ABSTRACT
Objective: To review the indications for invasive prenatal diagnostic procedures performed at the Royal Medical Services between the years 2013-2017 and to look at miscarriage rates related to these procedures.
Methodology: This retrospective review was carried out on 943 pregnant women at the Fetal Medicine unit who underwent invasive procedures at King Hussein Medical Centre, Amman, Jordan in the period between February 2013 and December 2017. This is the only unit for fetal medicine at the Royal Medical Services. Invasive procedures were performed between 11 to 28 weeks gestations and the outcomes were reviewed
Results: After analyzing the results of amniocentesis (AC) and chorionic villous sampling (CVS), the indications were as follows: Advanced age> 37 years {n=300, 31.8%}, family history of abnormal offspring {n = 237, 25.1%}, abnormal soft tissue marks on ultrasound abnormal integrated test {n = 200, 21.2%} and abnormal ultrasound findings {n = 206, 21.8%} .Total number of abnormal karytyping [n = 72, 7.6%}. The number of amniocentesis was 705 procedures constituting 74.7% of all procedures and the number of CVS’s was 238 constituting 25.2% of all procedures. . Miscarriage rates after amniocentesis was 0.3% and CVS was 1.3%.
Conclusion: At King Hussein Medical Centre, the most common method of invasive procedure is amniocentesis followed by CVS. Advanced maternal age is the most common indication for invasive prenatal procedures. Miscarriage rates are consistent with what is reported in the literature.
Key words: Advanced maternal age, Amniocentesis, Chorionic villious sampling, Prenatal diagnosis.
JRMS Dec 2018; 25(3):58-65/ DOI: 10.12816/00534
Introduction
Chorionic villus sampling CVS is an ambulatory outpatient procedure usually performed at tertiary centers to obtain samples of the placenta for genetic diagnosis. The procedure can be carried out trasvaginally or transabdominally under ultrasound guidance. Chorionic villus sampling is performed between 10 and 14 weeks of gestation by skilled and experienced operator.
The procedure should be avoided before 10 weeks as it can increase the incidence of facial and limb defect (1,2) and most abortions would have occurred before this time. It is also difficult to perform before this gestational age. It is associated with a small risk of culture and risk of mosaicism. (2) Amniocentesis is an alternative to CVS to obtain amniotic fluid which contains fetal cells for culturing and karyotyping. It is performed transabdominally under US guidance and is considered the most popular invasive procedure which should be done after completed 15 weeks of gestation. Early amniocentesis is associated with culture failure and fetal loss so it is better to avoid it (3). The main indications for genetic diagnosis include advanced maternal age, previous abnormal child, and family history of congenital abnormality as discussed in several studies (4). Other indications include abnormal US finding and soft tissue markers at aneuploidy screen. The most serious complication of CVS and amniocentesis is fetal loss which is reported around 1%. (4, 5)The objective of the study is to study the trends in indications for invasive prenatal diagnostic procedures, and ultimately to look at the rate of miscarriages as an end point complication of the procedures performed and to compare the results to what has been reported in the literature.
Method
Women were referred to the Fetal Medicine Unit for invasive prenatal testing for a variety of reasons which include the followings:
1. Advanced maternal age (AMA); age of the pregnant women 37 years and above
2. Family history of congenital abnormalities and/or history of abnormal offspring
3. Abnormal US findings; Polyhadraminos, IUGR, Cystic hygroma, Renal abnormalities, CNS abnormality, and others
4. Abnormal integrated tests; first trimester (PAPP-A and nuchal translucency) and second trimester (serum AFP, UE3,beta_hCG,inhibin A)
5. Soft tissue markers of aneuploidy on scan
6. Family history of Down syndrome
7. Increased nuchal translucency ( NT )
Women are counseled regarding the available diagnostic procedures- the pre-test counseling- when the nature of the procedure, risks and benefits are outlined when a detailed informed consent is taken. Invasive prenatal diagnostic procedures performed in this hospital include amniocentesis, chorionic villus sampling and cordocentesis. The procedures are all performed by a group of three consultant practitioners. However, cordocentesis procedures have been excluded from this review due to small numbers and varying levels of operator experience. Over a period of 5 years 943 Jordanian women underwent diagnostic prenatal procedures in the tertiary center of fetal medicine at King Hussein Hospital, Royal medical services which is considered a referral center to all military hospitals in Jordan. This is a retrospective review of all invasive procedures between 2013 and 2017. All patients who underwent CVS for thalassaemia and all patients who underwent molecular DNA testing and their samples which were sent outside Jordan for analysis were excluded from our study. The first trimester screen which involves calculating the risk of having a baby with Down syndrome involves B-HCG, PAPPA, Nuchal translucency and maternal age is not offered at our center. Patients who are interested in doing the test are asked to go to a private laboratory to have it done. None invasive prenatal diagnosis is not offered at our centre and all tests were done privately. Procedures performed included amniocentesis done after 15 weeks and CVS done between 11-14 weeks respectively which were done by 3 experienced consultants. Cordocentesis procedures were excluded from the study due to the lack of experience of certain consultants in this procedure and due to the increased risk of miscarriage associated with it compared to other procedures. (6) If, after appropriate reflection and consideration, the women then elect to undergo an invasive procedure. The procedures were performed under US guidance and aseptic technique using transabdominal approach only, using a spinal needle G 18-20 for amniocentesis and G18 for CVS. Prophylactic antibiotic was not prescribed. Local anesthesia was given only to patients who underwent CVS. All patients were given appointments to be seen in clinic in one week after the procedure to discuss the early results and to follow up results and to assess complications. Following the procedures, the patients were asked to notify the center should any sign or symptom of complications appear. All procedures were recorded in a specific form which was divided into two parts, one was filled in the clinic which included the maternal age, parity, gestational age, indication for the procedure, procedure performed, test requested, any complication at the time of the procedure and the presence of a positive fetal heart at the end of the procedure. Anti D immunoglobulin was prescribed and administered to all rhesus negative women. The second part is filled at the laboratory which includes the results and saving the data into a specialized registry for follow up and auditing purposes.
The study was approved by our local ethical committee at the Royal Medical Services.
Results
This study was conducted in the fetal medicine unit at King Hussein Medical Hospital where diagnostic procedures were done by 3 operators at a rate of 60 cases annually each. This is above the standard rate (usually around 30 cases per year as recommended by the RCOG). (7) The maximum number of procedures was done in 2016 where the number of cases was 211; on the other hand, the lowest number of procedures was in 2017 reaching 166 cases as shown in (Chart 1). (Chart 2) shows the number of abnormal cytology detected at our unit, showing the highest at 25 cases in 2014 and the lowest at 8 cases in 2013. (Fig 1) shows the type of abnormalities detected over a 5 years period where the maximum number is 29 cases of Down syndrome. (Figure 2) shows indications of procedures annually between 2013 and 2017. (Table I ) compares the percentage of CVS cases to AC throughout the five years showing a roughly three-fold prevalence of AC at 74.7% over CVS at 25.2%. (Table II) compares the percentage rate of miscarriage associated with both procedures over five year's period. The percentage of miscarriage occurrence with CVS is at 1.26% compared to miscarriage rate of 0.28% for AC. (Table III) shows the frequency of the abnormalities detected in relation to the indication of procedure.
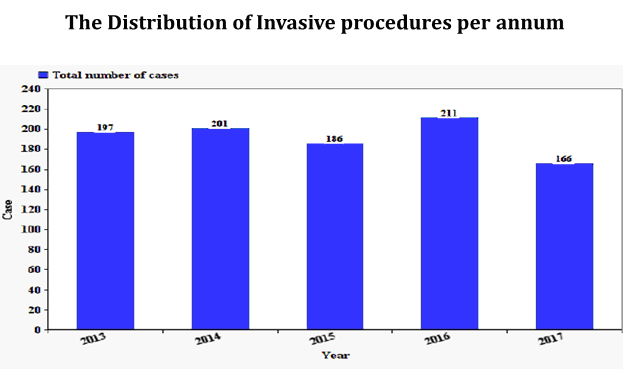
Chart 1: Number of procedures done per annum.
Chart 2 Shows the number of abnormal cytology detected at our unit.
|
Case
|
Number
|
|
Trisomy 21
|
29
|
|
Trisomy 18
|
20
|
|
Trisomy 13
|
06
|
|
Turner syndrome
|
09
|
|
Triploidy
|
05
|
|
Klinefelter syndrome
|
03
|
Fig 1: Type of abnormalities detected over 5 years period
Fig 2: Shows indications of procedures annually between 2013 and 2017.
Table I: compares the percentage of CVS cases to AC throughout the five years showing a roughly three-fold prevalence of AC at 74.7% over CVS at 25.2%.
|
Procedure
|
Number
|
Percentage
of procedures
|
|
Chorionic Villous sampling
|
238
|
25.2
|
|
Amniocentesis
|
705
|
74.7
|
|
Table II: compares the percentage rate of
miscarriage associated with both procedures over five years period. The
percentage of miscarriage occurrence with CVS is at 1.26% compared to
miscarriage rate of 0.28% for AC.
|
Procedure
|
Number
|
Miscarriages
|
Percentage
|
|
Chorionic
Villous sampling
|
238
|
3
|
1.26
|
|
Amniocentesis
|
705
|
2
|
0.28
|
| |
|
Table III: Shows the frequency of the
abnormalities detected in relation to the indication of procedure
|
|
Total Number of Abnormality Detected According
to Indicator
|
Number of Abnormalities
|
Percentage of Abnormality
|
|
Advanced maternal age
(AMA)
|
27
|
37.%
|
|
Abnormal ultrasound
findings
|
20
|
28%
|
|
Family history
|
12
|
17%
|
|
Previous history of
down syndrome
|
13
|
18%
|
Discussion
Our fetal medicine unit is part of the obstetrics and Gynaecology Department at King Hussein Medical Centre. We have around 12000 deliveries per year at our hospital. We get referrals from all peripheral hospitals and the private sector. The caesarean section rate at our hospital is around 40% which is high but our hospital is a tertiary centre. This is the first audit done at the centre regarding the indication, results and the outcome of invasive procedures. A total number of 943 women were involved in the study over a period of 5 years with an average of 188 procedures done a year (around 62 procedures per operator) which is in excess to the standard set by the expert committee of the Royal College of Obstetricians and Gynecologists (7). The most common procedure done by far with 3 fold prevalence is amniocentesis as compared to CVS which accounts for 25.2 percent of the procedures done over the five years interval. All our patients were insured at our hospital and all tests were done at our hospital for free. The maximum number of procedures was done in 2016 where the number of cases was 211; on the other hand the lowest number of procedures was in 2017 reaching 166 cases as shown in (Chart 1). All tests were analyzed at our cytogenetic Lab. (Chart 2) shows the number of abnormal cytology detected at our unit, showing the highest at 25 cases in 2014 and the lowest at 8 cases in 2013. The total number of abnormal results was reported in 72 cases out of 942 invasive procedures giving a rate of 7.6% of picking abnormal results which is consistent with what is reported by many studies. (8, 9). The type of abnormalities detected over 5 year's period are shown in Figure1. As shown above, the majority of abnormalities were Trisomy 21, 18 and 13 making 76% of all abnormalities detected. The rest of the abnormalities included few cases of Turners, Triploidy and Klinefelter. These findings are in agreement with what is reported by other studies. (10,11). There were also few cases of reciprocal translocations and deletions. All samples had early results using quantitative fluorescence polymerase chain reaction for the rapid testing for chromosome 13, 18, 21, X and Y chromosome within 24-48 hours and then a complete culture of all chromosomes within 2 weeks. The advantage of having CVS for our patients is to have an early result. Termination of pregnancy is not allowed in Jordan but we have FATAWAS from religious leaders which allow it, if the fetus has severe abnormality and the baby has not exceeded 120 days. Few patients opted for termination of pregnancy in cases of severe abnormalities. Amniocentesis is technically easier but the results are later compared to CVS. (12) We had 8 cases of culture failure, 5 after CVS and 3 after AC. This is consistent with what has been reported in several studies. (13,14) (Figure 2) shows indications of procedures annually between 2013 and 2017, showing AMA as the leading indication followed by family history of abnormal offspring. Ultrasound indication, on the other hand, rose significantly in 2017 reaching 62 cases compared to the number of cases in previous years and to other indications. There is a drop in AMA as an indication in 2017 as more numbers of patients started to do first trimester screening test which led to a reduction in unnecessary procedures as illustrated in figure 1. Ultrasound indication, on the other hand, rose significantly in 2017 reaching 62 cases compared to the number of cases in previous years and to other indications. This can be explained by the introduction of high standard U/S machine at our unit by the end of 2016. Few cases were done because of high risk on biochemical screening which was done privately. The majority of our invasive procedures were Amniocentesis, constituting 74.7% of all procedures. The rest of the procedures were done by CVS. (Table I) This is probably because Amniocentesis needs less training and most of our patients are referred late to our fetal medicine unit. (15.16) The rate of miscarriage rates for both procedures is constant over the 5 years period. The pregnancy loss in our study was 0.28% for Amniocentesis and 1.265 for CVS as shown in (Table II). These results are consistent with what is reported in the literature. (17,18) We usually councel our patients and tell them that the rate of miscarriage for both procedures at our unit is 1% but after these results, we should tell our patients that the risk of miscarriage from amniocentesis is less than CVS and amniocentesis is safer.
There are many studies on Amniocentesis; the most prominent is by Tobaretal which reported a 1% rate of fetal loss after amniocentesis [18]. More recent studies were by Seeds (15) and Mujezinovicet.al (16) concluded that pregnancy loss after amniocentesis was 0.6%. Philip et.al in 2004 reported a miscarriage rate of less than 0.5% (19). Several factors lead to increase the rate of miscarriage post invasive diagnostic procedures such as the operator’s experience (the experienced operator has a lower rate of loss) (20). Other important factors that increase the rate of miscarriage are increase PAPP-A and increased NT (21). Our miscarriage rates for both procedures are acceptable. (Table III) shows the frequency of the abnormalities detected in relation to the indication of procedure. The highest numbers of abnormalities were detected after scanning the mother due to advanced maternal age where the number of detected cases was 27 (37.5%). This is followed by abnormal US findings with a number of 20 cases (28%). The least number of detections occurred with the history of abnormal offspring standing at 17%.I think that we need to look again at advanced maternal age as an indication as the numbers are high! NIPND testing is a new procedure and we are looking at introducing it at the RMS.
At the end, our fetal medicine unit at King Hussein Medical Centre is busy, our doctors are experienced. We perform a large number of invasive procedures annually. Our complication rates are consistent with what is reported in other studies as shown earlier.
Conclusion
At King Hussein Medical Centre, the most common method of invasive procedure is amniocentesis followed by CVS. Advanced maternal age is the most common indication for invasive prenatal procedures, however, this indication is on the decline due to the introduction of biochemical testing and None invasive prenatal diagnosis (NIPND). Miscarriage rates are consistent with what is reported in the literature. Amniocentesis is safer than CVS
References
1.National Institute of Child Health and Human Development. Report of the NICHHD workshop on chorionic villus sampling and limb and other defects. Am J ObstetGynecol1993;169:1–6
2.Firth HV, Boyd PA, Chamberlain P, MacKenzie IZ, Lindenbaum RH, Huson SM. Severe limb abnormalities after chorionic villus sampling at 56-66 days' gestation. Lancet. 1991; 337(8744): 762-3.
3.American College of Obstetricians and Gynaecologists. ACOG Practice Bulletin No. 88, December 2007. Invasive prenatal testing for aneuploidy. Obstet Gynecol 2007; 110:1459
4.Wapner RJ. Chorionic villus sampling. Obstet Gynecol Clin North Am 1997; 24:83.
5.Caron L, Tihy F, Dallaire L. Frequencies of chromosomal abnormalities at amniocentesis: over 20 years of cytogenetic analyses in one laboratory.Am J Med Genetics 1999;82:149-54.
6.Han SH, An JW, Jeong GY. Clinical and cytogenetic findings on 31,615 mid-trimester amniocenteses. Korean J Lab Med 2008;28:378-85
7.Amniocentesis and Chorionic Villus Sampling (Green top guidelines NO.8 June 2010) RCOG
8.Nizard J, Duyme M, Ville Y. Teaching ultrasound-guided invasive procedures in fetal medicine: learning curves with and withoutan electronic guidance system. Ultrasound ObstetGynecol2002;19:274–7.
9.Blessed WB, Lacoste H, Welch RA. Obstetrician–gynecologists performing genetic amniocentesis may be misleading themselves and their patients. Am J ObstetGynecol2001; 184: 1340–1342
10.Nicolaides KH, Brizot M, Patel F, Snijders R. Comparison of chorionic villus sampling and amniocentesis for fetal karyotyping at 10–13 weeks' gestation. Lancet1994; 344: 435–439
11.Vijayan Valaytham, Raman Subvamanian, Yap Juan, Patrick Chia. Indications for Invasive Prenatal Diagnostic Procedures at a Dedicated Fetal Medicine Centre: An 8 Year Audit 2003-2010.Med J Malaysia vol68 No4, Augest 2013
12.Smidt-Jensen S, Permin M, Philip J, Lundsteen C, Zachary J,Fowler S, et al. Randomized comparison of amniocentesis andtransbdominal and transcervical chorionic villus sampling.Lancet1992;340:1237–44
13.Alfirevic Z, Mujezinovic F, Sundberg K. Amniocentesis and chorionic villus sampling for prenatal diagnosis. Cochrane Database Syst Rev 2003;(3):CD003252. DOI: 10.1002/14651858.CD003252.
14.Namrata Kashyap*, Mandakini Pradhan, Sangeeta Yadav, Neeta Singh. Invasive prenatal diagnostic procedures: a developing countries’ perspective. Int J Reprod Contracept Obstet Gynecol. 2016 Jan;5(1):41-
15.Seeds JW. Diagnostic mid trimester amniocentesis: how safe?Am J ObstetGynecol2004; 191: 607–615.
16.Mujezinovic F, Alfirevic Z. Procedure-related complications of amniocentesis and chorionic villous sampling: a systematic review. ObstetGynecol2007; 110: 687–694.
17.Tseng JJ, Chou MM, Lo FC, Lai HY, Chen MH. Detection of chromosome aberration in the second trimester using genetic amniocentesis: experience during 1995e2004. Taiwan J ObstetGynecol2006;45:39-41.
18.Tabor A, Vestergaard CH, Lidegaard O. Fetal loss rate after chorionic villus sampling and amniocentesis: an 11-year national registry study. Ultrasound ObstetGynecol2009; 34: 19–24.
19.Philip J, Silver RK, Wilson RD, Thom EA, Zachary JM, Mohide P. Late first- trimester invasive prenatal diagnosis: Results of an international randomized trial. Obstet Gynecol. 2004;103(6):1164–1173.
20.Wijnberger LDE, van der Schouw YT, Christiaens GCML. Learning in medicine: chorionic villus sampling. Prenat Diagn2000; 20: 241–246.
21.Akolekar R, Bower S, Flack N, Bilardo CM, Nicolaides KH. Prediction of miscarriage and stillbirth at 11–13 weeks and the contribution of chorionic villus sampling. Prenat Diagn2011; 31: 38–45