ABSTRACT
Objective: To investigate whether elevated serum leptin levels correlate positively with the occurrence of cardiovascular disease in the randomly selected sample of patients.
Methods: The study enrolled 630 subjects, 322 females and 308 males, who were randomly selected among patients attending the outpatient clinic of Endocrinology and Diabetes in King Hussein Medical Center, Royal Medical Services, Jordan. Diabetes was diagnosed according to American Diabetes Association (ADA) criteria, and blood samples were analyzed using standard biochemical kits at KHMC laboratory. The Data collected were later analysed using SPSS IBM software and Receiver Operating Characteristic Curves were used to determine the positive correlation of elevated serum leptin levels among individuals suffering from cardiovascular disease.
Results: This study revealed a positive relation between the occurrence of cardiovascular disease and serum leptin levels, with the strongest association being observed among males , with an area under the curve ( AUC) of 0.734 as compared to AUC of 0.658 for the female group and 0.588 for both genders together . Significant difference was also observed between diabetic and non- diabetic individuals of both genders, with mean serum leptin levels of 20.19±13.47 and 16.1009±15.98 respectively.
Conclusion: Our results confirm that serum leptin levels are higher in patients with clinically evident CVD, however further data are needed to justify it’s clinical use as a predictor of CVD . Acknowledgement of the limitations of this study may aid in future attempts to demonstrate this relation through conducting similar studies aiming to shed light on this interesting relation which will help us understand with further detail the pathophysiology of obesity- related cardiovascular disease.
Key words: Cardiovascular disease, Diabetes mellitus, Obesity, Serum Leptin levels.
JRMS Dec 2017; 24(3):34-42/DOI:10.12816/0042338
Introduction
According to WHO statistics, cardiovascular disease was the leading cause of mortality for the year 2012, causing 17.5 million deaths out of the 56 million deaths recorded globally (31.25%).(1) Given the fact that almost 80% of the deaths caused by cardiovascular disease are actually preventable, it is of utmost importance to identify risk factors and prevent cardiovascular morbidity and mortality beforehand. (1) One of those factors accounting for the increased cardiovascular mortality is the parallel increment in the prevalence of obesity. Almost 1.9 Billion adults by the year 2016 are overweight, 13% of whom are classified as obese. This increase is mainly attributed to the globalization- urbanization phenomenon. (2) Leptin is a 16 kDa hormone, encoded by the obese gene (ob). It is a peptide hormone formed of 165 amino acids. Identified almost 20 years ago, leptin has since then attracted a lot of attention from researchers in the field of energy utilization and weight control. (3-5) Leptin receptor is a transmembrane protein structurally homologous to gp130 receptor family. Binding of leptin to it’s receptor results in homodimerization and activation of intracellular messengers such as STAT (signal transducer and activator transcription factor), Mitogen-Activated Protein (MAP) and Nitrous Oxide (NO) and others. Leptin is mainly secreted by adipocytes, hence it’s level in the serum is directly proportional to the amount of adipose tissue present in the subject.
It mainly targets receptors in the hypothalamus, through which it ensures maintaining stable energy stores within a relatively narrow range - thus when fat mass increases, leptin levels increase too, suppressing appetite inducing weight loss, and vice versa. It has been shown to increase overall sympathetic activity, facilitate glucose metabolism and improve insulin sensitivity . (5,6) Interestingly, though, obese individuals are leptin resistant rather than deficient, meaning they would need larger amounts of this hormone to achieve favourable results and achieve balance. (7)Although leptin in the normal physiological range has a protective role in regulating pressure and volume in human body, this hormone may have deleterious effects if present in excess, possibly acting as an independent risk factor for the development of cardiovascular disease. (6,8) The prevalence of obesity in northern Jordan according to Khader et al was estimated to be 28.1% among males and 53.1% among females(9), which reflects the huge impact these figures may have on the health care system. According to WHO the leading cause of mortality in Jordan in 2014 was cardiovascular disease- estimated to be 35% of the overall mortality. (10). Hence it is of great importance to identify possible risk factors that may be implemented in obesity related cardiovascular disease. The aim of this study, therefore, is to is to investigate whether elevated serum leptin levels correlate positively with the occurrence of cardiovascular disease. Methods and materials
Subjects:
This cross-sectional study was conducted in the endocrinology clinic at King Hussein Medical City in Amman, Jordan, during the period from August 2009 to May 2010. 630 subjects were enrolled (322 females and 308 males), all aged between 20-70 years. The subjects were randomly selected among visitors of the endocrine clinic at the KHMC during the previously stated period (from August 2009 to May 2010), and every other visitor to the morning clinics was recruited unless proven unfit due to exclusion criteria. Exclusion criteria: Individuals with T1DM were excluded, as well as pregnant females and anyone falling outside the age-range. Also individuals with chronic kidney disease or hypogonadism were excluded. The study was approved by the Royal Medical Services Ethics Committee, and informed consent was obtained from each subject enrolled. Demographic and health history data collection was done by Dr Ahmad Obaidat (see authors) and a specialized team of nutritionists through revision of individuals’ health records and filling forms with relevant data.
Methods
Anthropometric measures were recorded following standard procedures . (11,12) Blood samples were collected after a 10-12 hour overnight fast. Standard biochemical kits (Cobas c 311 Hitachi) were used to run the tests following standard procedures at Princess Iman Centre for Laboratory Research and Science Center, KHMC. Body mass index was calculated using the formula BMI= weight (kg)/Height2 (m2). Subjects were classified to non-obese: BMI 18.5- 24.9, overweight 25.0-27.5, and obese 27.5-40 kg/m2. Diabetes was diagnosed according to American Diabetes Association (ADA)13 recommendations as fasting plasma glucose 126mg/dl on two or more occasions and/or HbA1c 6.5%.
Subject’s medical records were used to identify patients with composite cardiovascular disease and ischemic heart disease, including individuals with previous acute coronary event, chronic stable angina, patients with previous coronary artery bypass surgery of following coronary angiography with proved coronary artery disease (occlusive or non- occlusive).
Statistical analysis:
Data were analyzed using the statistical package for social sciences IBM SPSS Statistics 20 . Data were presented in terms of mean ± standard deviation, p values were provided where indicated. Levels of statistical significance were identified as p values of ≤ 0.05, ≤ 0.01 and ≤ 0.001. Receiver operating characteristic curves ( ROC) were used to determine the efficiency of leptin as a biochemical marker for cardiovascular disease (CVD).
Results
Descriptive: demographic analysis of the study group (Table I) : Anthropometric and clinical indices are shown including means and standard errors of deviation for each variable. 630 individuals were recruited, 322 (51%) women and 308 (49%) men. The mean age for the study group was 43.27±0.5 years with no significant difference between males and females . The mean BMI was 30.40 ± 0.36 for males, and 32.24 ± 0.47 for females. 105 (34.1%) of men and 187 (57.6%) of women were hypertensive. 133 (43.2%) of men and 134 (41.6%) of women had diabetes mellitus, and 180(58.4%) of men, 136 (42.2%) of women were hyperlipidemic. Clinical and biochemical indices by gender for the study group. (Table II ): Clinical and biochemical indices are displayed showing means and standard errors of deviation for each variable. The mean fasting blood glucose was 124.30 ±3.39 for males, and 119. 15 ± 3.25 for females with no statistically significant difference . The mean leptin in the male study group was 10.64 ± 9.94 and in the females 23.96 ± 6.6 with a p value ˂0.001 . Serum leptin levels were higher in obese individuals (mean 21.62 ± 16.27 ng/ml; range 0.3-160 ng/ml) as compared to lean subjects (mean 9.15 ± 8.44 ng/ml ; range 0.1- 48.5 ng/ml) p-value < 0.001). (Figure 1) Mean BMI was 22.69 ± 1.45; range 18.6-24.9 for the non-obese group , and 35.57 ± 5.215; range 30.0 to 66.9 for the obese group. (Figure 1) The mean serum level of leptin was much higher in both obese and non-obese females 28.4 and 14.4 respectively ,with a mean of 23.96 ± 6.6 , as compared to obese and non-obese males with 14.17 and 3.99 respectively and an overall mean of 10.63 ± 9.94 ( p- value < 0.001 ). A significant difference was also observed among the patients with diabetes mellitus versus non –diabetic patients with a mean leptin of 20.19 ± 13.47 and 16.1009± 15.98 respectively (p- value < 0.001). Further analysis was performed using IBM SPSS statistics 20 to assess the predictive value of leptin as an indicator of cardiovascular disease. Among males, 21 individuals who were positive for cardiovascular disease had serum leptin levels above mean, as opposed to 12 individuals who were also suffering from cardiovascular disease but their leptin levels were found to be below mean (p- value 0.002) . (Figure 2) When the female group data was analysed, however, it failed to show the same statistical significance. Females with cardiovascular disease and serum leptin levels above mean were 19 out of a total of 36, the remaining 17 had below mean leptin levels ( p- value 0.208). (Figure 2) No statistical significance was observed in leptin levels among patients with diabetes and those with normal glucose metabolism who suffer from cardiovascular disease. Additionally, serum leptin levels are directly proportional to serum insulin levels (Figure 6).
Receiver operating curves ( ROC):
ROC curves to determine the efficiency of leptin measurement as a marker of cardiovascular disease. Data analysis using ROC curves was performed aiming to identify the area under the curve, as well as the sensitivity and specificity of leptin as an indicator of CVD. The area under the curve was 0.588 for both genders together- suggesting some positive relation , however not enough to justify clinical use( see figure 3). AUC for the female group was 0.658 (Figure 4) and for males 0.734 showing an even more positive correlation between leptin levels and cardiovascular disease (Figure 5)
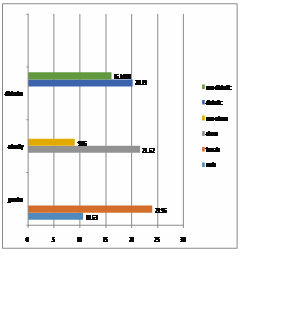 Figure 1
Figure 1 ( leptin levels compared to gender, obesity and diabetes)
Figure 2 ( leptin levels in obese diabetic, obese non-diabetic
Figure 3 Area Under the Curve for both genders with CVD: 0.588
Figure 4 Area Under the Curve for females with CVD : 0.658
Figure 5 Area Under the Curve for males with CVD : 0.734
Table I: Anthropometric Characteristics by gender for the study group
|
|
Anthropometric Characteristics by gender for the study
group
|
|
Indices
|
Mean± Standard Error of Deviation
|
|
Total (n=630)
|
Men (n= 308)
|
Women (n=322)
|
|
Age (Years)
|
43.26±0.54
|
42.19 ± 0.75
|
44.28 ±0.79
|
|
Weight( Kg)
|
85.82±1.12
|
90.34 ± 1.16
|
81.30 ± 1.21
|
|
Height (cm)
|
165.53±0.35
|
172.18 ± 0.35
|
158.89 ± 0.35
|
|
Waist Circumference (cm)
|
99.73±0.7
|
101.79 ± 0.83
|
97.76 ± 1.09 P
˂0.01
|
|
Body Mass Index (Kg/ m2)
|
31.79±0.38
|
30.40 ± 0,36
|
32,24 ± 0.47
|
|
Waist to Height Ratio
|
0.605±0.01
|
0.59 ± 0.00
|
0.62 ± 0.01
|
Table II: Clinical and Biochemical Indices By gender
|
|
Clinical and Biochemical Indices By gender
|
|
Indices
|
Mean ± Standard of Error of Mean
|
|
Total (n=630)
|
Men (n=308)
|
Women (n=322)
|
|
Fasting Blood Glucose (mg/dl)
|
121.67±2.35
|
124.30± 3.39
|
119.15 ± 3.25
|
|
Systolic Blood Pressure (mmHg)
|
134.87±1.12
|
132.69 ± 1.73
|
136.96 ± 1.42
|
|
Diastolic Blood Pressure (mmHg)
|
81.74±0.46
|
79.58 ± 0.68
|
83.80 ± 0.61 p˂ 0.001
|
|
Leptin Level (nm/ml)
|
10.80±0.43
|
10.63 ± 9.94
|
23.96 ± 6.6 P ˂ 0.001
|
|
High Density Lipoprotein (mg/dl)
|
48.44±0.78
|
46.23 ± 0.75
|
50.66± 0.83 P ˂0.001
|
|
Triglycerides (mg/dl)
|
163.18±4.72
|
172.45 ± 4.47
|
153.91 ± 4.96 P ˂ 0.01
|
Figure 6 :( leptin levels compared to insulin secretion)
Discussion
This is one of a few studies conducted to investigate whether elevated serum leptin levels correlate positively with the occurrence of cardiovascular disease in the randomly selected sample of patients.
The link between leptin and cardiovascular disease could be, in part, due to the fact that leptin is a peptide hormone primarily synthesized by adipocytes(14), thus it’s level is directly proportional to the amount of adipose tissue in the individual. As is well recognized, obesity is a worldwide rapidly growing metabolic disorder with dramatic burden on the health and economy of both the developed and developing countries. Long term studies relate obesity to cardiovascular disease ; some even prove it to be an independent risk factor for coronary atherosclerosis. (6,15) This occurs mostly secondary to activation of the sympathetic nervous system, as well as impairment of the endothelial function.(6,16,17) Though leptin deficiency is the cause of obesity for some rare cases, most obese individuals are leptin resistant (7), thus having high levels of leptin in their circulation. Our results are in keeping with this observation, as leptin levels were consistently higher among obese individuals as opposed to non-obese subjects, and this was demonstrated in both genders with a statistically significant p-value of ˂ 0.001. Leptin levels were also higher in females, and this is mostly due to the lowering effect testosterone exerts on leptin production. (18.19) Leptin has also been identified in several studies as an independent biomarker for metabolic syndrome.(20-25)In the Framingham Third Generation Cohort, leptin concentrations were associated with increased risk of metabolic syndrome . (26)This effect may be through activation of lipolytic hormones, such as glucocorticoids and catecholamines, leading to hyperlipidemia, central obesity and insulin resistance.(20)Metabolic syndrome itself is a constellation of metabolic disorders that increase the risk of CVD (,18,27). Upon further analysis, our results have shown a statistically significant difference in leptin levels among patients with diabetes mellitus compared to patients with normal glucose metabolism. This is consistent with data from several different populations all in keeping with a positive correlation between insulin level and leptin concentration,(28,29)as insulin resistant men showed higher levels of leptin than insulin sensitive men regardless of the body fat mass (Figure 6). The possible explanation for this observation may be due to leptin activity in the pancreas, which would normally inhibit insulin secretion, however due to insulin resistance there is loss of leptin- induced inhibition of glucose-stimulated insulin secretion, which contributes to insulin resistance and Type 2 Diabetes. But how would leptin act at the molecular level as an independent risk factor for CVD? In it’s normal physiological levels leptin plays a key role in blood pressure and volume regulation,(8,15)as it is capable of regulating cardiac and vascular contractility through a local NO – dependent mechanism. So in vascular endothelial cells leptin activates the stress- activated protein kinase (SAPK) and Jun NH2-terminal kinase (JNK)transduction pathways, which are also activated by ROS – thus explaining the hazardous effects of sustained hyperleptinemia .(30) However in the case of hyperleptinaeimia due to leptin resistance, it has been considered as a pathophysiological trigger for cardiovascular disease, accounted even as an independent risk factor. (6,31) Once leptin signalling in the hypothalamus is disrupted, the energy balance loses equilibrium and obesity ensues. (14,32,33) Given the fact that leptin resistance is tissue specific, it tends to affect the hypothalamic signalling only, whereas the peripheral signalling remains unchanged(34). For instance the sympathetic activation to maintain blood pressure control is still retained, partly attributing to the deleterious effects of leptin when present in high levels. When APOE-1 deficient mice were treated with recombinant leptin treatment, it further promoted atherosclerosis and thrombosis. On the other hand, leptin resistance is also proatherogenic.(7)Once leptin binds to it’s receptor, IRS-1 and IRS-2 activity increases, which eventually leads to suppressed PI-3 activity, a well known positive inotropic mediator for the heart and the vasculature, which leads to reduced cardiac inotropicity.(6,35,36)This may also explain the onset of insulin resistance observed in patients with chronic hyperleptinemia. (37) An interesting observation, though, is that Leptin may also play an important role in the catabolic cardiac cachexia which affects patients with congestive heart failure- as it has been found to be elevated in individuals with congestive heart failure.(6,38) Our results have shown a positive relation between serum leptin levels and the existence of clinically evident cardiovascular disease. The findings were more consistent among males, as the AUC (Area Under the Curve) for leptin used as a risk factor for CVD was 0.734 (figure5) , and in females 0.658 (Figure 4) , revealing a less positive correlation. These findings are consistent with several studies that have been conducted attempting to demonstrate the relation between leptin and CVD. Li et al (21) demonstrated that serum leptin levels are positively correlated with CVD and Metabolic Syndrome in a group of 957 Taiwanese adults. Wallace et al (28) in a large prospective study (WOSCOPS) demonstrated that leptin is a novel, independent risk factor for CVD. Preliminary data from the group included in the study linked leptin to C- Reactive Protein (CRP) – a marker of chronic low grade inflammation and predictor of risk for CVD. Welch et al demonstrated the positive correlation between diabetes and hyperleptinemia in a group of 5804 patients both males and females, studied over the period between 197-1999. However the data provided weren’t sufficient to demonstrate a positive correlation between hyperleptinemia and cardiovascular disease.(39) Their findings were also consistent with the Quebec cardiovascular study (40) .
Conclusion
In conclusion, our results confirm that leptin levels are higher in patients with clinically evident CVD, however further data are needed to justify it’s clinical use as a risk factor for CVD . Acknowledgement of the limitations of this study may aid in future attempts to demonstrate this relation through conducting similar studies aiming to shed light on this interesting relation which will help us understand with further detail the risk factors implemented in obesity- related cardiovascular disease.
Study limitations:
Single measurements of leptin levels may not be a fair reflection of the mean levels of leptin in the individuals involved in the study group ( leptin variability). Additionally the degree of diabetes control was not accounted for when measuring leptin levels, as well as other factors that might interfere with metabolism such as thyroid dysfunction. The cardiovascular disease in this study was identified as only the clinically evident cardiovascular disease- which may not be sufficient to account for the true existence of cardiovascular disease among these individuals given the fact that some patients may harbour silent atherosclerosis. A possible alternative might be the usage of cardiovascular risk profiles or software calculators that predict the risk of CVD .
References
1.http://www.who.int/mediacentre/factsheets/fs317/en/
2.http://www.who.int/mediacentre/factsheets/fs311/en/
3. Zhang F, Chen Y, Heiman M, Dimarchi R. Leptin: structure, function and biology. Vitam Horm. 2005;71:345–372.
4. Leibel RL, Chung WK & Chua CS Jr 1997. The molecular genetics of rodent single gene obesities. Journal of Biological Chemistry 272 31937–31940.
5. Friedman JM 2002 The function of leptin in nutrition, weight and physiology. Nutrition Reviews 60 S1–S14.
6. Ren J. Leptin and hyperleptinemia- from friend to foe for cardiovascular function. J Endocrinol. 2004 Apr;181(1):1-10.
7. Ronghua Yang, Lili A. Barouch . Leptin signaling and obesity ,cardiovascular consequences. Circulation Research.2007;101:545-559.
8. Patel SB, Reams GP, Spear RM, Freeman RH, Villarreal D. Leptin: linking obesity, the metabolic syndrome , and cardiovascular disease. Curr Hypertens Resp. 2008 Apr;10(2): 131-7.
9. Khader Y1, Irshaidat O, Khasawneh M, Amarin Z, Alomari M, Batieha A. Overweight and obesity among school children in Jordan: prevalence and associated factors. Matern Child Health J. 2009 May;13(3):424-31. doi: 10.1007/s10995-008-0362-0. Epub 2008 May 22.
10. http://www.who.int/nmh/publications/ncd-profiles-2014/en/
11. Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey: anthropometry and physical activity monitor procedures manual [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; 2005 January 1 [cited 2014 October 11]. Available from: http://www.cdc.gov/nchs/data/nhanes/ nhanes_ 05_06/BM.pdf.
12 . Lee RD, Nieman DC. Nutritional Assessment. 5th ed. New York (NY): McGraw-Hill Education; 2010.
13. American Diabetes Association : Diabetes Care 2015 Jan; 38(Supplement 1): S8-S16. https://doi.org/10.2337/dc15-S005
14. Hou N, Luo JD. Leptin and cardiovascular diseases. Clin Exp Pharmacol Physiol. 2011 Dec;38(12) 905-13.
15. Sowers JR 1998 Obesity and cardiovascular disease. Clinical Chemistry 44 1821–1825.
16. Kuo JJ, Jones OB & Hall JE 2003 Chronic cardiovascular and renal actions of leptin during hyperinsulinemia. American Journal of Physiology. Regulatory, Integrative and Comparative Physiology 284 R1037–R1042.
17. Julius S, ValentiniM&Palatini P 2000 Overweight and hypertension: a 2-way street? Hypertension 35 807–813.
18. Van Vliet-Ostaptchouk JV, Nuotio ML, Slagter SN et al. The prevalence of metabolic syndrome and metabolically healthy obesity in Europe: a collaborative analysis of ten large cohort studies. BMC Endocr Disord 2014;14:9-22.
19. Hamed M. Haddad SH, AL Quobili F. Serum uric acid and leptin levels in metabolic syndrome. Int J Pharm Sci Rev Res 2013;20:21-7.
20. Ahmad A. Obeidat1§, Mousa N. Ahmad2, Fares H. Haddad3 et al 2016. Leptin and uric acid as predictors of metabolic syndrome in jordanian adults; Nutrition Research and Practice. 2016.
21. Li WC, Hsiao KY, Chen IC, Chang YC, Wang SH, Wu KH. Serum leptin is associated with cardiometabolic risk and predicts metabolic syndrome in Taiwanese adults. Cardiovasc Diabetol 2011;10:36-42.
22 . Huang KC, Lin RC, Kormas N, et al: Plasma leptin is associated with insulin resistance independent of age, body mass index, fat mass, lipids, and pubertal development in nondiabetic adolescents. Int J Obes Relat Metab Disord 2004, 28(4):470-5.
23. Moreno LA, Pineda I, Rodriguez G, et al: Leptin and metabolic syndrome in obese and non-obese children. Horm Metab Res 2002, 34(7):394-9.
24. Hodge AM, Boyko EJ, de Courten M, et al: Leptin and other components of the Metabolic Syndrome in Mauritius–a factor analysis. Int J Obes Relat Metab Disord 2001, 25(1):126-31.
25. Ukkola O, Kesäniemi YA. Leptin and high-sensitivity C-reactive protein and their interaction in the metabolic syndrome in middle-aged subjects. Metabolism 2007;56:1221-7.
26 Ingelsson E, Larson MG, Yin X, et al: Circulating ghrelin, leptin, and soluble leptin receptor concentrations and cardiometabolic risk factors in a community-based sample. J Clin Endocrinol Metab 2008, 93(8):3149-57.
27. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ et al ; International Diabetes Federation Task Force on Epidemiology and Prevention; Hational Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; International Association for the Study of Obesity. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009;120:1640-5.
28. Wallace AM, McMahon AD, Packard CJ, Kelly A, Shepherd J, Gaw A, Sattar N; WOSCOPS Executive Committee. Plasma leptin and the risk of cardiovascular disease in the west of Scotland coronary prevention study (WOSCOPS). Circulation 2001;104:3052-6.
29. Ookuma M, Ookuma K & York D1998 Effects of leptin on insulin secretion from isolated rat pancreatic islets. Diabetes 47 219–223.
30. Bouloumie A, Marumo T, Lafontan M & Busse R 1999 Leptin induces oxidative stress in human endothelial cells. FASEB Journal 13 1231–1238.
31. ReillyMP,IqbalN,SchuttaM et al. Plasma leptin levels are associated with coronary atherosclerosis in type 2 diabetes. J Clin Endocrinol Metab. 2004;89: 3872–3878.
32. Cohen P, Zhao C, Cai X, Montez JM, Rohani SC, Feinstein P, Mombaerts P, Friedman JM. Selective deletion of leptin receptor in neurons leads to obesity. J Clin Invest. 2001;108:1113–1121.
33. Bates SH, Myers MG. The role of leptin- STAT signalling in neuroendocrine function : an integrative prospective . J Clinic Invest .2001;108:1113-1121.
34. Mark AL, Correia ML, Rahmouni K, Haynes WG. Selective leptin resistance: a new concept in leptin physiology with cardiovascular implications. J Hypertens. 2002;20:1245–1250.
35. Northcott CA, Poy MN, Najjar SM & Watts SW 2002 Phosphoinositide 3-kinase mediates enhanced spontaneous and agonist-induced contraction in aorta of deoxycorticosterone acetate-salt hypertensive rats. Circulation Research 91 360–369.
36. von Lewinski D, Voss K, Hulsmann S, KoglerH&Pieske B 2003 Insulin-like growth factor-1 exerts Ca2+-dependent positive inotropic effects in failing human myocardium. Circulation Research 92 169–176.
37. Harvey J, McKay NG, Walker KS, Van der Kaay J, Downes CP & Ashford ML 2000 Essential role of phosphoinositide 3-kinase in leptin-induced K(ATP) channel activation in the rat CRI-Gi insulinoma cell line. Journal of Biological Chemistry 275 4660–4669.
38. Schulze PC, Kratzsch J, Linke A, Schoene N, Adams V, Gielen S, Erbs S, Moebius-Winkler S & Schuler G 2003 Elevated serum levels of leptin and soluble leptin receptor in patients with advanced chronic heart failure. European Journal of Heart Failure 5 33–40.
39. Paul Welsh, PHD,1 Heather M. Murray, MSC,2 et al . Leptin Predicts Diabetes but not Cardiovascular Disease . Diabetes Care. 2009 Feb; 32(2): 308–310.
40. Couillard C, Lamarche B, Mauriege P, et al. Leptinemia is not a risk factor for ischemic heart disease in men: prospective results from the Quebec Cardiovascular Study. Diabetes Care. 1998;21:782–786