ABSTRACT
Background: The definitive goal of plastic surgery in congenital craniofacial anomalies is to create symmetry and reach near normal aesthetic appearance. Comprehensive knowledge of normal facial shape and aesthetic subunits will help surgeons in their preoperative strategies for success. Lips are thecornerstone in facial appearance and the philtrum represents its central aesthetic subunit. Since measures and topography of normal facial appearance vary among different races and communities, several studies have delineated the variations in philtral morphology in different communities.
in this prospective study, performed by pediatric dentists and plastic surgeons, we delineate the different morphologies of philtrum in normal Jordanian pediatric population which will have practical applications in cleft lip surgery.
Methods: This was a prospective study in 200Jordanian children (106 males, 94 females)of less than 14 years of age presented to dental pediatric clinic at King Hussein Medical Center, without any craniofacial anomalies or trauma. The ethical committee approved the study, and consent forms were signed by the parents before taking photos of the children.
All medical
photographs of each participant in 3 views (frontal, basal and lateral)were
taken using a Samsung S6 edge plus digital 16-megapixel camera (Samsung South Korea). The photographs
were analyzed blindly by three plastic surgeons, to determine the shape of
philtrum for each participant using the following points:
1.
The peaks of the Cupid’s bow (cphi–cphi)
2. Origin of philtral column at each
side(cphs-cphs)
Photos were analyzed using MS Paint program for photos (Microsoft Paint for Windows 7). Our classification of the morphology of the philtrum was based on modifications of A. Mori et al.ˡ in Japanese children: Type 1 triangular, type 2 parallel, type 3 concave and type 4 flat(Fig.2).
Limitations to this study include The quality and limitations of two-dimensional photographic assessments compared to three-dimensional photogrammetric systems, its sensitivity to the angle at which the photograph is captured and the position of the subject, however, it’s cost-effective and noninvasive in terms of facial shape evaluation especially if high-resolution medical photography is used. Also, another limitation is the need for three-dimensional photogrammetry or lasers system for accurate anthropometric distance measurements, and if there are true morphological changes in correlation with the age of each subject.
Results: The most common morphology of philtrum was type 1- triangular, observed in 92/200 (46%)children. The least common morphology of philtrum was type 4-flat, observed in 7/200 (3.5%) children.
Conclusion: The definitive goal of cleft lip surgery is to obtain near normalcy in function and aesthetics, keeping in mind that facial morphology varies among different races, we hope that the results of our study delineate the different morphologies of philtrum shape in Jordanian children and will be a synergistic tool for our surgeons in their preoperative markings and planning.
Keywords: Cleft lip,Cleft lip geometric repair, Philtrum, Philtral columns, and Upper lip subunits
JRMS December 2019;26(3):37-47/ 10.12816/0054816
Introduction
The definitive goal of plastic surgery in congenital craniofacial anomalies is to create symmetry and reach near normal aesthetic appearance.
Comprehensive knowledge of normal facial shape and aesthetic subunits will help surgeons in their preoperative strategies for success. Lips are important in facial appearance and the philtrum represents its central aesthetic subunit. Since measures and topography of normal facial appearance vary among different races and communities, several studies have delineated variations in philtral morphology in certain communities.ˡ,2
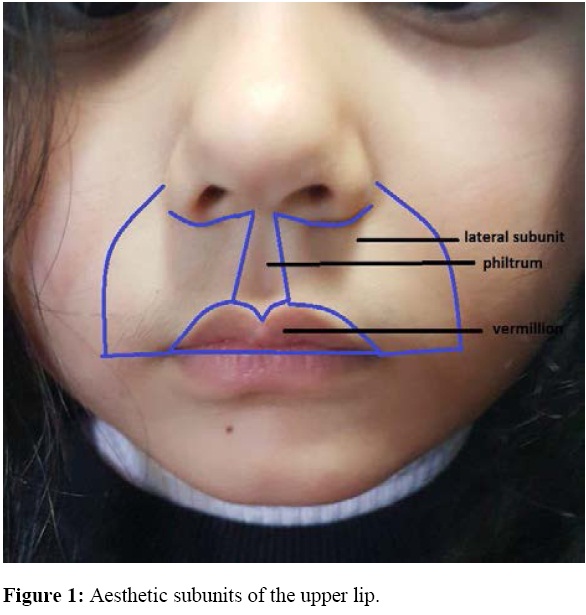
The upper lip is composed of three subunits: Vermillion, philtrum, and lateral units bounded superiorly by the columella and alar grooves, inferiorly by the interlabial space and laterally by the nasolabial folds. Borders between these three subunits form the philtral columns (ridges), cupid bows and vermillion border. Furthermore, the vermillion is subdivided into dry and wet mucosa separated by the wet to dry line (Fig.1).3
Several classifications are proposed for the morphology of the philtral columns, for example by Mohler, Uemura, and A. Mori. The classification of the morphology of philtrum based on modifications of A. Mori et al.ˡ in Japanese children is as follows (Fig 2): Type 1-triangular, type 2- parallel, type 3- concave and type 4 - flat. In the Triangular type, the origins of the philtral column are located near both sides of the medial crural footplates and the dimple is triangular. In the Parallel type, the philtral columns originate from the nostril sills, exhibit an almost parallel shape and the dimple is rectangular. In the Concave type, the upper cross of the philtral columns is located in the middle of the upper lip, and there is no philtrum dimple in the upper half of the upper lip, the dimple is accentuated in the lower half only. And in the Flat type, the philtral columns have almost no prominence, the dimple is flat and nearly absent. 1,2

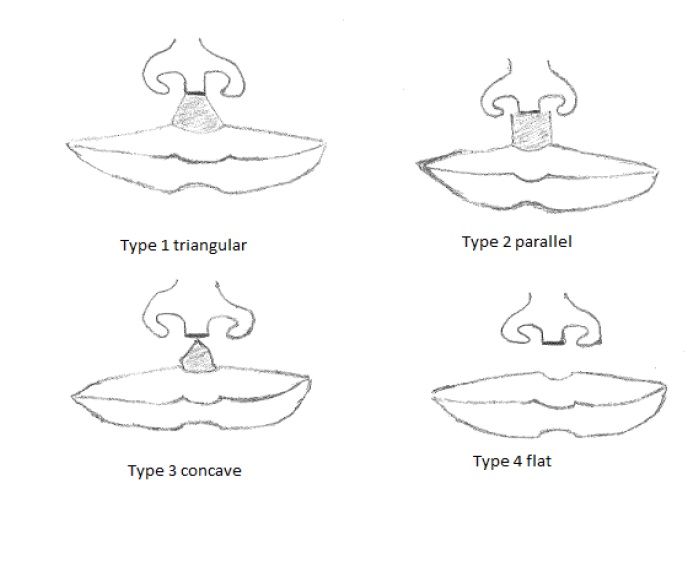
Figure 2: Showing different types of morphology of the philtral column.
Several anatomical dissection studies have demonstrated that the orbicularis oris muscle anatomy constructs the framework for philtral topography. It is composed of two parts: pars peripheralis and pars marginalis, confined within the lip and vermillion border, respectively.
The pars peripheralis and pars marginalis are composed of superficial and deep layers. The deep layer is in continuity with buccinator muscle while the superficial layer is in continuity with the muscles of oral commissure. In the midline, the deep layer is continuous with the opposite side while the superficial layer decussates with the other site and inserts into the dermis of lateral philtral columns. The muscle decussation and insertion into the dermis will raise the skin and pull it out forming the philtral ridges. The levator labii superioris contributes to forming philtral columns through vertical fibers that run parallel to them and insert to vermillion border lateral to median groove. Also, fibers of depressor septii nasii muscle contribute by inserting into the upper philtral ridge.
The muscle decussation at the midline in the absence of dermal insertion will form the median philtrum groove or dimple. Another factor that contributes to the formation of this groove is collagen fibers condensation at midline. The cupid bows are formed by the lifting action of levator labii superioris at vermillion border together with depressing action of orbicularis oris muscle at central tubercle.5,6(Fig.3)
Furthermore, recent studies have demonstrated that the vascular anatomy of the philtrum corresponds to its complex structure and to the mechanism of cleft lip. The vascular arcade composed of left and right philtral arteries arising from superior labial arteries are located at the philtral columns, this arterial arcade together with its membranes lead to compartmentalization of superficial fat pads and separation of philtrum from lateral lips .7
The normal looking philtrum is essential in cleft lip repair surgery, the complex anatomy of the muscle reflects on the three-dimensional topography: the philtral columns dimple, and cupid bows. The philtrum is underdeveloped in unilateral cleft lip and absent in bilateral cases, the muscle is hypoplastic and instead of decussating at midline it is mal-inserted longitudinally along cleft margins resulting in absent philtral ridges and shallow philtral dimple8,9(Fig.3)
Figure 3: One year follow up after cleft lip repair. Orbicularis Oris(O.O) anatomy: in cleft lip, O.O is hypoplastic and mal-inserted along cleft margins, normally O.O is decussated at midline (red line: peripheralis, blue: marginalis, pink: levator labii, yellow: depressor septii). Note the neo-philtral elevation by restoration of normal muscle decussation at midline.
The aesthetic, structural and functional cleft lip repair should apply the main anatomic principles and restore them for the best outcome. Various methods of constructing a philtral ridge have been described for repairs of a unilateral cleft lip like adequate muscle release and rotation from abnormal insertion, re-orientation, and restoration of pars peripheralis decussation at midline.
It is very important to preserve the philtral dimple by avoiding extensive medial muscle dissection so that the muscle dissection on the medial segment must not cross the mid philtrum, muscle eversion at a new philtral column using mattress sutures or by overlapping the lateral muscle over the medial segment. Parsmarginalis reconstruction at Vermillion is very important to avoid whistling and preserve vermillion volume8,9,10,11
In bilateral cleft lip repair, the prolabial flap design must be narrower at the columellar-labial junction (not more than 2 mm) because of progressive widening with growth to avoid the abnormal rectangular shape. The philtral columns elevation can be simulated by lateral strips of de-epithelialized skin on prolabium. 8 (Fig.4)
Figure 4: Three years follow up of bilateral cleft lip repair: note the creation of philtral dimple by muscle decussation at midline and neo-philtral elevation by lateral prolabial de-epithelialized strips.
The philtral ridge can also be augmented with a dermal or fat grafting in secondary cleft lip revisions simulating the increased connective tissue present in the normal ridge.8
Furthermore, philtrum shapes and dimensions with its racial variations must be fully recognized by cleft surgeons. Achieving near normal three-dimensional topography of cleft lip with a fine scar is the final goal of cleft lip repair avoiding the psychosocial stigmata and permitting normal social interaction.
The understanding of the shape of philtrum with its variation among the races is essential in final philtral creation: guide incision during surgery, final scar position, neo-philtral elevation, philtral dimple, and white roll pout. 1,2,8,9
In this prospective study, performed by pediatric dentists and plastic surgeons, we are delineating the different morphologies of philtrum in normal Jordanian pediatric population which will have practical applications in the cleft lip surgery at our center.
Materials and methods
This was a prospective study in 200 Jordanian Children (106 males, 94 females) presented to the dental pediatric clinic at King Hussein Medical center, without any craniofacial anomalies or trauma. All children were of age less than 14 years; the age range 3-14 years and the average age was8.88 years for males and 9years for females.
All medical photographs for each subject were taken using a Samsung S6 edge plus digital camera 16 megapixels. (Samsung South Korea).3 views (frontal, basal and lateral) were taken of each participant and analyzed blindly by three plastic surgeons to determine the shape of the philtrum, using the following points:
1. The peaks of the Cupid’s bow (cphi–cphi)
2. Origin of philtral column at each side(cphs-cphs)
Photos were analyzed using MS Paint program for photos (Microsoft Paint for Windows 7). (Fig.5)
Figure.5: points (cphi-cphi): the peak of cupid bows each side, points (cphs-cphs): the origin of the philtral column each side.
Our classification of the morphology of philtrum was based on modifications of A. Mori et al.ˡ in Japanese children: Type 1-triangular, type 2- parallel, type 3-concave, and type 4 -flat (Fig.2) as described in the introduction section.
Results
The overall most common type of morphology of philtrum was type 1- triangular which was observed in 92 out of 200 children represent 46%. The least common type of morphology of the philtral column observed was type 4-flat, and it accounted for 7 out of 200 children represents 3.5%.
The breakdown of males and females total numbers according to the morphology of the philtral column was as shown in the following table (I).
Table I: showing the breakdown of males and females total numbers according to the morphology of the philtral column.
|
Philtral column type
|
Type 1 Triangular
|
Type 2 Parallel
|
Type 3 Concave
|
Type 4 Flat
|
|
Total number
|
92
|
69
|
32
|
7
|
|
Male
|
47
|
33
|
22
|
4
|
|
Female
|
45
|
36
|
10
|
3
|
Discussion
The lips are very important from both functional and aesthetic standpoints. The aesthetic topography of the upper lip is more sophisticated than the lower lip, therefore, inherent understanding of aesthetic topography and its variations is essential for medical specialties; mainly the plastic surgeons who deal with the reconstruction of congenital and acquired lip defects.1,2,3,4
This is very essential in all cleft lip repair surgeries, especially in geometric cleft lip repairs such as the anatomic subunit cleft lip repair; where the placement of incision point at medial cleft lip segment columellar-labial junction, Cphs point is determined that will reflect on the incision shape at lateral segment, final shape of cleft neo-column and shape of philtral dimple (Fig. 6)
.9,10,11
Figure 6: Geometric cleft lip repair markings and intraoperative results. Note the philtral column shape determination is based on normal side shape, point cphs” on the medial segment and its counterpart on the lateral segment (red dots) which represent the origin of the neo-philtral column is very important. The yellow line represents the incision line.
The results of our study delineate the different morphologies in the philtrum shape of Jordanian children. It will be a synergistic tool for our surgeons in their preoperative markings and planning for better outcomes of the surgery.
Limitations of this study include The quality and limitations of two-dimensional photographic assessments compared to three-dimensional photogrammetric assessments, its sensitivity to the angle at which the photograph is captured and the position of the subject. However, it is cost effective and noninvasive in terms of facial shape evaluation especially if high-resolution medical photography is used. Also, a two-dimensional photographic assessment has a limitation in measuring accurately the anthropometric distance, and if there are true morphological changes related to age, hence there was a need for three-dimensional photogrammetry or lasers system.
Understanding the common philtrum shapes in our population will effectively help plastic surgeons in mirroring the contralateral philtral column in unilateral cases and in designing the prolabium flap in bilateral cleft lip cases. Furthermore, it will also aid in surgeons’ efforts to preserve philtral dimple and to simulate philtral column elevation.
References
1. Mori, A.; Nakajima, T. Kaneko, T.; Sakum, H.; andAokiY.(2005) Analysis of 109 Japanese children’s lip and nose shapes using a 3-dimensional digitizer. British Journal of Plastic Surgery. 58, 318–329.
2. Abdulrasheed, I.and EneyeA.M. (2013)Philtral Columns and Nostril Shapes in Nigerian Children: A Morphometric and Aesthetic Analysis. Plastic Surgery International Volume, Article ID 382754.
3. Tirbod T. F. (2003).An Overview of Facial Aesthetic Units.J Oral Maxillofac Surg.61:1207-1211,
4. Constantinides, J.; Federspil, P.; and Iro, H. (1999) Functional and AestheticObjectives in the Reconstruction of Lip Defects. Facial Plastic Surgery. 15 (4): 337-349.
5. Latham, R. A, and Deaton, T G. (1976 Feb) The structural basis of the philtrum and the contour of the vermilion border: a study of the musculature of the upper lip. J Anat.121 (Pt 1): 151–160.
6. BriedisJ.and JacksonI..(1980)The anatomy of the philtrum: observations were done on dissection of the normal lip. British journal of plastic surgery.34: 128 – 132.
7. Garcia de Mitchell, A.Pessa, J. E. SchaverienM. V., Rohrich, R. J. (December 2008), The Philtrum: Anatomical Observations from a New Perspective. Plastic and Reconstructive Surgery. 122(6):1756-1760.
8. Rogers, C.R.; Meara, J. G.; and Mulliken, J. B. (January 2014).The Philtrum in Cleft Lip: Review of Anatomy and Techniques for Construction. The Journal of Craniofacial Surgery.25, Number (1).
9. Grieves, MR; Camison L; and Losee JE. (2014 Dec). Evidence-based medicine: Unilateral cleft lip and nose repair. Plastic and Reconstructive Surgery. 134(6):1372-80.
10. (2005 Jul); Unilateral cleft lip repair: an anatomical subunit approximation technique. Plastic and Reconstructive Surgery. 116(1):61-71.
11. Tse, R.; and Lien, S (2015) Unilateral Cleft Lip Repair Using the anatomical Subunit Approximation: Modifications and Analysis of Early Results in 100 Consecutive Cases.Plastic and Reconstructive Surgery. 136 (1): 119-130.