controversy, and many parathyroid surgeons question the necessity of imaging before surgical exploration as currently available techniques do not provide any better results than an expert surgeon does (3,13).
Various non-invasive methods have been proposed for the preoperative localization of parathyroid adenoma such as US, CT, MRI and isotope scanning (2). The sensitivity of the majority of them is too low to justify their routine use (3). When these methods fail, some invasive procedures can be used. Some workers observed that measuring iPTH in both internal jugular veins separately could predict accurately in which side of the neck the hyperfunctioning tissue is located, however, it is an invasive technique with possible complications, and its routine use is not recommended (14).
Radioisotope techniques, like other imaging procedures, have been used for the detection of parathyroid glands. The usefulness of a cationic complex of isoalkilonitriles (15) of Technetium (Tc99m -MIBI) has been described. MIBI is a lipophilic radiotracer that concentrates in the cells and inside the mitochondria through active transport and passive diffusion, depending on the respective membrane potential difference. In metabolically hyperactive cells, such as malignant and adenomatous cells (16-20), the number of mitochondria is increased and, according to the degree of cellular activity, different MIBI uptake patterns can be observed (21,22).
Tc99m -MIBI was evaluated in the assessment of many tumors and malignancies (16-20), such as breast cancer (23,24). Uptake by benign tumors was not the rule, but primary parathyroid adenomas showed a good incorporation of the radiomarker (9,25,26). It allows a morphological study of the parathyroid gland including the localization of ectopic glands.
Although there was a wide range of reported sensitivity (57%-95%) and positive predictive value (82%-100%), this technique seems to be sensitive enough to detect parathyroid adenomas (9-11,25-27).
In our study, the overall sensitivity of double-phase Tc99m -sestamibi scintigraphy was 91% versus 74% for ultrasonography (P ≤ 0.05). For the patients with adenoma, the detection sensitivity for Tc99m -sestamibi scintigraphy was 96% versus 79% for ultrasonography (P ≤ 0.05) while inpatients with hyperplasia the detection efficiency was 67% versus 50% for ultrasonography (P > 0.05). There was one false positive scan with Tc99m -sestamibi scintigraphy in a patient with concomitant multinodular thyroid disease. However, difficulties associated with thyroid nodule call for complementary thyroid scanning.
The detection rate of sonography was significantly inferior to that of Tc-MIBI. Both imaging modalities had lower sensitivities in the setting of hyperplastic parathyroid disease. If both imaging studies were considered as a single test, sensitivity for imaging patients with histologically confirmed hyperparathyroidism would be 91% (p ≤ 0.05).
Two cases of ectopic adenomas were identified preoperatively by sestamibi but not ultrasonography. This contributed significantly to the surgical approach. When MIBI scan shows a single gland, the risk of missing multiple localization appears to be low.
No correlation was found between preoperative serum concentrations of calcium and iPTH on the one hand, and sensitivity of MIBI-scintigraphy on the other (p>0.05). Again, we did not find any relation between the sensitivity of sestamibi and the location of the parathyroid gland, neither between the upper and lower nor between the right and the left side (p>0.05).
Identification of hyper functioning parathyroid tissue prior to surgery indicates that when an imaging procedure is required, Tc99m -MIBI may be of great help in the management of hyperparathyroidism, especially in cases of parathyroid adenoma, including those with aberrant location. These advantages appear to be great enough to justify systematic use of MIBI scan prior to surgery.
Nevertheless, because of its greater accessibility, lower costs, and simplicity ultrasonography may be used as a screening modality for parathyroid adenoma localization prior to surgery, and Tc99m -MIBI scintigraphy could be used as the second step when sonography is negative. This approach could be of practical value in view of scarce sources in financing the other more expensive one.
Conclusion
Similar to previous reports, our results confirm that MIBI scintigraphy is a reliable and useful method to locate hyperfunctioning parathyroid tissue. It is more sensitive and accurate than ultrasonography for the preoperative localization of abnormal parathyroid glands, and in contrast to ultrasonography its sensitivity does not decrease if a parathyroid adenoma is located ectopically. Nevertheless, because of the greater accessibility, lower costs and its simplicity ultrasonography could be used as a screening modality for parathyroid adenoma localization.
The combination of Tc99m MIBI scintigraphy and US performed by well-trained operators, and up-to-date instruments could improve the diagnostic accuracy.
This test may be useful in patients with post-operative recurrence of hyperparathyroidism, which will be assessed in another study.
As a future step; the use of pinhole collimator could improve the detection rate of small parathyroid adenomas, however, this needs further evaluation.
Table I: The results of MIBI scan.
|
|
|
Positive
|
Negative
|
|
32
|
3
|
|
Hyperplasia
|
Single adenoma
|
Double adenoma
|
Ectopic
adenoma
|
False positive
|
|
|
4
|
23
|
2
|
2
|
1
|
|
References
1.
Tibblin S, Bondeson AG, Bondeson L et al. Surgical strategy in hyperparathyroidism due to solitary adenoma Ann Surg 1984; 200: 776-784.
2.
Wada A, Sugihara M, Sugimura K, Kuroda H. Magnetic resonance imaging (MRI) and Technetium-99m-methoxyisonitrile (MIBI) scintigraphy to evaluate the abnormal parathyroid gland and PET efficacy for secondary hyperparathyroidism. Radiat Med 1999; 17(4): 275-282.
3.
Coakley AJ. Parathyroid imaging. Nucl Med Commun 1995; 15: 522-533.
4.
Fine EJ. Parathyroid imaging: its current status and future role. Semin Nucl Med 1987; 17:350-9.
5.
Young AE, Gaunt JI, Croft DN, Collins REC. Location of parathyroid adenomas by Thallium-201 and Technetium-99m subtraction scanning. BMJ 1983; 286: 1384-1386.
6.
Lee DS, Cheon GJ. Reproducibility of assessment of myocardial function using gated Tc 99m MIBI SPECT and quantitative software. Nucl Med Commun 2000; 21: 1127-1134.
7.
Saeed MA, Saeed S. Enhanced Tc 99m MIBI SPECT detection of hibernating myocardium following the use of sub-lingual nitroglycerine. Nucl Med Commun 2001; 22: 65-72.
8.
Coakley AJ, Kettle AG, Wells CP, et al. Tc99m -sestamibi: A new agent for parathyroid imaging. Nucl Med Commun 1989; 10: 791-794.
9.
Casara D, Rubello D. Tc 99m MIBI radio-guided minimally invasive parathyroid surgery planned on the basis of a preoperative combined Tc-99m-pertechnetate/ Tc 99m MIBI and ultrasound imaging protocol. Eur J Nucl Med 2000; 27: 1300-1304.
10.
Torregrosa JV, Palomar MR, Pons F. Has double-phase scintigraphy usefulness in the diagnosis of hyperparathyroidism?. Nephrol Dial transplant 1998; 13: 37-40.
11.
Piga M, Bolasco P, Satta L. Double-phase parathyroid Tc 99m MIBI scintigraphy to identify functional autonomy in secondary hyperparathyroidism. J Nucl Med 1996; 37: 565-569.
12.
Davis RK, Hoffman J, Dart D, et al. Unilateral parathyroidectomy. Otolaryngol Head Neck Surg 1990; 102: 635-638.
13.
Van’t Hoff W, Ballardie FW, Bicknell EJ. Primary hyperparathyroidism: The case for medical management. Br Med J 1983; 287: 1605-1608.
14.
McMillan NC, Smith L, McKellar NJ, et al. The localization of parathyroid tumors: A comparison of CT scan with cervical vein hormone assay. Scot Med J 1983; 28: 153-156.
15.
Reilly RM, So M, Polihronis J. Rapid quality control of Tc-99m-sestamibi. Nucl Med Commun 1992; 13: 664-666.
16.
Caner B, Kitapcl M, Unlu M. Technetium-99m-MIBI uptake in benign and malignant bone lesions: A comparison study with Technetium-99m-MDP. J Nucl Med 1992; 33: 319-324.
17. Kanmaz B, Erdil TY, Sayman HB. The role of Tc-99m-tetrofosmin in the evaluation of thyroid nodules. Nucl Med Commun 2000; 21: 333-339.
18. Adalet I, Kocak M. Determination of medullary thyroid carcinoma metastases by Tl-201, Tc-99m-(V) DMSA, Tc 99m MIBI and Tc099m-tetrofosmin. Nucl Med Commun 1999; 20: 353-359.
19. Jong MD, Bernard BF, Breeman WAP. Comparison of uptake of Tc 99m MIBI, Tc-99m-tetrofosmin and Tc-99m-Q12 into human breast cancer cell lines. Eur J Nucl Med 1996; 23: 1361-1366.
20. Koukouraki S, Damilakis J. Giatromanolaki A. Functional imaging of tumors with Tc-99m-sestamibi pinhole scintigraphy. Nucl Med Commun, 1996; 17: 943-951.
21. Piga M, Bolasco P, Satta L, et al. Double-phase parathyroid technetium-99m-MIBI scintigraphy to identify functional autonomy in secondary hyperparathyroidism. J Nucl Med 1996; 37: 565-569.
22. Chin ML, Kronange JF, Piwinca WD. Effect of mitochondrial and plasma membrane potentials on accumulation of hexakis (2 methoxyisobutil isonitrile) technetium in cultured mouse fibroblasts. J Nucl Med 1990; 31: 1646-1653
23. Palmedo H, Biersack HJ. Scintigraphy with Tc 99m MIBI: Results of a prospective European multicenter study. Eur J Nucl Med (1998) 25: 375-385.
24. Horne T, Pappo I. Tc 99m MIBI scintimammography for the detection of breast malignancies: Contribution of the count ratio to specificity. Nucl Med Commun, 1999; 20: 511-516.
25. Ambrosoni P, Heuguerot C, Olaizola I. Can we use Tc 99m MIBI in functional studies of the parathyroid gland? Nephrol Dial transplant, 1998; 13: 33-36.
26. Moka D, Voth E, Dietlein M. Preoperative localization of parathyroid adenomas using Tc 99m MIBI scintigraphy. AJM 2000; 108: 733-736.
27. Doherty MJ, Kettle AG, Wells P. Parathyroid with Tc-99m-sestamibi: Preoperative localization and tissue uptake studies. J Nucl Med 1992; 33: 313-318.