ABSTRACT
Objective: To assess wound-related complications in patients
undergoing open-heart surgery through minimally invasive approach, and
to assess an alternative safer access to standard sternotomy.
Methods: Over
30 months period ninety patients underwent elective open heart surgery
via upper sternotomy incision risk factors for wound infection. Sternal
wound complications were classified according to the seriousness and the
extent of wound infection. Patients were followed-up for one month
after hospital discharge.
Results: Of the 90 patients,
73 (81%) were males and 17 (19%) were females. Age ranged between 19-72
years (mean 40 years). The procedures performed were valve surgery,
coronary artery by-pass grafting and septal myomectomy in 86 (95.6%), 2
(2.2%) and 2 (2.2%) patients, respectively. Simple wound dehiscence
occurred in 2, superficial wound infection in 6. None had deep wound
infection or sternal wound dehiscence. One patient died from prosthetic
valve endocarditis without sternal wound complications.
Conclusion:
Upper median sternotomy significantly reduces the serious complication
of sternal wound closure and hence the hospital stay of the patients as
well as the utilization of the medical resources.
Key words: Sternal wound, Sternal wound complications, Upper mid-sternotomy.
JRMS June 2003; 10(1): 12-14 IntroductionFull median sternotomy provides an excellent approach to the heart and great vessels but serious wound- related complications might be encountered. We conducted this study to assess the rate of such complications in patients undergoing minimally invasive sternal approaches.
MethodsBetween January 18, 1997 and July 12, 1999 (30 months), ninety adult patients underwent open-heart surgery via an upper sternotomy incision (Fig.1). Data were prospectively collected. Patients were admitted to hospital 48 hours before surgery. The patients were anesthetized in the supine position and intubated with a
single lumen endotracheal tube, scrubbed with povidine iodine and was draped in the usual manner. External defibrillator was kept stand by in each case. A 4.5 - 8 cm incision was made beginning half-way between the sternal notch and the sterno–manubrial angle. The incision was carried down to the sternum using cautery. The sternum was opened from the sternal notch to the level of the third or fourth intercostal space and extended into the intercostal space on the right side (Fig. 1). To help reduce the potential for air emboli, the field was flooded with carbon dioxide (CO2) at 6 liters per min. This displaces oxygen (O2) and nitrogen (N2) and any bubbles of CO2 are rapidly absorbed. Venous drainage was accomplished using dual stage venous cannulae placed in the atrial appendage. The arterial cannulation was done via either femoral or aortic cannulation. Cross clamp time and bypass time were recorded for each patient. At the conclusion of the surgical procedure the incision was closed using stainless steel wires for the sternum and absorbable sutures for the subcutaneous tissue and skin. Prophylactic antibiotics (Cefuroxime and gentamcin) were administered for 48 hours after the procedure.
Risk factors for sternal wound complications including renal impairment, peripheral vascular disease (PVD), chronic obstructive airway disease (COPD), smoking, pump time, cross clamp time, left ventricular ejection fraction (EF) and diabetes mellitus were recorded.
Sternal wound complications were classified as: Simple wound dehiscence (SWD), superficial wound infection (SWI) and deep wound infection (DWI) with sternal dehiscence and mediastinitis. Patients were followed- up in the hospital and for one month after discharge.
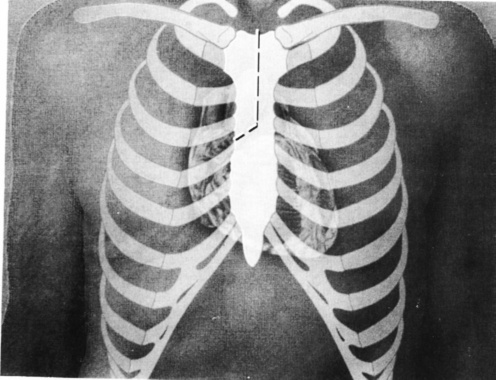
Fig. 1. Upper mid-sternotomy showing the direction of the sternal incision (Dotted line).
Results Of the 90 patients: 73 (81%) were males and 17 (19%) were females. Age ranged between 19-75 years with a mean age of 40 years. The average weight was 65.7 kg. Valve surgery was the commonest performed procedure (96%). Aortic valve replacement (AVR) in 75 patients, mitral valve replacement (MVR) in 5, MVR & AVR in 6. Two patients had coronary artery bypass graft (CABG) and 2 patients had septal myomectomy (Table I). Six patients had diabetes mellitus (6%). Left ventricular EF was normal in 57 cases (64%). Mild, moderate and severe EF reduction were noticed in 18 (30%), 9 (10%) and 6 (6%) patients respectively. Nonsmokers were 36 (40%) and smokers 54 (60%). Three patients had COPD and 3 had renal impairment. Average pump and cross clamp times were 76 and 46 minutes respectively (Table II).
Of the 90 patients, two had SWD, 6 patients had SWI
and none had DWI or dehiscence of the sternum. One patient died from prosthetic valve endocarditis after he had been operated upon two times and received a full course of antibiotics.
Table I: List of the operative procedures
|
Operative procedure
|
No. of Patients
|
|
*AVR
|
75
|
|
**MVR
|
5
|
|
AVR & MVR
|
6
|
|
^CABG
|
2
|
|
Septomyomectomy
|
2
|
* AVR: Aortic valve replacement
** MVR: Mitral valve replacement
^CABG: Coronary artery bypass graft
Table II: Distribution of risk factors
|
*DM
|
6 cases
|
6%
|
|
Average weight
|
65.7 Kg
|
|
|
Ejection fraction:
Normal
Mild
Moderate
Severe
|
No. of
patients
57
18
9
6
|
64%
20%
10%
6%
|
|
Smokers
|
54
|
60%
|
|
**COPD
|
3
|
3%
|
|
Renal impairment
|
3
|
3%
|
|
Average pump time
|
76 min
|
|
*DM: Diabetes mellitus
** COPD: Chronic obstructive airway disease
Discussion
Median sternotomy is one of the most frequently used surgical incisions in cardiac surgery all over the world. Both patient- and operation- related factors are involved in the pathogenesis of sternal wound complications.
Mediastinitis occurs in 1% to 2.5% of patients who undergo standard median sternotomy with the prevalence unchanged for the last 20 years (1). Valvuar procedures carry an infection rate of 1.8%, slightly higher than that seen in patients who undergo coronary artery bypass procedures. The incidence rises to 2.5% - 3% in patients who undergo a concomitant procedure (2). Ottino and associates have reported that significant risk factors for mediastinitis include the hospital environment, the interval between admission and operation, re-operation and rewiring (2). Patients may be contaminated before, during and after operation, and any kind of reintervention may predispose to the development of a wound infection (2). Prolonged ventilation and female sex were both associated with marked increase in the risk of major sternal complications. Age and weight were associated with a less, but still statistically significant risk (3). The incidence of infection may be increased if a single internal mammary artery (IMA) is used; the infection
rate approaches 5% if both arteries are used (4).
Surgical infection does not result from mere presence of bacteria but rather from a complex interaction between the host’s defence mechanisms and pathogenic microorganism. American A critical bacterial count of 105 microorganisms per gram of tissue is associated with development of infection (5).
Adequate sternal immobilization appears to have an effect on the incidence of post–median sternotomy mediastinitis (6) and may be it was contributing factor that protected our patients in this series from having this complication. Osteoporosis and severe pulmonary disease predispose to the development of sternal instability (6). Rigid fixation principles should be employed to minimize inflammation and fluid collections, as well as to optimize osteosynthesis (6).
The main patient-related factors include obesity, malnutrition, osteoporosis, DM, corticosteroid use, COPD and history of radiation therapy to the chest (7,8). These factors are common in cardiothoracic patients; they were not uncommon in our series.
Operative factors also may play a role. Technical errors in sternotomy closure, breaks in sterile techniques and bilateral IMA harvest all increase the probability of wound break down (4,8,9). Attention to surgical details and refinements in the operative techniques of sternal wound closure in patients at high risk can help reduce the morbidity and mortality associated with sternal wound complications.
Although the sternum was most commonly closed with interrupted stainless steel wires, many innovative methods of sternal closure have been developed, both for primary closure and reclosure. Among the techniques suggested for the closure of a fragile sternum or sternum with multiple fractures are the Robeicsek weave (10) and figure of 8 pericostal sutures (9). The drawback of the Robicsek weaves technique of sternal closure is that it may disrupt the collateral blood supply by producing a constricting weave around the vessels and it is not as effective in approximating the top and bottom of the gaping sternum.
Of the two patients that had SWD, none grew an organism on wound culture so they were considered technical inadequacy in wound closure. The other six patients who developed SWI had Staphylococcus aureus coagulase negative in four patients, and staphylococcus aureus coagulate positive in two patients. All were treated by the proper antibiotics, frequent dressing and were discharged early from hospital.
Conclusion
By using the minimally invasive approach (the upper sternotomy) most of the serious complications of sternal wound closure are reduced significantly and this will have a positive reflection on the morbidity and hospital stay as well as the utilization of the medical resources. Even those cases who developed SWI were easily managed because the wounds were small and stable.
Probably, it is premature to come up with this conclusion with such a number of patients but it is clear that minimally invasive access is safe as an operative technique and it reduces the morbidity of sternal wound complications in high-risk patients.
References
1. Loop FD, Lytle BW, Cosgrove DM, et al. Sternal wound complications after isolated coronary artery bypass grafting: Early and late mortality, morbidity, and cost of care. Ann Thorac Surg 1990; 49: 179-187.
2. Ottino G, De Paulis R, Pansini S, et al. Major sternal wound infection after open-heart surgery: A multivariate analysis of risk factors in 2.579 consecutive operative procedures. Ann Thorac Surg 1987; 44: 173-179.
3. Breyer R, Mills S, Hudspeth A, et al. A prospective study of sternal wound complications. Ann Thorac Surg 1984; 37: 412-416.
4. Culliford A, Cunningham JJ, Zeff R, et al. Sternal and costochondral infection following open-heart surgery. A review of 2.594 cases. J Thorac Cardiovasc Surg 1976; 72: 714-26.
5. El-Gamel A, Yonan NA, Hassan R, et al. Treatment of mediastinitis: Early modified Robicsek closure and pectoralis major advancement flap. Ann Thorac Surg 1998; 65: 41-47.
6. Gottlieb L, Pielet R, Karp R, et al. Rigid internal fixation of the sternum in postoperative mediastinitis. Arch Surgery 1994; 129: 489-493.
7. Demmy T, Park S, Liebler G, et al. Recent experience with major sternal wound complications. Ann Thorac Surg 1990; 10: 458-462.
8. Shafir R, Weiss J, Gur E, et al. Sternal wound infection: Our experience with 200 cases. J Cardiovasc Surg (Torino) 1994; 35: 103-104.
9. Di MRJ, Lee M, Bekoe S, et al. Interlocking figure-of-8 closure of the sternum. Ann Thorac Surg 1989; 47: 927-929.
10. Robicsek F, Daugherty H, Cook J. The prevention and treatment of sternum separation following open-heart surgery. J Thorac Cardiovasc Surg 1977; 73: 267-268.