ABSTRACT
Objective: The aim of our study is to identify the frequency of different Hepatitis C Virus (HCV) genotypes in hepatitis C virus infected patients at King Hussein Medical Center, Jordan and to find out the association of genotypes with HCV-RNA viral load, age and gender.
Methods: Our study was conducted at Princess Iman Center for research and laboratory sciences King Hussein Medical Center, Jordan in a retrospective manner in the period between January 2018 and September 2018.A total of 187 patients who attended gastroenterology clinics were included in our study with age range between 12 years and 72 years, 47 % (88) of which male and 53% (99) female. From each patient 10 ml blood were collected using yellow top gel tube for detection of both HCV-Ab and HCV-RNA. HCV-RNA concentration was analyzed by real time polymerase chain reaction and genotyped by reverse-hybridization method.
Results: Of the 128 patients with positive anti-HCV antibodies, all (100%) were positive for HCV-RNA by real time polymerase chain reaction. The overall genotype frequency showed that 92 (49.2%) was identified as genotype 1; 78 (41.7%) genotype 4; eight (4.3%) genotype 2; six (3.2%) genotype 3, two (1.06%) genotype 6 and 1(0.54%) genotype 5. Subtype 1a was the most prevalent among patients, followed by 4c/d, 4a, 1b, 3a, 2b, 2a, 4h and equally 5a, 6g, 6f.Genotype 4 was the most frequent in 50-59 years (19 of 33) and 12-19 years (six of nine). Genotype 1 was the most prevalent in other patient age categories 40-49 years (16 of 22), 20-29years (20 of 37) and 30-39 years (28 of 55).Genotype 5a, 6g and 6f were the least common and each found with 0.54% frequency. The frequency of genotypes 1, 4, 2, 3 and 6 in male was 22.4%, 21.2%, 1.6%, 1.06%, 0.54% respectively. in female the frequency of genotypes 1, 4, 2, 3, 5 and 6 was 26.5%, 20.26%, 2.64%, 2.1%, 0.54%, 0.54% respectively.
Conclusion: Our study showed HCV genotypes 1and 4 were the most frequent genotype, and comprise over 89% of all HCV infection. Genotype 1 was more frequently associated with intermediate or high viral load, whereas genotype 4h and 6g less frequent and associated with low viral load. Further study at a larger scale is recommended as well as clinical and lab correlations are warranted.
Key words: Frequency, HCV genotype, Jordan
JRMS December 2018; 25(3):50-57/ DOI: 10.12816/0052733
Introduction
Hepatitis C virus (HCV) is an enveloped virion containing a genome of single-stranded, positive-polarity RNA and it is a member of the flavivirus.(1) Infection caused by HCV is a widely spread and important health problem world wide. The frequency of HCV was 3.3% (200 million) of the world population as per world health organization reports.(2) About 170 million are chronic hepatitis C carrier, and in the USA between 60% and 85% develop chronic hepatitis C infection, which is leading to end stage liver disease (cirrhosis, hepatocellular carcinoma) and liver transplantation.(3) The sero frequency of HCV in Jordan was 0.6-6.25%, when compared to the corresponding populations in surrounding countries like Iraq (3.2%), Syria (1%), Lebanon (0.7-1%),Gaza strip (2.2%), and Egypt (13-22%); the frequency is convergent.(4) Other studies conducted in Jordan showed the frequency of HCV was 7.7% and 0.42%.(5,6) HCV infection is transmitted through blood contact like intravenous drug usage, reused needles, poorly sterilized surgical and dental equipment, and blood transfusion.(7) Variability of disease progression depends on several factors such as gender, age at infection, viral load and mode of infection, and genotype/subtype. The outcome of antiviral therapy in patients infected with HCV correlates with important predictors factors such as clinical findings, genotypes and viral load.(8) Depending on genomic sequences of HCV, six genotypes and a series of subtypes (a, b, c,…) have been identified, and they have different prevalence that vary from one geographic area to another. (9) HCV genotypes 1, 2, 3, are worldwide distributed, whereas genotypes 4, 5, 6, in a certain geographic areas of the world. (10) HCV genotype 1 is the most frequent worldwide (46% of all HCV infection), followed by genotype 3 (22%), and genotypes 2, 4 (each for 13%).(11) In Europe, genotype 1b is the most prevalent; in north America genotype 1a predominates; genotype 2 is most frequent in many developed countries; genotype 3a prevalent in north America and united kingdom in injected drug users; genotype 4, 5 are found in middle east, north and central Africa; genotype 6 is most frequent in south-east Asia.(12) Regarding Arab countries, genotype 4 is most frequent in Arabian Peninsula region, genotype 1a most frequent in Jordan, genotype 4 in Egypt, Sudan, Iraq, Syria, Lebanon and Gaza strip. (4) Study conducted in Greece found relationship between age and sex and the frequency of HCV genotype; genotype 1 was more common in older people and women, whereas genotype 3 was more common in younger patients and men. (13) The concentration of HCV (viral load) identified by PCR was higher in patient with genotype 1when compared with genotype 2 and 3. (14,15) Another relationship between HCV genotype and response to antiviral therapy present, the genotype 1b and 4 has a poor response to interferon, whereas in patients with genotype 2 and 3 found better response to treatment. (9) The aim of our study is to identify the frequency of different HCV genotypes in a Jordanian cohort according to age and gender and to elucidate the association between different HCV genotypes and viral load.
Methods
Our study was conducted at Princess Iman Center for Research and Laboratory Sciences-King Hussein Medical Center (KHMC) in a retrospective manner in the period between January 2018 and September 2018.The study was approved by Human Research Ethics Committee of the Royal Medical Services, Amman-Jordan. A total of 187 patients who attended gastroenterology clinics in KHMC, were included in our study, with age range between 12 years and 72 years, 47 % (88) of which male and 53% (99) female. Only patients whom showed positive tests for HCV antibodies by electro generated chemiluminescence (ECL) immunoassay and HCV-RNA by real time polymerase chain reaction (PCR) were included in the study. From each patient 10 ml blood was collected using yellow top gel tube for HCV-Ab and HCV-RNA detection. (ECL) immunoassay used to detect HCV antibodies by cobas 6000 analyzer (Roche Diagnostics, USA). The cobas 6000 analyzer series combined, the cobas e 601 analyzer for immunoassay and the cobas c 501 analyzer for biochemical testing, into a single integrated system (Figure1).(ECL) immunoassay is highly sensitive and specific. The controls and calibrators were included with each run. HCV-RNA was isolated from HCV-antibody positive samples using QIA amp viral RNA Mini Kit following instructions of manufacturer (QIAGEN-Germany).Quantitative detection of HCV pathogen by reverse transcriptase polymerase chain (RT-PCR) is based on the amplification of specific regions using Rotor-Gene Q thermocycler. Internal and external controls were included in each run to identify possible PCR inhibition and determination of viral RNA respectively. The analytical detection limit is 33.6 IU/ml. The sensitivity of the test is 95%, whereas the specificity 100%. HCV genotyping test is based on reverse-hybridization principle. 10 microliters biotinylated amplification product that generated by RT-PCR is hybridized to specific probes that are bound to nitrocellulose strips using GEN-C 2.0 kit, according to the manufacturer’s instructions (NLM diagnostics, Italy).The test allows identification of types 1(1a, 1b subtypes) and 2 (2a, 2b); type 3 (subtypes 3a, b, c, k); and type4 (subtype 4a, b, c/d, e, f, h); type 5(5a subtype); and type 6 (6a/6b, g, f, q, m). The sensitivity and specificity of HCV genotyping test were 100%.

Fig 1: Cobas® 6000 analyzer series.
Results
Among 187 patients with positive anti-HCV antibodies, all (100%) were positive HCV-RNA by RT-PCR. According to HCV-RNA viral load, patients divided into three groups: group A (n=71, 37.9%) with low viral load (less than 200,000 IU/ml), group B (n=42, 22.5%)-intermediate (200,000-600,000 IU/ml) and group C (n=74, 39.5%) - high (more than 600,000 IU/ml) (Figure 2). The overall genotype frequency showed that 92 (49.2%) was identified as genotype 1; 78 (41.7%) genotype 4; 8 (4.3%) genotype 2; 6 (3.2%) genotype 3, 2(1.06%) genotype 6 and 1(0.54%) genotype 5.Subtype 1a was the most prevalent among patients, followed by 4c/d, 4a, 1b, 3a, 2b, 2a, 4h and equally 5a, 6g, 6f (Table I). In order to compare the frequency of HCV genotype/subtype according to age, patients were categorized into groups with 10 years intervals as seen in (Table II). Association with age showed that HCV was most prevalent in patients aged 30-39 years followed by those aged 20-29 years and 50-59 years. Genotype 4 was the most frequent in 50-59 years (19 of 33) and 12-19 years (6 of 9). Genotype 1 was the most prevalent in other patient age categories 40-49 years (16 of 22), 20-29 years (20 of 37) and 30-39 years (28 of 55). This mean that patients with age less than 20 years and older 50 years are more frequently infected with HCV-genotype 4 and patient's age (20-49 years old) more frequently infected with HCV-genotype 1. Genotype 5a, 6g and 6f were the least common and each found with 0.54% frequency. The frequency of genotypes 1, 4, 2, 3 and 6 in male was 22.4%, 21.2%, 1.6%, 1.06%, 0.54% respectively. in female the frequency of genotypes 1, 4, 2, 3, 5 and 6 was 26.5%, 20.26%, 2.64%, 2.1%, 0.54%, 0.54% respectively(Table III). Genotype 6g, 5a and 4h were found only in females, whereas genotype 6f found in male. Males in comparison with females were slightly more frequently infected with genotype 4; whereas females with genotype 1, 2 and 3 (figure 3). Finally, according to the association of genotype and HCV-RNA viral load, the majority of infected patients with genotype 2 (5/8, 62.5%), genotype 3a (4/6) and genotype 1 (60/92, 65.2%) had an intermediate or high viral load more than 2x105 IU/ml. For genotype 4 (44/78, 56.4%) had a viral load more than 2x105 IU/ml and (34/52, 43.6%) less than 2x105 IU/ml. Subtypes 1a and 4c/d were the most prevalent in patients with low viral load (14.4% and 12.8% respectively). In another side, genotype 1a (13.3%) and 4a (8.5%) were the most frequent in the patients with high viral load. Genotype 4h, 5a, 6g and 6f were found in patient category with high viral load with frequency rate 1.06%, 0.54%, 0.54% and 0.54%respectively (Table IV).
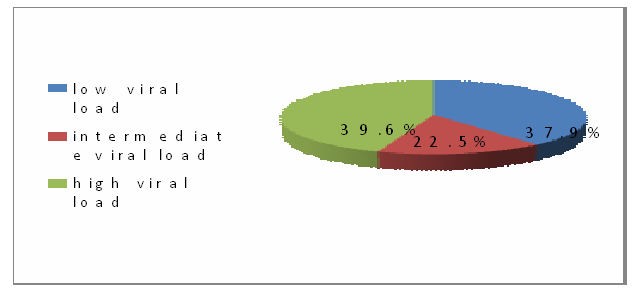
Fig 2: Frequency of HCV-RNA viral load groups.
Table I: Frequency of subtypes in all patients.
|
Subtype
|
Number
|
Percentage (%)
|
|
1a
|
66
|
35.3%
|
|
1b
|
26
|
13.9%
|
|
2a
|
3
|
1.6%
|
|
2b
|
5
|
2.7%
|
|
3a
|
6
|
3.2%
|
|
4a
|
35
|
18.7%
|
|
4c/d
|
41
|
21.9%
|
|
4h
|
2
|
1.07%
|
|
5a
|
1
|
0.54%
|
|
6g
|
1
|
0.54%
|
|
6f
|
1
|
0.54%
|
|
Total
|
187
|
100%
|
Table II: Frequency of HCV genotypes/subtypes according to age.
Age group
|
Age
group
(years)
|
1a
|
1b
|
2a
|
2b
|
3a
|
4a
|
4c/d
|
4h
|
5a
|
6g
|
6f
|
Total
|
|
12-19
|
0
|
0
|
0
|
1
|
1
|
3
|
3
|
0
|
0
|
1
|
0
|
9
|
|
20-29
|
15
|
5
|
1
|
0
|
0
|
8
|
7
|
1
|
0
|
0
|
0
|
37
|
|
30-39
|
19
|
9
|
1
|
1
|
3
|
11
|
10
|
0
|
0
|
0
|
1
|
55
|
|
40-49
|
14
|
2
|
0
|
1
|
1
|
3
|
1
|
0
|
0
|
0
|
0
|
22
|
|
50-59
|
7
|
6
|
0
|
1
|
0
|
4
|
14
|
1
|
0
|
0
|
0
|
33
|
|
60-72
|
11
|
4
|
1
|
1
|
1
|
6
|
6
|
0
|
1
|
0
|
0
|
31
|
|
Total
|
66
|
26
|
3
|
5
|
6
|
35
|
41
|
2
|
1
|
1
|
1
|
187
|
Table III: Distribution of HCV genotype according gender.
|
Genotype/
subtype
|
Male
|
Female
|
|
Frequency
|
Percentage
|
Frequency
|
Percentage
|
|
1
|
42
|
22.4%
|
50
|
26.5%
|
|
1a
|
35
|
18.7%
|
31
|
16.5%
|
|
1b
|
7
|
3.7%
|
19
|
10%
|
|
2
|
3
|
1.6%
|
5
|
2.64%
|
|
2a
|
2
|
1.06%
|
1
|
0.54%
|
|
2b
|
1
|
0.54%
|
4
|
2.1%
|
|
3
|
2
|
1.06%
|
4
|
2.1%
|
|
3a
|
2
|
1.06%
|
4
|
2.1%
|
|
4
|
40
|
21.2%
|
38
|
20.26%
|
|
4a
|
19
|
10%
|
16
|
8.5%
|
|
4c/d
|
21
|
11.2%
|
20
|
10.7%
|
|
4h
|
0
|
0%
|
2
|
1.06%
|
|
5a
|
0
|
0
|
1
|
0.54%
|
|
6
|
1
|
0.54%
|
1
|
0.54%
|
|
6g
|
0
|
0
|
1
|
0.54%
|
|
6f
|
1
|
0
|
0
|
0
|
|
Total
|
88
|
46.74%
|
99
|
52.84%
|
Table IV: HCV viral load distribution in genotypes.
|
Genotype
|
Viral load (IU/ml)
|
Total
|
|
|
˂ 200.000
|
200.000-600.000
|
> 600.000
|
|
|
1
|
32(17.2%)
|
21 (11.2%)
|
39 (20.8%)
|
92
|
|
1a
|
27 (14.4%)
|
13(6.9%)
|
25(13.3%)
|
|
|
1b
|
5 (2.8%)
|
8 (4.3%)
|
14 (7.5%)
|
|
|
2
|
3(1.60%)
|
1 (0.54%)
|
4 (2.12%)
|
8
|
|
2a
|
1(0.54%)
|
0
|
2 (1.06%)
|
|
|
2b
|
2(1.06%)
|
1 (0.54%)
|
2 (1.06%)
|
|
|
3
|
2 (1.06%)
|
2 (1.06%)
|
2 (1.06%)
|
6
|
|
3a
|
2 (1.06%)
|
2 (1.06%)
|
2 (1.06%)
|
|
|
4
|
34 (18.1%)
|
18(9.6%)
|
26 (13.9%)
|
187
|
|
4a
|
10(5.3%)
|
9 (4.8%)
|
16 (8.5%)
|
|
|
4c/d
|
24(12.8%)
|
9 (4.8%)
|
8 (4.2%)
|
|
|
4h
|
0 (0%)
|
0 (0%)
|
2 (1.06%)
|
|
|
5a
|
0
|
0
|
1(0.54%)
|
1
|
|
6
|
0 (0%)
|
0 (0%)
|
2 (1.06%)
|
2
|
|
6g
|
0 (0%)
|
0 (0%)
|
1 (0.54%)
|
|
|
6f
|
0
|
0
|
1(0.54%)
|
|
|
Total
|
71 (37.9%)
|
42 (22.5%)
|
74(39.6%)
|
187
|
Fig 3: Genotypes in male and female
Discussion
In our study, the frequency of HCV genotypes and association with patient’s age, gender and viral load were analyzed. Our results show that the genotype 1 was the most frequent (49.2%) followed by genotype 4 (41.7%). In 2002, Bdour studies HCV genotyping in a couple of Jordanian hospitals hemodialysis units and showed genotype 1 was the most prevalent one. (16) A global modeling study conducted in center for disease analysis (USA) with contribution from The Polaris Observatory HCV Collaborators for analyzing prevalence and genotype distributions of HCV infection worldwide showed frequency of HCV genotype 1 and 4 in Jordan 42.3% and 57.7% respectively. (17) Study about hepatitis C infection in Arab world by Mohamed A.D et al reported that the dominant subtype in Jordan was 1a, which is in keeping with our results that show 35.3% frequency rate of subtype 1a. (4) Gamal Esmat study shows the most frequent genotype in middle east Arab countries (except Jordan) was genotype 4, whereas in Jordan the subtype 1a was the dominant (40%), followed by 1b (33.3%) and 4 (26.6%).(18) Globally HCV genotypes prevalence was 46%, 22%, 13%, 13%, 2%, 1% for genotype 1, 3, 2,4,6, 5 respectively.(19) According to the mentioned results in Middle East countries there is no significant disparity between our results and others except for a study conducted in Qatar by Mahmud and his colleagues which showed the most prevalent genotype in Jordan is 4 with 77% followed by genotype 1 (22.8%) which might be due to a small sample number (71) comparing with our study (187).(20) Age related analysis of HCV genotypes distribution revealed that genotype 1 was more frequent in middle age infected patients (20-49 years), whereas genotype 4 in patients with age less than 20 years and those older than 50 years. Saba et al study conducted in Pakistan reported that genotype 3a was the most prevalent in all age groups; genotype 3b and 1a were highest among the 40-49 years old. (21) Another study from Italy shows genotype 2 was more common in the over 60-year age group, in the other hand genotype 3 was more prevalent in younger patients under 35 years age. (22) Regarding association of genotype with gender our results showed no significant difference between males and females. Males were slightly more frequently infected with genotype 4 (21.2%-male, 20.26%-female) whereas females more infected with genotype 1(26.5%-female, 22.4%-male). Female more frequently infected with genotype 2 and 3 (1.6%-male, 2.64%-female; 1.06%-male, 2.1%-female respectively). In agreement with our results no significant difference was seen by Amjad A et al (23). In China ZhiLi N et al reported that genotype 1 and 2 were more common in female patients than males. (24) Another study in Italy shows no statistical variation in the gender distribution for genotype 1 and 2, though subtype 1b was more common among females and genotype 3 was more frequent in males than females. (22) The association of HCV genotype and viral load we found that 60 0f 92 HCV genotype 1 infected patients have an intermediate or high viral load. Subtypes 1a and 4c/d were the most frequent in a group of patients with low viral load. Genotype 4 frequency in low viral load category and intermediate or high viral load categories was 18.1% and 23.5% with no significant variation. We found those genotypes 4h, 5a, 6g and 6fassociated only with high viral load. Anita C et al, Arnolfo P et al and Georges Pet al reported that viral load in patients infected with genotype 1 was significantly high. (14,22,25) Our study was limited by the sample number and clinical and pathological correlation was not included. Large scale prospective studies at institutional and national levels are recommended to figure out the prevalence of difference HCV genotypes in Jordan along with inclusion of clinical and pathological data.
Conclusion
Our study showed HCV genotypes 1and 4 were the most frequent genotype, and comprise over 89% of all HCV infection. Genotype 1 was more frequently associated with intermediate or high viral load, whereas genotype 4h and 6g less frequent and associated with low viral load. Further study at a larger scale is recommended as well as clinical and lab correlations are warranted.
References
1.Kayser FH, Beinz KA, Eskert Jet al. Medical microbiologybook 10th ed. 2005. Chapter 8, page 442-445.
2.Athar MA, XuY, Xie X et al. Rapid detection of HCV genotyping 1a, 1b, 2a, 3a, 3b and 6a in a single reaction using two-melting temperature codes by a real-time PCR-based assay. Journal of Virological Methods 2015; 85–90.
3.Thomas LB, FoulisPR, Mastorides SM et al.Hepatitis C Genotype Analysis: Results in a Large Veteran Population with Review of the Implications for Clinical Practice. Annals of Clinical & Laboratory Science 2012; v. 42; no. 4; p 355-362.
4.Daw MA,Dau AA. Hepatitis C Virus in Arab World: A State of Concern. The Scientific World Journal 2012; doi:10.1100/2012/719494.
5.Faris NS. Prevalence of hepatitis C and hepatitis B, prevention and immunization.Standard Scientific Research and Essays 2013; V.1; n.4: p 68-71.
6.Hamoudi W, Sheikh Ali SA, Abdallat M et al.HCV infection prevalence in a population recruited at health centers in Jordan. Journal of Epidemiology and Global Health 2013; v.3; p 67– 71.
7.Elgharably A, Gomaa AI, Crossey MM et al.Hepatitis C in Egypt – past, present, and future. International Journal of General Medicine 2017; v.10; p 1-6.
8.Nabi SG, Zaffar G, Sheikh NI et al. Hepatitis C virus genotypes: A plausible association with viral loads. Indian journal of pathology and microbiology2013; v.56; p 384-387.
9.Re V, Lampe E,Yoshida CF et al. hepatitis C virus genotypes in Cordoba, Argentina, unexpected high prevalence of genotype 2. MEDICINA (Buenos Aires) 2003; v.63; p 205-210.
10.Nouroz F, Shaheen S, Mujtaba G et al. An overview on hepatitis C virus genotypes and its control. The Egyptian Journal of Medical Human Genetics 2015; V.16; p 291–298.
11.Nyan DC, Swinson KL. A method for rapid detection and genotype identification of hepatitis C virus 1–6 by one-step reverse transcription loop-mediated isothermal amplification. International Journal of Infectious Diseases 2016; v.43; p 30–36.
12.Qattan I,Emery V. Hepatitis C virus genotyping in chronic hepatitis C patients. European Scientific Journal 2012; v.8; n. 27.
13.Raptopoulou M, Touloumi G, Tzourmakliotis D et al. Significant epidemiological changes in chronic hepatitis C infection: results of the nationwide HEPNET-GREECE cohort study. HIPPOKRATIA 2011; v.15; n. 1; p 26-31.
14.Chakaravarti A, Dogra G, Verma V et al. Distribution pattern of HCV genotypes & its association with viral load. Indian J Med Res 2011; v.133; p 326-331.
15.Lee H, Kyung Cho Y, UpKim H et al.Distribution of hepatitis C virus genotypes in Jeju Island. Korean Journal of Hepatology 2008; V.14; n.1.
16.Bdour S. Hepatitis C virus infection in Jordanian hemodialysis units: serological diagnosis and genotyping. J. Med. Microbiol 2002; v.51, pp 700–704. doi: 10.1099/0022-1317-51-8-700.
17.Razavi H. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: a modelling study. www.thelancet.com/gastrohep Vol 2 March 2017.
18.Esmat G. Hepatitis C in the Eastern Mediterranean Region. Eastern Mediterranean Health Journal 2013; v.19; n.7.
19.ower E, Estes C, Sarah B et al.Global epidemiology and genotype distribution of the hepatitis C virus infection. Journal of Hepatology 2014; v.61.
20.Mahmud S, Alkanaani ZK, ChemaitellyH et al.Hepatitis C virus genotypes in the Middle East and North Africa: Distribution, diversity, and patterns. J Med Virol. 2018; v.90: n.; pp 131–141.
21.Riaz S, Bashir MF, Haider S et al. Association of genotypes with viral load and biochemical markers in HCV-infected Sindhi patients. Brazilian Journal of Microbiology 2016; v.87; n.4.
22.Petruzziello A, Coppola N, Loquercio G et al. Distribution Pattern of Hepatitis C VirusGenotypes and Correlation with Viral Load and Risk Factors in Chronic Positive Patients. Intervirology 2014; v.57; p 311–318.
23.Ali A, Nisar M, Ahmad H et al. Determination of HCV genotypes and viral loads in chronic HCV infected patients of Hazara Pakistan. Virology Journal 2011; v.8:466.
24.Niu Z, Zhang PA, Tong YQ. Age and gender distribution of HepatitisC virus prevalence and genotypes of individuals of physical examination in WuHan, Central China. Springer Plus (2016) 5:1557.
25.Pageaux GP, Ducos J, MondainAM et al. Hepatitis C Virus Genotypes and Quantitation of Serum Hepatitis C Virus RNA in Liver Transplant Recipients: Relationship With Severity of Histological Recurrence and Implications in the Pathogenesis of HCV Infection.Liver Transplantation and Surgery 1997;v.3; n.5; p 501-505.