ABSTRACT
Objective: To evaluate the outcomes of Gastric banding as weight reduction surgery at King Hussein medical center, over six years period.
Methods: This retrospective study was conducted at King Hussein Medical Center , from Jan-2010 to Feb-2016. In six years duration, two hundred and fifty patients underwent gastric band surgery and enrolled in this study. Patient data information, age, sex, and their base line weights and Body Mass Index were collected, thereafter surgery data follow up protocol had been attained to assess the procedure outcomes in terms of either its efficacy for weight reduction or its complications that may be encountered after the procedure.
Results: The majority of patients were females and account for (88%), with a mean age of 28.5 years for both sexs and the mean preoperative Body Mass Index was 46.07 kg/m². The outcomes of gastric band were as follows, pouch dilatation 12%, Gastroesophageal reflux 7%, band slippage 2%, band migration 2%, and gastric erosion was 1.6%. The reoperation rate for band removal was 20.0%. The average of excess body weight reduction after surgery was 40.40%, 45.12% and 43.5% in the first, second and third year respectively.
Conclusion: Although the outcome of gastric band regarding weight reduction was acceptable, it has many adverse effects after surgery. At the same time, the high reoperation rate for band removal makes the band insertion as weight reduction surgery unfavorable option.
Keyword: Band removal, Bariatric surgery, Body mass index, Excess body weight, Gastric Banding.
JRMS April 2018; 25(1):37-43/DOI:10.12816/0046993
Introduction
By definition, obesity is when the body mass index (BMI) is more or = 30 kg/m², While the BMI is equal to weight in Kg divided by height square in meter. All studies world widely proof that, a recent increase in the incidence of morbid obesity, and this disease has been defined as a major public health problem. Medical or nonoperative management of obesity offers low success and have a high rate of failure, while surgical approach offers optimal option for weight reduction and significant decline in obesity associated co-morbidities, as described by Kissane NA and his colleague, (1). Gastric banding is one of these procedures and its restrictive bariatric surgery, which has been performed in many Centers world widely including King Hussein Medical center. Obesity can be classified into four classes as shown in table1; surgical management could be the best option for those with BMI more than 40 kg/m². In the other hand, patients that categorized as class 2 obesity and suffering from comorbidities (hypertension, diabetes Milletes (DM), sleep apnea, etc.) may be improved dramatically by surgical option. Any BMI less than 35kg/m2 considered class 1, and all are not surgical potentials. (2)In Jordan and in the last few years, it had been estimated that, a recognized percentage of adult's mortality and morbidity, aged from 20 to 64 years are within direct relation to obesity, as reported by Dr Hyader Aldomi at University of Jordan in 2010, about 39.8% of population in Jordan are obese, while 42% are overweight and only 18.2% are within normal weight range. (3)As published by Dr. Prem Lobo and his colleges, Excess body Weight loss (EBWL) can be satisfied after this procedure; however for some extent it's insufficient in a recognized proportion of patients. Year by year follow up post gastric banding showed substantial increase in its associated complications. (4,5) Our study examined patients’ postoperatively over 6 years duration. Tow hundred and fifty patients enrolled in this study. Although the procedures underwent by five different surgeons and under optimum surgical environment (so its not operator dependent), but the results showed high reoperation rate, and significant percentage of band complications, which subsequently makes the band option unfavorable. The study results are almost similar to other international studies.
Methods
In this retrospective study; we collected patient’s demographics before surgery, and observe the procedure outcomes after surgery from 2010 to 2016. Then the data was analyzed and compared with the results reported in literature studies. From 1st of February 2010 till 30th of November 2012, tow hundred and fifty morbidly obese patients were undergone Gastric Banding surgery at King Hussein Medical Center and followed regularly for the next five years after surgery till Feb.2016. Patients who were not followed regularly in our clinic excluded from this study. So, the target population of this study is morbid obese patients whom underwent gastric band surgery.First of all we classify the patients according to their BMI, there were 213 patients with BMI between (40 to 50) kg/m², and classified as obesity class3, 30 patients with BMI more than 50 kg/m and only 7 patients their BMI was less than 40 table II. Then we determined which patient is indicated for surgery, so any patient with BMI more than 40 kg/m² or between 35-40 kg/m² with co morbidities became potentials for gastric band procedure. Co morbidities that can be considered an indication for surgery are Diabetes, Hypertension, or sleep apnea. The number of patients with co morbidity is shown in table III. Before transferring the indicated patients for surgery, all patients had been assessed by psychologist, endocrinologist and nutritionist as preoperative preparation for surgery.
Table 1: Obesity classes
|
Obesity class
|
BMI
|
|
Normal
|
(18-25) kg/m²
|
|
Overweight
|
(>25-30)
kg/m²
|
|
Obesity class 1
|
(30-35) kg/m²
|
|
Obesity class 2
|
(>35-40)
kg/m²
|
|
Obesity class 3
|
(40-50) kg/m²
|
|
Obesity class 4
|
>50 kg/m²
|
BMI: body mass index
Table II: Numbers of patients according to their BMI before surgery
|
BMI (kg/m²)
|
TOTAL N = 250
|
|
More than 50
|
30 patients
|
|
Between 40-50
|
213 patients
|
|
Less than 40
|
7 patients
|
Table III: Number of patients with co morbidities
|
Variable
|
Total N= 25
|
|
DM
|
13
|
|
HTN
|
10
|
|
Sleep apnea
|
2
|
Procedure Technique
After creation pneumoperitonium, band was introduced in the abdominal cavity and applied on the upper part of stomach. To avoid lateral slippage, a stitch was applied between the left crus and the band, and between the greater curvature and the left crus. In order to avoid anterior slippage, the pouch was secured by few gastric stitches. The result is small gastric pouch of less than 20 cc, finally the adjusting part of band and called the port was fixed to anterior abdominal wall to be easily accessible. Patients kept postoperatively for one or two days in our hospital, then discharged with appointment for 1st outpatient clinic after 2 weeks, and then twice monthly for the first year, after that follow-up examinations were performed three monthly in the 2nd year, then yearly up to 5 years. A liquid clear diet was advised in the first 14 days postoperatively, and then soft diet added for the next two weeks, after that normal diet was introduced. During follow up period any Patient complaint was evaluated clinically and investigated by gastrogaffin, barium meal, and CT scan or upper endoscopy.
Statistical analysis
The statistics measures performed by measuring the average of patients age and the median of their BMI, then we observe patients after surgery and the percentage of each complication measured separately. Many of these complications became an indication for reoperation to remove the band, and the reoperation rate measured from the total cases that underwent the procedure. In this section, the statistical method used to obtain the results of this study is discussed. As a part of this postoperative study, documentation of weight reduction, eating habit and clinical examination performed at every visit. BMI was known as base line, and then weight of patient measured at every clinic visits, so the average of weight reduction at year (j) is computed as
Now, the excess body weight loss for every patient underwent surgery measured and summarized as 1st, 2nd and 3rd year post operation, to delineate the efficiency of gastric band. For example, one of our patients underwent gastric band in 2011, his base line BMI was 42 kg/m², so, the excess BMI was 42-25= 17 kg/m² and his height was 1.5M, the excess body weight equal to 17*1.5*1.5 =38.25kg, then we measure the weight reduction from the excess body weight. After that we documented the weight reduction in percentage for the 1st, 2nd, and 3rd year after surgery.
Results
At King Hussein Medical Center the gastric band performed in female patient seven times more than male, with age average of 28.5 years for both gender. The mean preoperative BMI was 46.07 kg/m².All operations were performed laparoscopically by well-trained bariatric and laparoscopic team, under same circumstances, and the average of operative time was 90 minutes. There was no Conversion rate to open technique.Weight reduction was computed according to equation (2) using the excess body weight measured after the surgery for three consecutive years. The average of weight loss in the 1st year was 40.4%, increased in the following year to 45.12% and then declined to 43.5% in the 3rd year.As shown in following line chart, there is a sufficient weight reduction in the 1st and 2nd year which is started to decline in the 3rd year. (Fig1).Weight reduction curve clinically is not justified. In comparison between the percentage of weight reduction through the 1st, 2nd and 3rd years, there is a dramatic increase in weight reduction in the 1st and 2nd year. This change could be due to patient less
satisfaction of banding, the desire to eat is still present and the band can be adjusted to increase the gastric pouch and allow more caloric intake. In addition, there were many adverse effects that diagnosed during the follow up period, despite the percentages were variable, however the complication rate was significant. About 25% of patients developed complications during postoperative period and 80% of them underwent reopertation for band removal. Five patients discovered to have band slippage by oral gastrografin study and account 2%. While Pouch dilatation diagnosed in a significant proportion of patients, there were 30 patients (12%) discovered endoscopically and radiologically to have pouch dilatation. Five patients had a sever pouch dilatation and returned to theater for band removal ( tow of them reoperated early dilatation after 8 and 9 months and the others developed later dilatation on 22nd ,28th and 34th months respectively after the procedure), and then 13 patients appointed to remove band because of dilatation.Band migration was uncommon complication, occurred in 2% of cases, and diagnosed after 24-48 months after surgery. Since band migration is serious complication, all patients with migration reoperated for band removal. Band erosion occurred in 4 patients; two patients have incomplete erosion and removed surgically, while the other two patients, referred to gastroenterologist for endoscopic band removal due to complete erosion and the band was found completely in the stomach.Hence Gastroesophageal reflux disease is known to be relatively contraindicated for band insertion, all patients underwent gastroscopy before surgery. Gastroesophageal reflux is common complication, and it was the most common cause of patient’s discomfort, an 18 patients suffering from heart burn, which was not present before surgery, most of them respond to Proton pump inhibitors like omeprazol, and only 3 patients reoperated for band removal after tow years of surgery. (Figure 2).
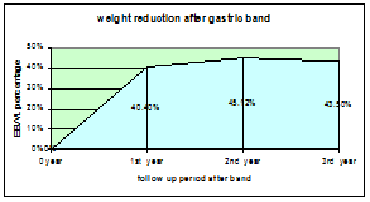
Fig1: line chart demonstrates weight reduction after gastric band
*EBWL, Excess body Weight Loss, 1st,2nd,3rd Year: after surgery
Fig 2: The percentages of Post gastric band complications at KHMC from 2010 till 2016
*P.dilatation : Pouch dilatation, G. erosion: gastric erosion, GERD: Gastroesophageal reflux disease
Band removal
Band removal was performed in a significant proportion of patients, 50 patients (20%) underwent band removal. The most common causes of band removal were Pouch dilatation and patient discomfort. Others due to development of one or more complications as mentioned above.(Fig 3). The rate of reopening after gastric band was 20% and it was only for band removal, the percentage was disappointing and makes the procedure unsuitable bariatric option.
Discussion
The most commonly performed bariatric operations worldwide are sleeve gastrectomy, gastric bypass, and gastric banding. These procedures have been carried out in more than 90% of countries performing bariatric surgery. Adjustable Gastric band as described by Dr. Prem Lobo and his colleague is restrictive procedure performed under laparoscopic technique, to create a small gastric pouch that can tolerate about 20cc fluid or food. (4,5) Initially by introducing Gastric band the early results were excellent, but the long term follow up proofed that many patients became uncomfortable and asked for reversal. By literature review, many prospective studies compare Gastric Banding with gastric bypass or/and Sleeve Gastrectomy. At the same time, a few trials describe the different types of gastric bands (high and low-pressure bands). Also, there are few studies reported data on the complication, and the procedure outcomes. Generally, patient’s outcome after Banding is influenced by the incidence of follow up complications. These include pouch dilatation, slippage, and band migration or erosion as well as incision site complications and esophageal reflux. Furthermore, in the literature, there are only a few studies describe the late complications and long-term results after banding specially with a time period longer than 5 years as published by Dr Michael Korenkov and his colleague in 2012. (5)In our clinical study, the results obtained within 3-7 years of follow up that shows a high complication and reoperation rate. In our experience, most of the patients change their eating behaviors to high calorie intake and sweet, to avoid hungry sensation. In general, an improvement in obesity-related co morbidities was seen in most patients. In our retrospective study with preoperative data collection, the majority of our patients were female, which is similar to study results done by Dr M. Sieb, S. Strasser when the results were disappointing, (6).Post gastric banding complications: By the time, a switch from the perigastric to a pars flaccida technique and using the 2nd generation band, dramatically decline the rate of slippage and pouch dilatation. As noted in tow studies by Dr Michael Korenkov and Dr H. Weiss, F. Aigner in 2012 and 2010 respectively. (5,6) In spite best surgical technique, Pouch dilatation is the most common long-term complication after Gastric Banding leading to band removal according to our study experience. In literature, the incidence of pouch dilatation is influenced by the technique (perigastric versus pars flaccida) and surgical approach (open versus laparoscopic). Most literature proofed that Opening the lesser sac during open band placement leads to a higher incidence of pouch dilatation than the laparoscopic approach. Most Data in the literature describe the rate of pouch dilatation in different manner; because there is variable approach and technique are mostly heterogeneous because most studies include different approaches and techniques. (6,7) Gastric band migration and erosion have silent presentation, in its early phase, as described by Dr Mal Fobi and his colleague (7). Peritonism is usually absent, and there are few retrospective studies obtained from long-term studies available. According to study done in Latvia Riga Stradins University by Dr Andrejs Vanags and his colleague, the incidence of band migration almost similar to our result, starts from 0.6% to 6%. In a few studies, band migration has been considered as a lethal complication that should be diagnosed and managed early. In our data, the patients with band migration and erosion were complaining of dyspepsia, heart burn and epigastric pain, endoscopy showed that gastric wall erosion by the band, the erosion either complete need endoscopic management or partial planned for laparoscopic band removal. (8)By our experience, band migration occurs by 24–48 months postoperatively, which showed near result to Dr W. Ceelen, J. Walder,study. Dr C. Stroh, U. Hohmann state that, the erosion incidence has been shown to increase over the long-term follow-up period, Band erosion may become a life-threatening condition if complicate gastrointestinal bleeding or obstruction. Because of that, early diagnosis and management is crucial. (9,10)Band’s port is surgical device inserted in the abdominal wall to adjust the band by saline and connected to the band by tube. In our study, we did not document any port infection either in early postoperative period or after band filling. In the literature, port infection is encountered to be recognized issue and has been reported to be the initial presentation of erosion and account 0.83%, described by Dr. L.D. MacLean, Dr. N. Christou. The treatment of erosion depends on symptomatology. We advise band removal if symptomatic or in cases of complete erosion using gastroscopy, typical approach described by Dr Ümit Bilge Dogan. (11,12) Repositioning of the gastric band was widely performed at the end of the 1990s, specially in cases of slippage and pouch dilatation, the results was disappointing, all literature data showing more complications with band repositioning as shown by article of Dr C. Stroh, U. Hohmann (9,10). Thus, in cases of slippage and pouch dilatation, most published results and our findings reveal no indication for rebanding, described by Dr Christian Gouillat. (13) Regarding weight reduction, Dr Christian Gouillat & Angélique Denis report an EBWL of 41.1% in the 3rd year after surgery, which conducted as Prospective, Multicenter, 3-Year Trial of Laparoscopic Adjustable Gastric Banding with the MIDBAN,(13). Our results are similar to the mentioned study, but not as the same results observed in study performed by Guy-Bernard Cadière. (14) In our study patients had a higher weight loss, mostly due to the higher preoperative BMI. In comparison to previous data our study showed more weight reduction reaching 43.5%in the 3rd year of follow-up. The intervention rate for reoperation was significantly high; up to 20% of our patients underwent band removal in the following 5 years after surgery. These data are less than literature results, which reported by M. Suter, J. M. Calmes, when the reoperation rate around 50%, PUBLISHED ONLINE MARCH 21, 2011.(14,15,16.17)
Conclusion
Gastric Banding as weight reduction surgery was known to be reversible and safe bariatric procedure, however the band is associated with several complications and high failure rate. This paper endeavored to evaluate the outcomes of Gastric banding as weight reduction surgery at king Hussein medical center, over six years duration. The study was conducted at KHMC and proofed that, gastric band has high reoperation rate for band removal and may complicate many side effects like pouch dilatation and gastric erosion or slippage. Furthermore, to achieve long-term success after bariatric surgery and to avoid complications, lifelong postoperative follow up is required, which is an important concern for obesity surgery.
Strengths and limitations:
This study is the 1st retrospective analysis in Jordan that delineates the gastric band surgery outcomes.
References
1-Kissane Nicole, Janey Pratt, Medical and surgical treatment of obesity, 2011 Mar; 25(1):11-25, PMID: 21516910
2-Schawrtz principles of surgery 10th edition, chapter 27 page 1100.
Charles brunicardi,MD, PhD, 2010.
3-Dr. Hayder Al-Domi, PhD. Asst. Prof. Nut. & Dietetics, University of Jordan 2010 Obesity Pandemic in Jordan out of Control: The Nexus Between Eating Practices & Physical Activity,
4-Dr. Prem Lobo, Adjustible Gastric Band, Sydney NSW, Holly Edmond, NC 28079, Greg Eden, Aukland 1130. www.yourpracticeonline.net
5-Michael Korenkov , Wendy A. Brown, Adjustable Gastric Banding. Springer 2012, ISBN 978-3-642-16244-2.
6-Sieb.M, Stefan Strasser, H. Weiss, F. Aigner, and H. Nehoda, “Disappointing mid-term results after lap gastric banding in young patients,” Surgery for Obesity and Related Diseases. Published online 2010 Dec 22. doi: 10.1155/2011/128451.
7-Mal Fobi, MD; Hoil Lee, MD; Band Erosion: Incidence, Etiology, Management and Outcome after Banded Vertical Gastric Bypass,Center for
Surgical treatment of Obesity, Hawaiian Gardens; Tri-City Regional Hospital, Los Angeles, CA, USA, Obesity Surgery, 11, pp-pp.
8-Andrejs Vanags, Ilze Strumfa, Maris Pavars,: Intragastric Migration of Swedish Adjustible Gastric Band, Clinical University Hospital, Riga, Latvia Riga Stradins University, Latvia. DOI: 10.2478/v10163-010-0021-6.
9-Wim Ceelen, Julio Walder, “Surgical treatment of severe obesity with a low-pressure adjustable gastric band: experimental data and clinical results in 625 patients,” PMC1513977.
10-C. Stroh, Hohmann.U, Will et al., “Experiences of two centers of bariatric surgery in the treatment of intragastrale band migration after gastric banding—2005 and 2006,” International Journal of Colorectal Disease, 2008. Article ID 128451.
11-Dr. L.D. MacLean, Dr. N. Christou, Canada 2004, The gastric band procedure evaluation , Report number 15, This analysis was prepared for the Technology Assessment Unit (TAU) of the McGill University Health Centre (MUHC).
12- Ümit Bilge Dogan, MD, Mustafa Salih Akin, MD, Serkan Yalaki, MD. Endoscopic management of gastric band erosions: A 7-year series of 14 patients., Turkey, DOI: 10.1503/cjs.001313.
13-Christian Gouillat & Angélique Denis & Perrine Badol-Van Straaten ,Prospective, Multicenter, 3-Year Trial of Laparoscopic, Adjustable Gastric Banding with the MIDBAND.OBES SURG, DOI 10.1007/s11695-011-0508-9.
14-Jacques Himpens, MD; Guy-Bernard Cadière, MD, PhD; Michel Bazi, MD Long-term Outcomes of Laparoscopic Adjustable Gastric Banding.ARCH SURG PUBLISHED ONLINE MARCH 21, 2011.
15- Gustavsson and A. Westling, “Laparoscopic adjustable gastric banding: complications and side effects responsible for the poor long-term outcome,” 2002, SURG INNOV June 2002 9: 115-124.
16-Michel Suter, J. M. Calmes, “A 10-year experience with laparoscopic gastric banding for morbid obesity: high long-term complication and failure rates,” , 2006. PMID:16839478.
17-Jong Seob Park, Sang-moon Han, Feasibility and safety of conversion sleeve gastrectomy after failed primary adjustable gastric band or sleeve gastrectomy.JMBS, J Metab Bariatr Surg 2016; 5(2): 62-66.Published online: 30 December 2016.