ABSTRACT
Objectives: To investigate clinically and radiographically the number of roots and root canals in the maxillary first premolars in a group of Jordanian population using magnifying loupes while carrying out routine endodontic practice.
Methods: A total of 176 patients 87 female (49.4%) and 89 male (50.6%) received root canal treatment of maxillary first premolar at King Hussein Medical Centre from January 2012 till January 2015. The age of the patients was ranging from 18 to 60 years. The teeth included in the study were both clinically and radiographically examined for the number of root canals using sharp endodontic explorer and magnifying loupes. Diagnostic preoperative radiographs were taken for evaluation. Two radiographs in two planes (parallel and 20ᵒ- 40ᵒ horizontal angle cone shift) were taken during routine endodontic treatment for these teeth. The number of roots and root canals in the maxillary first premolars was recorded.
Results: Out of the total of 176 maxillary first premolars 56 teeth had one root (31.8%), 118 teeth had two roots (67.0%) and two teeth had three roots (1.1%) . Based on Vertucci's classification of root canal morphology: one tooth (0.6%) had type I canal configuration (one canal), 17 teeth (9.7%) had type II (two canals with shared apical foramen), 156 teeth (88.6%) had type IV (two canals with separate apical foramen) and two teeth (1.1%) had type VIII ( three canals with separate apical foramina). The percentage of two canals (type II and IV) is 98.3%.
Conclusion: The percentage of two canals (either with shared or separate apical foramina) is very high in the maxillary first premolars in Jordanian population. Inspection should be done for the presence of second canal whenever endodontic treatment is planned for this tooth.
Key words: Anatomic variation, Cone shift, Maxillary first premolars, Root canals, Vertucci's classification.
JRMS Dec 2017; 24(3): 19-24 / DOI:10.12816/0042333
Introduction
A good knowledge of the anatomy of the tooth and its root canal system is essential for the success of root canal treatment.1 The main goal of root canal treatment is a good cleaning and shaping of all root canals and filling of these canals with an inert filling material.(1,2) The inadequate knowledge of the anatomy of the root canal system can lead to incomplete biomechanical instrumentation and failure of endodontic treatment. (3) It is well known that tooth anatomy varies according to racial origin. . (2,3,4) Therefore it is very important to be familiar with characteristic features of the tooth anatomy and its variations in different racial groups since such knowledge can enhance the success of endodontic treatment. (4) Review of the literature showed a high variability in the anatomy of the root canal system of the maxillary first premolar. (5-26) The incidence of one root ranges from 17.9% - 66%; while the incidence of two roots ranges from 33.3% - 80.9%. The occurrence of three roots is scarce and ranges from 0 to 4% .The occurrence of one canal varies between 1.3% - 48.8% while that of two canals ranges from 50.6% to 96.1%. (5-26) The external and internal anatomy of maxillary first premolars of Jordanian population has only been studied by Awawdeh et al. (5) They examined 600 extracted first maxillary premolars from North Jordan clinics using clearing technique. The aim of our study was to investigate clinically and radiographically the number of roots and root canals in the maxillary first premolars in a group of Jordanian population in routine endodontic practice.
Methods
A total of 176 patients 87 females (49.4%) and 89 males (50.6%) received root canal treatment of maxillary first premolars in the endodontic clinic at King Hussein Medical Centre from January 2012 till January 2015. The age of the patients was ranging from 18 to 60 years. The teeth included in the study were both clinically and radiographically examined for the number of root canals. Diagnostic preoperative radiographs were taken for evaluation. The teeth included in the study were those that required nonsurgical endodontic treatment. The included teeth were free of root resorption, had no calcifications or open apices. No retreatment cases were included in the study. Routine endodontic procedures were undertaken: Local anesthesia administration, rubber dam isolation, adequate oval access cavity was opened between the cusp tips, being wider bucco-palatally. 2.5% sodium hypochlorite irrigation was used. Examination of the floor of the pulp chamber to locate canals orifices is done using sharp endodontic explorer and 3.5 high resolution magnification loupes ( Keeler Inc. UK). Two periapical radiographs in two angles were taken (parallel and 20ᵒ- 40ᵒ horizontal angle cone shift) for evaluation of the number of roots and root canals as well as for confirmation of the working length after inserting size 15,20 or 25 K files in the canals. These radiographs were evaluated using x ray viewer. The teeth included were both clinically and radiographically examined by two specialists with more than 10 years of experience in endodontics. The number of roots and root canals in the maxillary first premolars was recorded. The number of roots was recorded as one root, two roots (whether they are completely or partially separate or they are fused) or three roots. The number of canals was classified according to Vertucci classification (7) as shown in Figure 1.
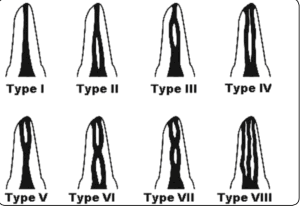
Figure 1: Vertucci classification of the root canal system (7).
Results
Out of the total of 176 maxillary first premolars 56 teeth had one root (31.8%), 118 teeth had two fused or separate roots (67.0%) and two teeth had three roots (1.1%) . Based on Vertucci's classification of root canal morphology: one tooth (0.6%) had type I canal configuration (one canal), 17 teeth (9.7%) had type II (two canals with shared apical foramen), 156 teeth (88.6%) had type IV (two canals with separate apical foramen) and two teeth (1.1%) had type VIII ( three canals with separate apical foramina). The incidence of two canals (type II and IV) is 98.3%. Out of the 87 females 32.1% of the maxillary first premolar had one root, 66,7% had two roots and 1.2% had three roots. Regarding root canal morphology 1.2% of the female’s maxillary first premolar had type I, 12.6% had type II, 85.1% had type IV and 1.2% had type VIII. Out of the 89 males 31.5% of the maxillary first premolar had one root, 67.4% had two roots and 1.1% had three roots. Regarding root canal morphology none of the male’s maxillary first premolars had type I, 6.7% had type II, 92.1% had type IV and 1.1% had type VIII.
Discussion
Knowledge of root canal morphology and its frequent variations is a basic requirement for endodontic success. (1,2) Failure of the dentist to detect all the canals present in the tooth may lead to failure of root canal treatment.(3) The number of roots and canals of the maxillary first premolar in the literature shows a wide variation. (5-26) The differences may be due to the study design (clinical versus laboratory) method of canal identification (radiographic examination, root sectioning, canal staining and root clearing, examination with SEM or CBCT cone-beam computed tomography techniques), classification method, sample size or due to racial variation. (1,2) Clinically, diagnostic preoperative radiograph and its careful examination is necessary before starting root canal treatment. (27) Additional periapical radiographs with cone shift angulations will show more adequate information about root canal system. Martinez-Lozano et al. (28) found that by varying the horizontal angle of x-ray tube 20ᵒ- 40ᵒ, the number of root canals observed in maxillary first and second premolars coincided with the actual number of canals present. Sardar et al reported that the second canal of maxillary second premolars became obvious in 78% of cases when cone shift radiographic technique was used. (29) In the present study one preoperative radiograph was taken . Another two radiographs (one at right angle and the other with 20ᵒ- 40ᵒ horizontal angle cone shift) were taken to explore the number of roots and root canals and to take the working length of the canals during root canal treatment. Other diagnostic measures that help in locating root canal orifices include adequate access and modification of the outline of the access cavity, exploration of the tooth's interior and appropriate magnification and illumination. (2,3) In this study adequate oval access cavity was opened between the cusp tips, being wider bucco-palatally. Endodontic explorer and magnifying loupes were used to help in examination of the pulp chamber floor and to identify and locate the orifices of the root canals. Using dental loupes and dental operating microscope (DOM) provides the endodontist with good lighting and magnification which improves the ability to locate extra canals. (30) Ahmad et al (31) reviewed 92 studies done on the maxillary first premolars for different populations and calculated the averages for certain internal and external morphologic features. They reported that the majority of maxillary first premolars had two roots (56.6%) or one root (41.7%) and the majority had two root canals (86.6%) with type IV being the most common canal type (64.8%). Table I compares the results of Jordanian population with other populations for the number of roots of maxillary first premolars. In the present study the classification of the number of roots was challenging as it was difficult to distinguish radiographically between single wide root and two fused roots. In spite of this, the percentage of the number of roots in maxillary first premolar was close to that of Awwawdeh et al in vitro study that was done on extracted teeth of Jordanian population. (5) In our study 31.8% of the maxillary first premolar had one root. This is lower than those reported for Mexicans, (6) North Americans, (7) Chinese, (8) Kuwaiti, (10) and Indian population. (19) An interesting observation in our study is that the majority of maxillary first premolars had two roots and one canal in each root (67%). This percentage is higher than most earlier studies that were done around the world ; its higher than those reported for Mexicans, (6) North Americans, (7) Chinese, (8) Brazilians, (9) Kuwaiti, (10) Singaporeans, (11) and Indians. (19) The incidence of three roots in the present study was only 1.1%. This low percentage is in consistent with previous studies where the incidence varies between 0- 4%. (5- 20) Although the presence of three roots is rare in maxillary first premolar, this must be kept in mind during negotiation of canals during root canal treatment. Premolars with three roots will also cause difficulty in tooth extraction or movement during orthodontic treatment. Beside the number of roots, the number of root canals in the maxillary first premolars is also studied which is of more clinical significance for endodontists. Table II compares the results of Jordanian population with other populations for the number of root canals in maxillary first premolars. In our study only 0.6% of teeth had one root canal type I. A surprising observation is that our results are much lower than most studies for other populations all over the world. (6-12,14-23) The most common root canal configuration in our study was type IV (88.6%), followed by type II (9.7%). In the present study on Jordanian population the incidence of two canals whether they are completely separate or fused apically is very high (98.3%). This percentage is slightly higher than those of Turkish,(16, 21) Saudi (18, 25) and Spanish population (13) but much higher than those for Mexicans, (6) North Americans, (7) Chinese, (8) Brazilians, (9) Kuwaiti, (10) Singaporeans, (11) and Indians. (19) Our results for the number of roots and root canals are very close to Awwawdeh et al, results. Therefore, the observed variation noted in our studies could be a true variation in Jordanian population. The incidence of three canals (type VIII) in the present study was only 1.1%. This low percentage lies in the range of previous studies where the incidence varies between 0- 5%. (5-20) Although the incidence of three canals is rare, it should be kept in mind during root canal treatment of this tooth. Three canals should be suspected clinically when the pulp chamber appears to deviate from normal configuration and does not aligned in its expected bucco-palatal relationship. (32,33) If the pulp chamber seems to be either triangular in shape or too large in a mesiodistal direction, more than one root canal should be suspected. (32,33)
Table 1: Percentages of number of roots in maxillary first premolars of different population.
|
3
Roots
|
2 Roots
|
1 Root
|
Number
of
teeth
|
Population
|
Study
|
|
2.4
|
54.6
|
43.0
|
259
|
Mexican
|
Pineda and Kuttler (1972) 6
|
|
4.0
|
56.5
|
39.5
|
400
|
American
|
Vertucci (1984) 7
|
|
0
|
40.0
|
60.0
|
100
|
Chinese
|
Walker (1987) 8
|
|
2.5
|
41.7
|
55.8
|
240
|
Brazilian
|
Pécora et al (1991) 9
|
|
3.8
|
53.2
|
43.0
|
79
|
Kuwaiti
|
Zaatar et al (1997) 10
|
|
0
|
50.6
|
49.4
|
957
|
Singaporean
|
Loh (1998) 11
|
|
1.3
|
61.3
|
37.3
|
300
|
Turkish
|
Kartal et al (1998) 12
|
|
3.3
|
56.7
|
40.0
|
150
|
Spanish
|
Chaparro, et al (1999) 13
|
|
9.2
|
75.3
|
15.5
|
142
|
Polish
|
Lipski et al (2005) 14
|
|
1.2
|
80.9
|
17.9
|
246
|
Saudi
|
Atieh (2008) 15
|
|
0.8
|
68.4
|
30.8
|
600
|
Jordanian
|
Awawdeh et al (2008) 5
|
|
1.1
|
55.7
|
45.2
|
653
|
Turkish
|
Ozcan et al (2012) 16
|
|
0.7
|
33.3
|
66.0
|
300
|
Chinese
|
Tian et al (2012) 17
|
|
0
|
71.7
|
28.3
|
120
|
Saudi
|
Elkady and Allouba (2013)18
|
|
0.4
|
46.0
|
53.6
|
250
|
Indian
|
Gupta et al (2015) 19
|
|
1
|
70.8
|
28.2
|
511
|
Turkish
|
Bulut et al (2015) 20
|
|
1.1
|
67.0
|
31.8
|
176
|
Jordanian
|
Present study
|
Table 2: Percentages of number of root canals in maxillary first premolars of different population
|
Study
|
Population
|
Type
of study
|
No of
teeth
|
% one
canal
|
% two
canals
|
% three canals
|
|
Pineda,Kuttler(1972)6
|
Mexican
|
In
vitro Radiograph
|
259
|
26.2
|
73.3
|
0.5
|
|
Vertucci (1984) 7
|
American
|
In
vitro (Clearing)
|
400
|
8.0
|
87.0
|
5.0
|
|
Walker
(1987)
8
|
Chinese
|
In
vitro (Radiograph and clearing)
|
100
|
13
|
87
|
0.0
|
|
Pécora
et al (1991) 9
|
Brazilian
|
In
vitro (Clearing)
|
240
|
17.1
|
80.4
|
2.5
|
|
Caliskan
et al (1995) 21
|
Turkish
|
In
vitro (Clearing)
|
100
|
3.9
|
96.1
|
0.0
|
|
Zaatar
et al (1997) 10
|
Kuwaiti
|
In
vivo Radiograph
|
79
|
11.4
|
84.8
|
3.8
|
|
Kartal
et al (1998) 12
|
Turkish
|
In
vitro (Clearing)
|
300
|
8.7
|
89.6
|
1.7
|
|
Chaparroet
al (1999) 13
|
Spanish
|
In
vitro (CS)
|
150
|
1.3
|
95.3
|
3.3
|
|
Deng
et al (2004) 22
|
Chinese
|
In
vitro (Clearing)
|
326
|
48.8
|
50.6
|
0.6
|
|
Oginni
(2004)
23
|
Nigerian
|
In
vivo Radiograph
|
122
|
14.8
|
85.2
|
0.0
|
|
Lipski et al (2005) 14
|
Polish
|
In
vitro Radiograph
|
142
|
2.1
|
88.7
|
9.2
|
|
Cheng,
Weng (2008) 24
|
Chinese
|
In
vitro (Clearing)
|
422
|
10.1
|
87.8
|
1.9
|
|
Atieh
(2008)
15
|
Saudi
|
In
vitro (Clearing)
|
246
|
8.9
|
89.9
|
1.2
|
|
Awawdeh
et al (2008) 5
|
Jordanian
|
In
vitro (Clearing)
|
600
|
3.3
|
95.2
|
1.5
|
|
Ozcan
et al (2012) 16
|
Turkish
|
In
vitro (Radiograph and (CS)
|
653
|
7.8
|
90.7
|
1.5
|
|
Tian
et al (2012) 17
|
Chinese
|
In
vivo (CBCT)
|
300
|
14.3
|
85.0
|
0.7
|
|
Al-Nazhan
et al (2012) 25
|
Saudi
|
In
vivo Radiograph
|
463
|
3.6
|
93.6
|
2.4
|
|
Elkady,
Allouba(2013) 18
|
Saudi
|
In
vivo (CBCT)
|
120
|
5.0
|
95.0
|
0.0
|
|
Ok et
al (2014) 26
|
Turkish
|
In
vivo (CBCT)
|
1379
|
9.6
|
89.4
|
1.0
|
|
Gupta
et al (2015) 19
|
Indian
|
In
vitro(Clearing)
|
250
|
23.2
|
75.6
|
1.2
|
|
Bulut
et al (2015) 20
|
Turkish
|
In
vitro (CBCT)
|
511
|
62.6
|
37.4
|
0.0
|
|
Present
study
|
Jordanian
|
In
vivo Radiograph
|
176
|
0.6
|
98.3
|
1.1
|
CS: cross sectioning
CBCT: cone beam computed tomography
Conclusion
Inspection should be done for the presence of second canal whenever endodontic treatment is planned for maxillary first premolars as the incidence of two canals (either with shared or separate apical foramina) is very high in this tooth among Jordanian population. The most common anatomic variation of this tooth is the presence of three roots and three root canals which must be kept in mind while planning and performing endodontic, restorative or surgical treatment of this tooth.
References
1. Vertucci FJ, Haddix J E, Britto LR. Tooth morphology and access cavity preparation in: Cohen S, Keiser K, editors. Pathways of the pulp. 9th ed. St. louis, Missouri; 2006.
2. Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endodontic Topics. 2005;10(1):3-29.
3. Cantatore G, Berutti E, Castellucci A. Missed anatomy: frequency and clinical impact. Endodontic Topics. 2006;15(1):3-31.
4. Krasner P, Rankow H J. Anatomy of the pulp chamber floor. J Endod 2003; 30: 5-16.
5. Awawdeh L, Abdullah H, Al-Qudah A. Root form and canal morphology of Jordanian maxillary first premolars. J Endod 2008;34:956–61.
6. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol 1972;33:101–10.
7. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589–99.
8. Walker RT. Root form and canal anatomy of maxillary first premolars in a southern Chinese population. Endod Dent Traumatol 1987;3:130–4.
9. Pecora JD, Saquy P, Sousa Neto M, Woelfel J. Root form and canal anatomy of maxillary first premolars. Braz Dent J 1991;2:87–94.
10. Zaatar EI, Al-Kandari AM, Alhomaidah S, Al Yasin IM. Frequency of endodontic treatment in Kuwait: radiographic evaluation of 846 endodontically treated teeth. J Endod 1997;23:453–6.
11. Loh H. Root morphology of the maxillary first premolar in Singaporeans. Aust Dent J 1998;43:399–402.
12. Kartal N, Ozcelik B, Cimilli H. Root canal morphology of maxillary premolars. J Endod 1998;24:417–9.
13. Chaparro A, Segura J, Guerrero E, et al. Number of roots and canals in maxillary first premolars: study of an Andalusian population. Endod Dent Traumatol 1999;15:65–7.
14. Lipski M, Wozniak K, Lagocka R, Tomasik M. Root and canal morphology of the first human maxillary premolar. Durham Anthropol J 2005;12:2–3.
15. Atieh MA. Root and canal morphology of maxillary first premolars in a Saudi population. J Contemp Dent Pract 2008;9:46–53.
16. Ozcan E, Colak H, Hamidi MM. Root and canal morphology of maxillary first premolars in a Turkish population. J Dent Sci 2012;7:390–4.
17. Tian YY, Guo B, Zhang R, et al. Root and canal morphology of maxillary first premolars in a Chinese subpopulation evaluated using cone-beam computed tomography
. Int Endod J 2012;45:996–1003.
18. Elkady AM, Allouba K. Cone beam computed tomographic analysis of root and canal morphology of maxillary premolars in Saudi subpopulation. Egypt Dent J 2013;59:3419–29.
19. Gupta S, Sinha DJ, Gowhar O, et al. Root and canal morphology of maxillary first premolar teeth in north Indian population using clearing technique: an in vitro study. J Conserv Dent 2015;18:232–6.
20. Bulut DG, Kose E, Ozcan G, Sekerci A, Canger E, Sisman Y. Evaluation of root morphology and root canal configuration of premolars in the Turkish individuals using cone beam computed tomography. Eur J of Dent 2015;9:551-7
21. Caliskan MK, Pehlivan Y, Sepetcioglu F, et al. Root canal morphology of human permanent teeth in a Turkish population. J Endod 1995;21:200–4.
22. Deng D, Zhang M, Wu W. The morphology study of root canal system of permanent teeth. Sichuan J Anat 2004;12:22–6.
23. Oginni A. Clinical radiographic estimation of the number of root canals in maxillary first and second premolars among Nigerians. Internet J Dent Sci. Available at: http://print.ispub.com/api/0/ispub-article/6583, 2004;2.
24. Cheng X, Weng Y. Observation of the roots and root canals of 442 maxillary first premolars. Shanghai Kou Qiang Yi Xue 2008;17:525–8.
25. Al-Nazhan S, Al-Daafas A, Al-Maflehi N. Radiographic investigation of in vivo endodontically treated maxillary premolars in a Saudi Arabian sub-population. Saudi Endod J 2012;2:1–5.
26. Ok E, Altunsoy M, Nur BG, et al. A cone-beam computed tomography study of root canal morphology of maxillary and mandibular premolars in a Turkish population. Acta Odontol Scand 2014;72:701–6.
27. Slowey RR. Radiographic aids in the detection of extra root canals. Oral Surg Oral Med Oral Pathol. 1974;37(5):762-72.
28. Martinez-Lozano MA, Forner-Navarro L, Sanchez- Cortes JL. Analysis of radiologic factors in determining premolar root canal systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999: 88: 719–722.
29. Sardar KP, Khokhar NH, Siddiqui MI. Frequency of two canals in maxillary second premolar tooth. J Coll Physicians Surg Pak 2007: 17: 12–14.
30. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MP canal in maxillary molars. J Endod 2002; 28: 324–327.
31. Ahmad IA, Alenezi MA. Root and Root Canal Morphology of Maxillary First Premolars: A Literature Review and Clinical Considerations. J Endod. 2016; 42:861-872
32. 19Soares JA, Leonardo RT. Root canal treatment of three-rooted maxillary first and second premolars--a case report. Int Endod J. 2003;36(10):705-10.
33. Chauhan R, Chandra A. endodontic management of three-rooted maxillary first and second premolars: a case report. Gen Dent 2012; 60: 288-290.