ABSTRACT
Objective: Alkaptonuria is a metabolic disease caused by deficiency of the hepatic enzyme homogentisate 1, 2 dioxygenase (HGD), consequently the homogentisic acid (HGA) accumulates in the cells and body fluids. This accumulation causes early degeneration and black discoloration of the knees, spine, sclera, heart endocardium and valves. Joints arthroplasty is the treatment of choice when the conservative treatment is no longer effective.
Methods: Retrospectively fourteen alkaptonuria patients who have had knee replacement in our center have been analyzed, four females and ten males, six cases had bilateral knees replacements, follow up period ranges between 12- 36 months. Also, this study includes a review of 22 studies of joints replacement in alkaptonuria patients, these studies have been published between 2000-2016, and have included 36 patients; 12 females and 24 males, 63 joints had been replaced (39 knees, 21 hips and three shoulders). All these 50 patients have been followed for a period that range between 12-36 months.
Results: Our fourteen patients have had significant improvement after total knee replacements and there were no intra operative complications, during our follow up period no post-operative infections or any significant complaint have been observed. Also the 22 published studies have had no complication and they had good results.
Conclusion: Few cases of alkaptonuria have been operated by joint replacements and have been reported in the literatures, the follow up periods were not long. So more cases and longer period follow up are needed to estimate the benefits and the risks of the joint replacement in these patients with alkaptonuria. But according to our results joint replacement seems to be the treatment of choice to alleviate the pain in severely affected joints in alkaptonuria patients.
Keywords: Alkaptonuria, Jordan, Total knee replacement.
JRMS August 2019; 26(2):45-53/ DOI: 10.12816/0053290
Introduction
The history of alkaptonuria (AKU) (also called the black bone disease) started 1500 BC in the old Egyptian people; an Egyptian mummy was diagnosed with this disease.(1) It is the first human inherited disease found to fit the rules of Mendelian autosomal recessive inheritance.(2) Alkaptonuria is a rare disease with a prevalence of 1 case per 1 million to 250,000 live births. (3) Some population has reported higher prevalence rate; in Slovakia the prevalence is 1 case per 19000 live births.
(4) Alkaptonuria is a metabolic disease caused by deficiency of the hepatic enzyme homogentisate 1,2 dioxygenase (HGD), so the homogentistic acid (HGA) accumulates in the cells and body fluids, after accumulation of the acid the polymerization process changes it to a blue-black pigment that deposit in the skin, cartilage and collagenous tissue (ochronosis).(5) This accumulation causes early degeneration of the knees, spine, sclera, heart endocardium and valves.
(6) The natural history of the disease has a wide range of variations but it usually starts with dark urine at birth. Ochronosis and the arthropathy that affect peripheral large joints and spine start in the third and fourth decade of life, kidney and cardiac valves start in the fifth and sixth decade. (7, 8) Diagnosis is based on the changing of urine color after exposure to air. Laboratory investigations such at the iron chloride reduction test which gives the green-blue color and the addition of Benedict reagent in which the color become brown. Conformation of diagnosis can be made by detection of high quantities of HGA in the urine using the gas chromatography mass spectrophotometer (GCMS). The prevalence of Alkaptonuria in Jordan is unknown. Recent published studies showed that there are 64 cases; 40 cases have been reported form the same village and nine of them were identified in one family. (9, 10) The reason of this high rate is the consanguineous marriages which estimated to be 28%-63% in Jordan.(11) Currently, the treatment of symptoms is the accepted approach. However, the joint replacement procedures are the treatment of choice for significant degenerative arthritis. (12)
Methods
The study protocol was submitted and approved by the institution's technical and ethics review board. After the ethical community acceptance, we conducted and analyzed a series of fourteen patients with alkaptonuria; 10 males and four females, six cases had bilateral knee replacements, the ages range between 65 and 60. All patients were evaluated according to the Knee society score pre operatively and the ranges were between 20-50 with poor function. Five cases had no alignment deformity, seven cases had moderate knee Varus deformity (<5 degrees) and two cases had severe Varus knee deformity. All 20 surgeries have been done under general anesthesia; spinal anesthesia was avoided according to the Anesthesia recommendation for patients suffering from Alkaptonuria.13 Black discoloration of the femoral condyles cartilage, patella, meniscus and surrounding soft tissue was seen in the all surgeries. (Figure 1, 2 & 3C). The histological results showed thickened synovium, dark pigmented cartilage and reactive giant cells. All patients are over 60 year old and should be evaluated for osteoporosis and should be treated accordingly. In the future we plan to raise this issue in our study.
Intraoperative and post-surgery complications were observed. The fourteen patients have been followed up for 12-36 months in the clinic according to the Knee Society score and functional knee score.
Ten patients were referred to us from alkaptonuria research office at the Faculty of Medicine of Mutah University, the following four patients were diagnosed accidentally after the intraoperative observations.
Case 1:
A 64 year-old man presented to the Rheumatologic clinic in prince Ali Hospital, Karak, Jordan, in April 2009 for knees pain and limitation of motion which was causing to him significant disability in his daily activity and in his work as a farmer, his problems have started and progressed since nine years. He has had a history of discoloration of urine that changed to dark - black after urination. He was born of second degree consanguineous marriage and he was fourth in birth order. There is no history of any chronic drug intake. The head and neck examination, revealed black discoloration of the sclera as well as of the ear. (Figure 1A & 1B) Radiographic evaluation by bilateral standing knees plan X-R has showed advanced degenerative osteoarthritis involving medial, lateral and patella-femoral compartment, more significant at the medial side. No osteophytes were detected on either side. (Figure 2A)
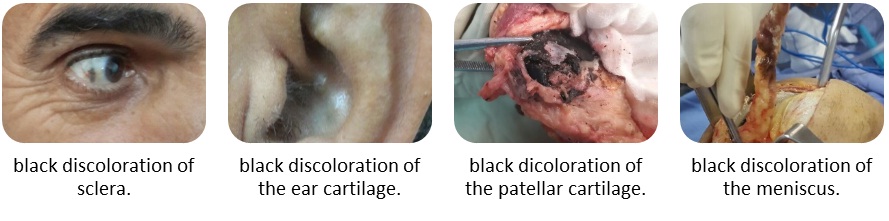
Fig 1: Clinical manifestation of Alkaptonouria; black discoloration of the sclera, ear, patella and meniscus.
Fig 2: Osteoarthritic changes due to Alkaptonouria.
The patient underwent cemented total knee arthroplasty for one side in 2013 and for the other side he underwent the same cemented total knee prosthesis in 2014. (Figure 3A) The macroscopic findings at surgery showed extensive loss of articular cartilage, with black staining of the degenerative cartilage, menisci, and the synovial tissues. (Figure 1C) The patellar tendon was stiff and attenuated, which was making the patellar mobilization a little bit difficult.
Case 2:
A 63-year-old male, he was referred to the orthopedic clinic for evaluation of long standing bilateral knees pain. His pain has been associated with some knees swelling some times. Non-steroidal anti-inflammatory drugs (NSAIDs) are no longer provided relief of symptoms. The patient has mentioned other joints pain such as back pain and shoulders pain that does not interfere with his life style. He has a family history of joints problems and he was born of third degree consanguineous marriage and he was second in birth order. There was no history of any chronic drug intake. . His knees had neutral alignment. Further examination showed a mild knees swelling due to minimal amount of joints effusion. Ranges of motion were 0-110 of flexion with some crepitation. Compression of the patella-femoral joint caused a significant discomfort. No laxity of the collateral and cruciate ligaments was found. The radio graphical evaluation showed bilateral knees osteoarthritis which needed surgical intervention by total knee arthroplasties. He underwent left knee arthroplasty in 2013 and the right one in 2014, during surgery, dark black discoloration of the cartilage and of the soft tissues was observed. (Figure 1D & 2C) The histopathological study showed black pigmentations of the bone and the surrounding soft tissues. There were no intraoperative or post-operative complications. After the first surgery the patients was examined again and he was found to have black spots in his eyes, ears and nail beds. He had high levels of HGA and was diagnosed as a case of alkaptonuria.
Case 3:
A 63-year-old male, resident in Karak, presented to the orthopedic clinic for further evaluation of his 8 years left knee pain that was characterized as painful locking symptoms. He has tried NSAIDs and the intra-articular injection without significant relief. He has had a history of discoloration of urine that changed to dark - black after urination. He was born of second degree consanguineous marriage and he was fifth in birth order. During his first visit he was found to have black spots in his eyes, ears and nail beds of his thumbs. The left knee has had diminished range of motion and in fixed flexion position about 20 degrees, his right knee also had limited range of motion with crepitation. Bilateral standing knees plan X-R showed advanced degenerative osteoarthritis. (Figure 2B) The patient underwent left knee arthroplasty in 2014 and he described it as a miracle, and he underwent right knee replacement in 2015(Figure 3B). Both surgeries had no complications and the black discoloration was observed in the all compartments of the knees. (Figure 3C)

Fig 3: Bilateral Knee Replacement for Alkaptonouria patient
Case 4:
A 60-year-old male, cars painters, lives in Zarqa city but his was born in Kark city where he had raised with his family. He have presented to the orthopedic clinic for evaluation of long standing bilateral knees pain and deformities. The patient has mentioned other joints pain such as back pain and shoulders pain that also interfere with his life. He has a family history of joints problems and he was born of third degree consanguineous marriage and he was third in birth order. His knees had severe Varus malalignment in flexed flexion deformity 25 degrees with limited range of motion 25-80 degrees. The radio graphical evaluation showed bilateral knees osteoarthritis and Varus deformity which needed surgical intervention by total knee arthroplasties. He underwent left knee arthroplasty in 2015 and the right one in 2016, during surgery, dark black discoloration of the cartilage and of the soft tissues was observed. (Figure 4)

Fig 4: Bilateral Osteoarthritis due to Alkaptonouria. Intraoperatively, black discoloration s of the soft tissue
The histopathological study showed black pigmentations of the bone and the surrounding soft tissues. There were no intraoperative or post-operative compilations. After the first surgery the patients was examined again and he was found to have black spots in his eyes, ears and nail beds. He had high levels of HGA and was diagnosed as a case of alkaptonuria.
Results
In this study, our fourteen patients had significant improvement according to the Knee Society score, the scores ranges between 70-95, and the functional knee score ranges between 65-95. There were no intra operative complications. During our follow up periods which range between 12- 36 months, the patients have pain free range of motion; 0-110 flexion, they can walk independently without support and we did not observe any post-operative infections or any significant complaint. The published articles since 2000 till 2016; no failures or major complications were mentioned in such cases and all patients have had significant improvement regarding the pain and the range of motion.
Discussion
The ochronotic arthropathy is devastating problem for the patients and can be divided to endogenous ochronosis (alkaptonuria) and exogenous ochronosis which are induced by exposure to some harmful substances such as topical phenol, oral antimalarial drugs and levodopa. (6) Alkaptonuria is a rare inherited metabolic disease which has a wide variety of mutations (115 known mutations till now) (14) and inherited as recessive autosomal manner. The disease consequences accelerate in the fourth decade of life due to the decrease of renal clearance ability and increasing the accumulation of the homogentistic acid. (15)
Alkaptonuria is a systemic disease. Regarding the musculoskeletal system; the most frequent manifestation is the intervertebral space calcification and narrowing involving the entire spine, followed by peripheral major joints degeneration. The degeneration first appears in the knees, hips, and shoulders but surprisingly it spares the sacroiliac joints. All these manifestations causing pain, limited morbidity and recurrent joint swellings.(16, 17) Our patients have had a persistent bilateral knees pain for long duration, the pain increased with activity and at the end of the day, also they mentioned recurrent knees swellings that have been resolved spontaneously. Other complaints have involved mild hips and back pain. Non-steroidal anti-inflammatory drugs that were prescribed by the primary physicians no longer have provided relief of the pain.
The cardiovascular system could be affected in late stage of the disease due to valves calcification that my leads to aortic stenosis, ischemic heart disease and myocardial infarction. (7,8) Alkaptonuria can cause respiratory alterations such as throat dryness, dysphagia and dyspnea. (18) Also in late stages of the disease the patient may be suffering from urinary disorders such as nephrolithiasis and even renal failure. (19, 20) Radiographic evaluation by bilateral standing knees plan X-R for the patients of this study has showed advanced degenerative osteoarthritis involving medial, lateral and patella-femoral compartment, more significant at the medial side. No osteophytes were detected on either side. (Figure 2) There is no specific treatment for alkaptonuria, decreasing the intake of the tyrosine and phenylalanine and increasing the intake of vitamin C have shown poor clinical evidence. A 3 year randomized therapeutic trial of nitisinone in alkaptonuria showed significant reduction of homogentistic acid in plasma and urine without improving the joints functions. (21, 22) The treatment of the musculoskeletal system is symptomatic and depends on the stage of the disease. In early degenerative stage the swimming, truncal muscles strengthening and non-steroidal ant inflammatory drugs can provide benefit to the patients but it cannot decrease the rate of the cartilaginous joint surfaces destruction that manifests at the third and fourth decade. Joints arthroplasty is the treatment of choice for the late degenerative stage when the conservative treatment is no longer effective. There are no guidelines for joint replacement in alkaptonuria patients because all published cases have been published as case reports. (Table I). In our review of the 22 published articles since 2000 till 2016; no failures or major complications were mentioned in all cases and the patients have had significant improvement regarding the pain and the range of motion. But the published cases of alkaptonuria are few and the follow up periods for these cases were not long.
Table I: All the published cases of Alkaptonouria between 2000-2018
|
Results
|
Follow up time
|
Procedure
|
gender
|
Age
|
Number of
cases
|
Article
|
Year
|
|
Improvement
|
15-36 months
|
Total knee
replacements
|
Females and
males
|
62
|
Fourteen
|
Jamal Alshawabkeh et. al
|
2018
|
|
|
|
|
|
|
|
|
|
|
Improvement
|
3 year
|
Total hip and
knee
|
male
|
62
|
one
|
.Adamopoulos A. et al.23
|
2016
|
|
Improvement.
|
15
months
|
Total knee
replacement.
|
female
|
67
|
one
|
Mota PT. et al.24
|
2015
|
|
-------
|
-------
|
Total knee
replacement
|
male
|
66
|
one
|
Ardhanari .et al.25
|
2105
|
|
improvement
|
6 months
|
Total hip
replacement
|
male
|
46
|
one
|
Kaya, O. et al.26
|
2014
|
|
good
|
6 years
|
Bilateral
total shoulders
|
male
|
53
|
two
|
Varvitsiotis. et al.27
|
2014
|
|
improvement
|
6 months
|
Total hip
replacement
|
male
|
55
|
one
|
Ursino N. et al.28
|
2013
|
|
Good
|
12
months
|
Bilateral total
knees
|
male
|
69
|
Two
|
Ramadan.et al.29
|
2013
|
|
improvement
|
18
months
|
Right hip and
left total knee replacement.
|
female
|
62
|
two
|
Mehmit Ali
Acar. et al.30
|
2013
|
|
Good
|
------
|
Right knee
replacement
|
male
|
77
|
one
|
Varvitsiotis. et al.31
|
2012
|
|
Excellent
|
2 years
|
Left total
knee replacement
|
male
|
48
|
One
|
Abimbola.et al.32
|
2011
|
|
Good
|
------
|
Left knee
replacement
|
female
|
68
|
One
|
Fontao-Fernandez. et al.33
|
2010
|
|
-----
|
-------
|
Right hip
|
female
|
54
|
one
|
Babak
Siavashi. et al.34
|
2009
|
|
Good
|
------
|
Bilateral knees
replacement
|
male
|
56
|
two
|
Araki. et al.35
|
2009
|
|
Good
|
10
months
|
Bilateral
knees replacement
|
female
|
60
|
two
|
Kefeli. et al.36
|
2008
|
|
Good
|
----
|
Bilateral
knees replacement
|
male
|
59
|
two
|
Koetela. et al.37
|
2008
|
|
Improvement
|
2 year
|
Total hip
replacement
|
male
|
62
|
one
|
Kerimoglu S. et al.38
|
2005
|
|
Improvement
|
12 years
|
Knees, elbow,
shoulder and hips
|
females
|
53, 75,
72.
|
Eleven.
|
Spencer.et al.39
|
2004
|
|
Improvement
|
7 year
|
Bilateral
knees replacement and hip.
|
male
|
69
|
three
|
Fisher and
Davis.40
|
2004
|
|
Improvement
|
5 year
|
Bilateral
knees replacement and hip.
|
male
|
70
|
three
|
Moslovac.et al.41
|
2003
|
|
Improvement
|
14
months
|
Bilateral
knees replacement
|
male
|
70
|
two
|
Demir.42
|
2003
|
|
Good
|
4 year
|
Left knee
replacement
|
male
|
48
|
one
|
Aydogdou. et al.43
|
2000
|
|
Good
|
2 year
|
Bilateral hips
replacement
|
Female
|
54
|
two
|
Aynaci O. et al.44
|
2000
|
Conclusion
Few cases of alkaptonuria have been operated by joint replacements and have been reported in the literatures, the follow up periods were not long. So, more cases and longer period follow up are needed to estimate the benefits and the risks of the joint replacement in these patients with alkaptonuria. But according to our results joint replacement seems to be the treatment of choice to alleviate the pain in severely affected joints in alkaptonuria patients.
References
1. Stenn FF, Milgram JW, Lee SL, Weigand RJ, Veis A (1977). Biochemical Identification of Homogentisic Acid Pigment in an Ochronotic Egyptian Mummy. Science 1979(4303):566-568.
2. Zatkova ANemethova M. Genetics of alkaptonuria – an overview. Acta Facultatis Pharmaceuticae Universitatis Comenianae. 2015; 62(s11).
3. Mistry, J., Bukhari, M. and Taylor, A. “Alkaptonuria”. Rare Diseases. (2013) 1(1), p.e27475.
4. Rovenský J, Urbánek T, Imrich R. Alkaptonuria and Ochronosis – Experience From Slovakia. Acta Facultatis Pharmaceuticae Universitatis Comenianae. 2014; 61(1).
5. Gallagher J, Dillon J, Sireau N, Timmis O, Ranganath L. Alkaptonuria: An example of a “fundamental disease”—A rare disease with important lessons for more common disorders. Seminars in Cell & Developmental Biology. 2016; 52:53-57.
6. Taylor, A., Hsueh, M., Ranganath, L., Gallagher, J., Catterall, J. and Kraus, V. “Analysis of Cartilage Biomarkers of Aging and Turnover in the Osteoarthropathy of Alkaptonuria”. Osteoarthritis and Cartilage. (2015), 23, p.A135.
7. Pettit SJ, Fisher M, Gallagher JA, Ranganath LR. “Cardiovascular Manifestations of Alkaptonuria”. J Inherit Metab Dis 2011; 34:1177-81. Doi: 10.1007/s10545-011-9339-z.
8. Lok, Z., Goldstein, J. and Smith, J. “Alkaptonuria-Associated Aortic Stenosis”. J Card Surg, (2013). 28(4), pp.417-420.
9. Al Sbou M, Mwafi N, Lubad MA. “Identification of Forty Cases with Alkaptonuria in one Village on Jordan”. Rheumatol Int 2012; 32:3737-40. Doi: 10.1007/s00296-011-2219-x.
10. Al Sbou M, Mwafi N. “Nine Cases of Alkaptonuria in one Family in Southern Jordan”. Rheumatol Int 2012; 32:621-5. Doi: 10.1007/s00296-010-1701-1.
11.Tadmouri GO, Nair P, Obeid T, Al Ali MT, Al Khaja N, Hamamy HA (2009). “Consanguinity and Reproductive Health among Arabs”. Reprod Health 6:17. DOI: 10.1186/1742-4755-6-17
12. Reddy, O., Suresh, B., Gafoor, J. and Prasad, P. Alkaptonuria with review of literature. J NTR Univ Health Sci, (2014). 3(2), p.125.
13. Kastsiuchenka, S. and Mikulka, A. (2013). “Anaesthesia and Oorphan Disease”. European Journal of Anaesthesiology, 30(12), pp.779-780
14. Zatkova A. “An Update on Molecular Genetics of Alkaptonuria (AKU)”. J Inherit Metab Dis 2011; 341:1127-36. Doi: 10.1007/s10545-011-9363-z.
15. Saadati, N., Khodashahi, M. and Naghibzadeh, B. “A Case of Alkaptonuria Diagnosed in Late Adulthood”. IJMPCR, (2016). 6(4), pp.1-5.
16. Franz, A. and Abusafieh, M. (2016). “Severe Osteoarthritis of the Knee as an Early Symptom of Alkaptonuria, A Case Report”. Shafa Orthopedic Journal.February 2016, 3(1); e4547. DOI: http://dx.doi.org/10.17795/soj-4547.
17. Mwambingu, T. and Hide, G. Case 208: “Alkaptonuria”. Radiology, (2014).272(2), pp.608-611.
18. Abdullah, I., Rana, A. and Saeed, U. “Alkaptonuria, More than just a Mere Disease”. Journal of Neurosciences in Rural Practice, (2015). 6(2), p.257.
19. Sali, G., Thomas A., Kumar G., Nair B., Sanjeevan K., Mathew G, et al “Extensive Prostatic Calculi in Alkaptonuria: An unusual manifestation of rare disease”. Asian Journal of Urology, (2015).2(3), pp.179- 181.
20.Bataille, S., Moal, V., Aquaro, R., Grünfeld, J. and Daniel, L. “Hemolysis: a fatal complication of alkaptonuria in a severe renal failure patient”. CN, (2014). 81(05), pp.374-376.
21. Introne WJ, Perry MB, Troendle J, Tsilou E, Kayser MA, Suwannart P, et al. “A 3 Year Randomized Therapeutic Trial of Nitisinone in Alkpatonuria”. Mol Genet Metab. 2011; 103: 307-314.
22. Laschi M, Bernardini G, Dreassi E, Millucci L, Geminiani M, Braconi D, et al. Inhibition ofpara- Hydroxyphenylpyruvate Dioxygenase by Analogues of the Herbicide Nitisinone As a Strategy to Decrease Homogentisic Acid Levels, the Causative Agent of Alkaptonuria. ChemMedChem. 2016; 11(7):674-678.
23. Adamopoulos A, Panagiotis, Gavras M, soukakos K. 2016, “Total knee and Hip Reconstruction in Male Patient with Alkaptonouria with 3 Years of follow up: Case Report and Review of the Literature”. MOJ Orhtropedics & rheumatology. 2016, volume 4 Issue 3:00137.
24. Mota PT, Candido R, Pintado C (2015). “Alkaptonuria, a Rare Cause of Osteoarthritis-Case report”. JSM Clin Case Rep (2015); 3(3):1083.
25. Ardhanari A, Seetharam V, Subbaramaiah M, Kumaraswamy M. Anaesthetic management of a case of Alkaptonuria for Total knee arthroplasty. Sri Lankan J Anaesthesiol. 2015; 23(1).
26. Kaya, O. “Total hip replacement for an ochronotic patient: A technical trick”. Am J Case Rep, (2014) 15, pp.27-30.
27. Dimitrios V, Emmanouil D, Christoforos T, Athanasios P, Georgios P, et al. “Patient suffering from Ochronotic Arthropathy treated with Bilateral Total Shoulder Arthroplasty. Presentation of this case report with 6 years follow up”. Acta Orthopedica Hellenica (2014). 65(1): 3336.
28.Ursino N D. A Case Report: A Cementless Total Hip Arthroplasty in a Patient with Alkaptonuria. Orthopedic & Muscular System. 2013; 02(02).
29. Ozmanevra R, Güran O, Karatosun V, Günal I. “Total Knee Arthroplasty in Ochronosis: a case report and critical review of the literature”. Eklem Hastalık Cerrahisi (2013). 24(3): 169
30. Acar MA, Erkocak OF, Aydin BK, Altan E, Senaran H, et al. “Patients with Black Hip and Black Knee Due to Ochronotic Arthropathy: Case Report and Review of Literature”. Oman Medical J (2013). 28(6): 448-449
31. Malakasi I, Skagias I, Vrasami I, Grivas TB. “Total Knee Arthroplasty in a Patient with Ochronotic Arthritis. Case report and review of the literature”. Scientific Chronicles (2012). 17(2): 98-99.
32. Abimbola O, Hall G, Zuckerman JD. “Degenerative Arthritis of the Knee Secondary to Ochronosis”. Bull NYU Hosp Jt Dis (2011). 69(4): 331334.
33. Fontao-Fernández L, Ferreirós-Conde MJ, Otero-Villar J (2010).” Ochronotic Arthropathy: A presentation of 2 cases”. Rev Esp Cir Ortop Traumatol 54(6): 396-398.
34. Siavashi B, Zehtab MJ, Pendar E (2009).” Ochronosis of Hip Joint; a case report”. Cases J 2: 9337.
35. Araki K, Sudo A, Hasegawa M, Uchida A. “Devastating Ochronotic Arthropathy with Successful Bilateral Hip and Knee Arthroplasties”. J Clin Rheumatol (2009). (3): 138-140
36. Kefeli M, Tomak Y, Can B, Bariş S. “Arthroplasty for the Treatment of Joint Degeneration caused by Ochronosis in two Cases”. Acta Orthop Traumatol Turc (2008).42(2): 139-144.
37. Kotela A, Pirko K, Kotela I. “Ochronosis as A Cause of Multiple Joint Osteoarthritis in one Patient”. Przegl Lek (2010). 67(5): 427-431.
38. Kerimoglu S, Onder C, Aynaci O, Malkoc CH. (2005). “Hip Arthroplasty for Ochronosis”. Saudi Med J. 2005; 26:1812–1814.
39. Spencer JM, Gibbons CL, Sharp RJ, Carr AJ, Athanasiou NA. “Arthroplasty for Ochronotic Arthritis: no failure of 11 replacements in 3 patients followed up 6-12 years”. Acta Orthop Scand (2004). 75(3): 335338.
40. Fisher AA, Davis MW. “Alkaptonuric Ochronosis with Aortic Valve and Joint Replacements and Femoral Fracture: a case report and literature review”. Clin Med Res (2004). 2(4): 209-215.
41. Moslavac A, Moslavac S, Cop R (2003). “Case report of a patient with ochronosis and arthroplasty of the hip and both knees”. Reumatizam 50(1): 26-28.
42. Demir S (2003). “Alkaptonuric ochronosis: a case with multiple joint replacement arthroplasties”. Clin Rheumatol 22(6): 437-439.
43. Aydoğdu S, Cullu E, Ozsoy MH, Sur H (2000). “Cementless total knee arthroplasty in ochronotic arthropathy: a case report with a 4-year follow-up”. J Arthroplasty 15(4): 539-543.
44. Aynaci O, Onder C, Turhan AU (.2000). “Bilateral Hip Arthroplasty for Ochronotic Arthropathy”. Clin Rheumatol. 2000; 19:150–152.