In the developing world, anemia is a common problem in pregnancy because of the increased demand of iron (iron demand), needed to accommodate the increasing maternal blood volume and iron needs for the fetus [2].It is likely to be nutritional. [3]Iron deficiency anemia (IDA) is the leading cause of
anemia among pregnant women globally followed by folic acid deficiency despite
all the national recommendations and guidelines for treatment and prevention [4].
Our study concentrates on the following points:
· Is there
screening for IDA during antenatal care? Are pregnant women being counseled
about the benefits and the side effects of the iron supplement?
· Do our
pregnant women take their supplement on daily basis?
· Are they
compliant with the treatment, and if not, why?
Materials and Methods
The data collected
for this study was collected from a cross-sectional survey primarily targeting
patients admitted to the labor ward at King Hussein Medical Center during the
period between February-August 2016. A total of 400 Women were interviewed.
A questionnaire was filled after the consent of the patient,
(Figure 1).
It was completed by an Obstetrics and Gynecology
resident. The questionnaire sought information about sociodemographic
characteristics that included age, educational level for women, and area of residence.General
obstetric characteristics including gravidity,
parity, and birth weight were recorded, as were past obstetric history of anemia,
its previous management and family history of anemia. There were questions regarding
hemoglobin levels at booking and at delivery,
most common symptoms of anemia, compliance with
oral iron supplement sand any side –effects of
treatment.
Patients
were also asked about history of receiving intravenous iron or blood
transfusion. Birth outcomes were also noted.
Fig1:
Questionnaire sample.
Date:
-----------------------
Name: Hospital Number:
--------------------------
Age: --------------------
Parity: --------------------------- Education: ----------------------
Area of residence:
--------------------------------
Family history of
anemia: -------------------------
Smoking:
----------------------
History of anemia
during previous pregnancies and its treatment:
--------------------------------------------
Gestational age
at delivery: ------------------
Hb level at
interview: -------------------------
If anemic, most common
symptoms: ------------------------------------------------------------------------------
Hb level at booking:
----------------------------------------------------------------------
Compliance:
------------------------------------------------------------------------------------------------------------
Side effects:
------------------------------------------------------------------------------------------------------------
Any history of IV
iron or blood transfusion in this pregnancy: ------------------------------------------------
Birth outcome:
---------------------------------------------------------------------------------------------------------
Results
Most of our patients were in the (25-29) year’s
age group (39%), followed by (20-24) years age group (24%). (Chart I).
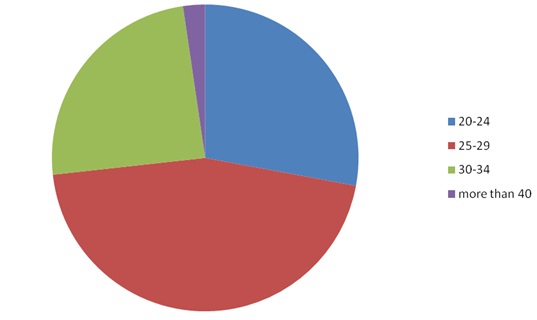
(Chart I ) : Age distribution in the studied sample
Most of the women were primigravidas
followed by the group of parity 1-2, (chart II).
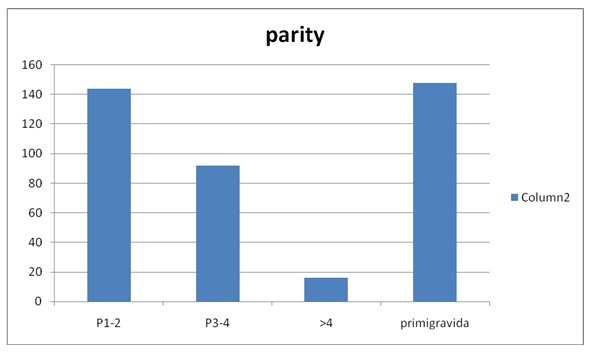
(Chart II): Distribution of parity in the studied
sample
Thirty-five percent of
our patients were university graduates and are employed.
Anemia
was defined as less than 10g/dl was as high as 40% at booking. More than half
of those patients continue to have anemia at term (25%). Less than one third of
them reported anemia symptoms like dizziness, fatigue and general weakness.
Most
of the women took oral iron supplements prescribed by doctors at the Royal
Medical Services (RMS). Twenty-six percent of them took it more than once daily,
(Chart III).
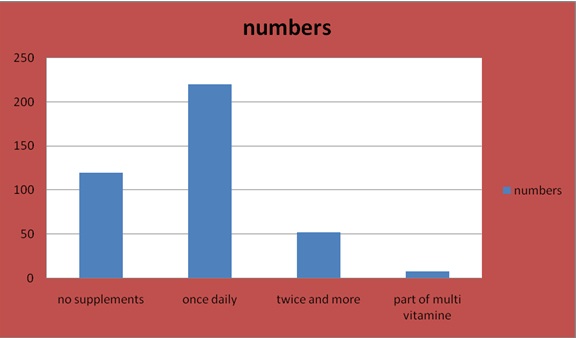
(Chart III): frequency of iron
supplementation in the studied sample.
Sixty-three
percent of patients were not compliant with treatment.
The
most common 2 reasons for non-compliance were nausea (17%) and constipation 13%.Thirty-seven
percent of those reporting nausea discontinued therapy, (Table 1).
Table
(I)
|
Side effect
|
Number of patients
|
|
Nausea
and vomiting
|
68=17%
|
|
Constipation
|
52=13%
|
|
Epigastric
pain and discomfort
Black
tarry stool
|
40=10%
40=12%
|
One
hundred and twenty women did not take any iron, (Chart III). Forty patients received
at least 2 units of blood during their pregnancy or postpartum.15% of anemic
mothers had low birth babies.80% of the women interviewed didn’t have counselling
about the benefits and side effects of the supplement.
All
patients had their Hb checked at booking and at delivery.
15%
had another check when they presented with symptoms of anemia or bleeding.Almost
all of the women received ferrous sulfate as oral iron supplement.
DISCUSSION
UP
to 52% of pregnant women suffer from anemia in developing countries with great
impact on their quality of their lives. If not treated, it can cause maternal
and fetal adverse out comes, [10].
In
ourstudy, screening of hemoglobin level was done at booking visit which is in
first trimester, and at delivery.Anemia was diagnosed in our patients if the HB
is less than 10 g/dl. Ferritin levels were not requested routinely. MCV was
noted in all patients. Recommendations for current practice in the UK are to
assess the mother’s hemoglobin concentration at booking and at 28 weeks’ gestation
(NICE 2008) and ensure there are systems in place to follow up abnormal
results. [11]. this is difficult in our country as we do not have clear
protocols and the antenatal care is not well established in the primary care
system. We should implement guidelines to make sure that anemia among our
patients is not missed.
Checking
Hb in the third trimester is essential because the demand of iron increased to
7.5 mg/day. [12] [13][14] this
predisposes to postpartum iron deficiency, which is associated with decreased
physical abilities , psychic disturbances including emotional instability,
depression, stress, and reduced cognitive performance, [15] [16] [117].
In
addition, mortality rate was higher in women with very low hemoglobin levels.
Also, co-morbidities such as postpartum hemorrhage, acute kidney injury, and
disseminated intravascular coagulation were higher in anemic mothers, [18]. It
is estimated that close to 20% of maternal mortalities are directly linked to anemia
and another 50% of maternal deaths are associated with anemia [19].Anemia is
common among our patients but no mortalities were noted among the study group.
Less than one third of our sample reported symptoms of anemia.
The
World Health Organization (WHO) and Centers for Disease Control (CDC) technical
consultation on the assessment of iron status at the population level concluded
that Hb and ferritin were the most efficient combination of indicators for
monitoring changes in the iron status of a population as a consequence of iron
supplementation (WHO/CDC 2005) but in our study the diagnosis of anemia was
based on HB levels and on MCV readings as ferritin levels were not done
routinely.
Ninety
percent of our women in the study were not informed about the details of the
iron supplement and its benefits, when and how to take it and side effects. They
did not know that the daily diet contains a number of substances (e.g.,
calcium, polyphenols, and phytates) that inhibit the absorption of iron by
approximately 40% [20]. Consequently, ferrous iron supplements should be taken
between meals, preferably with fruit juice.
Containing
vitamin C, which enhances absorption, whereas milk, coffee, and tea inhibit
absorption [18][21].All women should be given dietary information to maximize
iron intake and absorption, and physicians should give more time to council
patients regarding the benefits of iron supplements. Counselling was poor among
the population of ladies we looked at, and we as health care providers should allocate
more time and the skills to counsel patients about anemia, treatment and the
side effects.
From
our study, 63% were non-compliant to oral iron supplement and the most common
reasons for non-compliance were: nausea (17%) and constipation (13%). So
gastrointestinal manifestations are the main factors for non-compliance which
led to 37% of our ladies discontinuing treatment. These side-effects may be
dose dependent.It is generally considered that doses ≤ 50–60 mg iron/day generate less side-effects
than higher doses and that iron given in
controlled release formulations is better tolerated [4][22][23]. However, the
meta-regression analysis shows that there is no statistically significant
dose-response effect.
A
study of Danish pregnant women evaluated the effect of 20, 40, 60, and 80 mg
ferrous iron daily from 18 weeks gestation to delivery. It appeared that a dose
of 20 mg ferrous iron was inadequate to prevent iron deficiency in a
substantial number of women. However, 40 mg ferrous iron prevented IDA in more
than 95% of the women. Furthermore, there were no significant differences in
iron status between women taking 40, 60, and 80 mg elemental iron [8].The Iron
preparations that are available in our hospital contains 60 mg of elemental
iron.
Seventy
percent of our pregnant women were taking the supplements daily, 13% were
taking it more than once. In the United Kingdom, iron supplements are not given
routinely.When the level of ferritin is below 30 microgram/l this should prompt
treatment.If ferritin is 70microgram /l this reflects iron stores larger than
500 mg, so there is no need for treatment, [24].In our patients, supplements
were given to all patients as ferritin levels were not checked routinely and
anemia was common (40% of women at booking).
Twenty
five percent (25%) of our patients were anemic at the time of delivery but if
they have been treated with iron supplements and they were compliant, then this
percentage most likely would have been lower.
As
found after analyzing the questionnaire, 15% of anemic mothers have low birth
babies defined as less than 1.5KG. A meta-analysis summarizing 48 randomized
controlled trials and 44 cohort found that, for each 1 g/L increase in maternal
hemoglobin, neonatal birth weight increased by 14.0g (6.8 to 21.8g) [10]so that
should let us focus on detecting and preventing anemia especially in the third
trimester of pregnancy.
The
Gravidity is an important variable significantly associated with anemia. The
risk of anemia increases as the number of pregnancies increases from 3–5pregnancies
[24], but it is even common in the women who had less than three pregnancies.
This finding is consistent with other studies conducted in SaudiArabia and
India, in which they found that increased number of pregnancies and deliveries
is positively associated with the high risk of developing anemia.[25,26] This
is true among our patients as most of
them are multiparas.
In
our study, anemia at booking was found in 40% of our patients compared to the
developing countries which is 51% [WHO 2004]. This is really high and all these women should
have been checked pre-conceptually. Guidelines are essential to tackle this problem
to make sure that the Hb of these ladies is within normal limits before
conception.Anemia may be relative (physiological) or absolute [27].This may be
due to the low socioeconomic status of some of our patients, this will directly
affect the nutritional status and iron stores which as a result will decrease. This
might explain the high prevalence of anemia among our pregnant population.
Forty
patients received 2 units of blood before delivery with all the risks of blood
transfusions, this is mainly because they presented late in pregnancy with low
HB. No patient received IV iron in our study group. This is something we need
to look at and encourage those ladies to take this treatment.
Most
of our patients had IDA based on Hb and MCV results. We need to implement a
screening program for IDA. More time needs to be spent with our patients
explaining the treatment and the side effects of this treatment. This will
ensure and increase the compliance with the medications.
CONCLUSION
Anemia is a common
problem among our patients. Guidelines and protocols for the management of anemia
in pregnancy should be developed, implemented and audited. The guidelines
should consider both the types of oral iron supplements and recommended
doses.More time should be spent with our patients explaining the risks of anemia,
supplement options and the associated side-effects in order to maximize
compliance. Measurement of ferritin has to be part of the routine assessment of
all patients with anemia.
Limitation
of the study
It’s a retrospective study and the sample size is
relatively small.
References
- WHO. Archived: Iron deficiency
anemia: assessment, prevention and control: A guide
for programme managers,2001:WHO/NHD/01.3
- Trivedi SS, Purl M. New Delhi:
Jaypee Brothers Medical Publishers (P) Ltd; 2010.
Anemia in Pregnancy: Magnitude of Problem, Pharmaceutical; pp. 5–6.
Reprint Ed.
- Geneva: WHO; 1989. [Last accessed 2013 Apr 14]. WHO. Preventing and Controlling Anaemia through Primary Health Care: a Guide for Health Administrators and Programme Managers. Available from: http://www.who.int/nutrition/publications/micronutrients/anaemia_iron_deficiency/9241542497.pdf.
- McDiarmid T, Johnson ED (2002)
Clinical inquiries. Are any oral iron formulations
better tolerated than ferrous sulfate? J FamPract .2002June; 51(6):575-577.
- Crompton DW, Nesheim MC.
Nutritional impact of intestinal helminthiasis during the human life
cycle. Annual Review of Nutrition.2002; 22:35-59. [PubMed]
- Leveno KJ, Cunningham FG, Gant NF,
Alexander JM, Bloom SL, Casey BM et al. Williams Manual of
Obstetrics. Dallas: McGraw Hill, 2003.
- Brabin BJ, Hakimi M, Pellertier D. An
analysis of anemia and pregnancy-related maternal mortality.JNutr. 2001;
131:604S–614S. [PubMed]
- Milman N, Bergholt T, Eriksen L, et
al. Iron
prophylaxis during pregnancy - How much iron is needed? A randomized dose-response
study of 20–80 mg ferrous iron daily in pregnant women. ActaObstetGynecol
Scand.2005 Mar; 84(3):238-47.
- Mohammad A. Salahat, Abdullah I.
Ibrahim.
Prevalence of Anemia among Jordanian Pregnant Women and the Effect of
Early Pregnancy on Alkaline Phosphatase Activity. Jordan Journal of
Biological Sciences.2012; 5(1): 65-70.
- Haider BA, Olefin I, Wang M,
Spiegelman D, Ezzati M, Fawzi WW, et al. Anemia, maternal iron use,
and risk of adverse pregnancy outcomes: systematic review and
meta-analysis. BMJ. 2013; 346:f3443. [PMC free article] [PubMed].
- National Institute for Health and
Care Excellence (NICE). Clinical Guideline 62, Antenatal Care: routine
care for the healthy pregnant woman. National Collaborating Centre for
Women's and Children's Health (UK). London: RCOG Press. 2008. ISBN-13:
978-1-904752-46-2.
- Milman N. Iron and pregnancy—a
delicate balance. Annals of Hematology. 2006; 85(9):559–565.
[PubMed]
- World Health Organization. "Iron
deficiency Anemia: Assessment, prevention and control", WHO/NHD/01.3,
2001.
- Bothwell TH. Iron requirements in
pregnancy and strategies to meet them. American Journal of
Clinical Nutrition. 2000; 72:257S–264S
- Milman N. Postpartum anemia I:
definition, prevalence, causes, and consequences. Annals of Hematology.
2011; 90:1247–1253. [PubMed].
- Beard JL, Hendricks MK, Perez EM,
et al.
Maternal iron deficiency anemia affects postpartum emotions and cognition.
Journal of Nutrition. 2005; 135(2):267–272. [PubMed]
- Corwin EJ, Murray-Kolb LE, Beard
JL.
Low hemoglobin level is a risk factor for postpartum depression. Journal
of Nutrition. 2003; 133(12):4139–4142.
- Ghimire RH, Ghimire S. Maternal and
fetal outcome following severe anemia in pregnancy: Results
from Nobel Medical College Teaching Hospital, Biratnagar, Nepal.J Nobel
Med Coll. 2013;2(3):22-26. Doi: 10.3126/jonmc.v2i1.7668
- Anand T, Rahi M, Sharma P, Ingle
GK.
Issues in prevention of iron deficiency anemia in India. Nutrition
2014; 30:764–770.
- Hallberg L, Rossander L, Skaanberg
AB.
Phytates and the inhibitory effect of bran on iron absorption in man. American
Journal of Clinical Nutrition. 1987; 45(5):988–996. [PubMed]
- Hallberg L, Brune M, Rossander L. Iron
absorption in man: ascorbic acid and dose-dependent inhibition by phytate.
American Journal of Clinical Nutrition.1989 Feb; 49(1):140-144.
- Souza AI, Batista Filho M, Bresani
CC, Ferreira LOC, Figueroa JN (2009) Adherence and side effects
of three ferrous sulfate treatment regimens on anemic pregnant women in
clinical trials.CadSauda Publica.2009June;25(6):1225-33.
- Cad SaudePublica 25: 1225–1233. 54.
Liguori L (1993) Iron protein succinylate in the treatment of iron
deficiency: controlled, double-blind, multicenter clinical trial on over
1,000 patients. Int J ClinPharmacolTherToxicol 31: 103–123. [PubMed]
- PavordS, MyersB, Robinsons, AllardS,
Strong J. UK guidelines on the management of iron deficiency in pregnancy. Br J
Haematol.2012 Mar: 156(5):588-600.
- Elzahrani SS. Prevalence
of iron deficiency anemia amongpregnant women attending antenatal clinics
at Al-Hada Hospital. Canadian J Med. 2012; 3(1):10–14.
- Vivek RG, Halappanavar AB, Vivek
PR, HalkiSB,Maled VS, Deshpande PS. Prevalence of Anemia andits
epidemiological. Determinants in Pregnant Women.2012; 5(3):216–223.
- Bukar M, Audu BM, Sadauki HM,
Elnafaty AU, Mairiga AG. Prevalence of iron deficiency and
megaloblastic anemia at booking in a secondary Health facility in North
Eastern Nigeria.Nigerian Journal of Medicine. 2009; 50(2):33–37