ABSTRACT
Neonatal hypocalcemia is the most prevalent type of hypocalcemia encountered by pediatricians. A fall in total calcium below 7.5 mg/dL or ionized calcium concentration below 4.4 mg/dL (or 1.1 mmol/L) usually defines neonatal hypocalcemia.
Neonatal hypocalcemia categorized into early hypocalcemia (within the first72 hour) and late hypocalcemia (occurs after 3-4 days to 6 weeks of life).
The mechanisms for neonatal hypocalcemia are unclear, but may represent a delayed response to the rise of parathyroid hormone (PTH) following hypocalcemia.
Objective: to determine the frequency of early and late neonatal hypocalcemia and the most common risk factors in the development of neonatal hypocalcemia.
Methods: A retrospective study was conducted at the neonatal ward of Prince Zaid Bin Al Hussein Military Hospital (Tafila-Jordan) from June 2018 to May 2019.
The total number of Ninety-four neonates with or without clinical manifestations of hypocalcemia were included in this study from 3542 deliveries, by year, admitted to neonatal units at Prince Zaid Bin Alhussien Military Hospital.
Clinical data were analyzed in terms of gender, gestational age (GA), type of delivery, birth weight, perinatal history, signs, and symptoms at diagnosis of hypocalcemia, and Apgar score at the first minute.
Total serum calcium, magnesium, albumin, phosphorus, total bilirubin, and glucose levels were measured. Arterial blood gas and chest radiographs were measured.
In all hypocalcemic infants, serum calcium levels and blood samples were obtained before calcium therapy.
We explain the major risk factor to develop neonatal hypocalcemia: premature baby (< 37 weeks of gestational age), low birth weight (< 2500gram), neonatal asphyxia is a condition characterized by an impairment of exchange of the respiratory gases resulting in hypoxemia, hypercapnia and metabolic acidosis.
We excluded all neonates with congenital anomalies or metabolic syndromes.
For statistical evaluation, we used the Microsoft Excel 2010 software and SPSS version 18.
Results: Ninety-four neonates admitted to the neonatal ward were ascertained with a final diagnosis of neonatal hypocalcemia.
Fifty-seven were male (60.6%). Thirty-seven (39.4%) were female. Of all mothers, 70.2% delivered their infants through Cesarean Section (CS) and 29.8% had gone through normal vaginal delivery (NVD), and the mean birth weight was 2388 ± 1383 g.
Four neonates (4.26%) had neonatal asphyxia, 47 had premature and low birth weight (51.06%), and 5 cases had diabetic mothers (5.32%).
Sixty cases (63.8%) had early hypocalcemia, while 34 (36.2%) had late hypocalcemia. Seven cases presented with convulsion, six cases presented with muscle twitch and four cases with poor feeding.
There was a statistically significant prevalence of early and late hypocalcemia among neonates who had a low first minute Apgar score (≤ 5) (P = 0.02, P = 0.03).
Conclusion: The frequency of early hypocalcemia is more common than late hypocalcemia, and the most common risk factors associated with transient hypocalcemia are premature, birth asphyxia, low birth weight, and diabetic mothers.
Keywords: frequency, early neonatal hypocalcemia, Late neonatal hypocalcemia, Apgar score.
RMS April 2020;27(1): 10.12816/0055462
Introduction
Calcium is measured as total calcium, comprising protein-bound and ionized forms. Ionized calcium, the form that causes physiological effects, comprises about 50% of total serum calcium. Of the remainder, 40% circulates bound to albumin and globulin, and about 8 to 10% is complexed into organic and inorganic acids (e.g., citrate, lactate, bicarbonate, sulfate, and phosphate). (1) Serum calcium is regulated within close limits by several hormones that balance gastrointestinal intake with urinary or fecal loss; the skeleton serves as a store of calcium so that it may be mobilized when needed or stored if necessary. (2) In calcium metabolism disorders, excessive calcium may be removed from the bone, or deficiency in various factors may impair bone formation, leading to bone diseases. (3) Hypocalcemia may be defined as serum Ca below as 7.5 mg/dL and ionized Ca below 4.4 mg/dL(or 1.1 mmol/L) if birthweight is over 1,500 g, or as serum Ca below 7 mg/dL and ionized Ca below 3.6 mg/dL (0.9 mmol/L) if birthweight is under 1,500 g. (4) Symptoms of hypocalcemia are more nonspecific in newborns than in older children; poor feeding, emesis, and apnea may be the only signs. More specific signs of hypocalcemia that might be found in older infants include tachycardia, irritability, jitteriness, tetany, laryngospasm, and seizures. (5) Neonatal hypocalcemia is categorized as early and late hypocalcemia according to its onset. Early hypocalcemia often occurs within the first 72 hours of life while the late form occurs after 3-4 days to 6 weeks of life. (6) Early hypocalcemia is more prevalent than late hypocalcemia, especially in neonates weighing less than 2.5 kg or premature babies or infants of diabetic mothers. (7) In early hypocalcemia, the physiological fall in plasma calcium is exaggerated, especially in the preterm infant, following birth asphyxia, in “sick” infants, and those born to diabetic mothers. The mechanisms for late neonatal hypocalcemia are unclear but may represent a delayed response to the rise of PTH following hypocalcemia. (2,8) With severe symptoms, including seizures, intravenous (i.v) 10% calcium gluconate (equivalent of 9.3 mg/mL of elemental calcium) in a dose of 100 mg/kg or 1 mL/kg infused over 15 min with a total dose no more than 20 mg of elemental calcium per kilogram is used. (9) A repeated dose may be administered after 10–15 min for every 6 hours if there has been no response to the symptoms, but only if clinically indicated for continued hypocalcemia. Maintenance intravenous calcium is 500 mg/kg/day of 10% calcium gluconate. (10)
Methods
A retrospective review study was conducted at the neonatal ward of Prince Zaid Bin Al Hussein Military Hospital from June 2018 to May 2019.
The total number of ninety-four newborns with or without clinical features of hypocalcemia was included in this study of 3,542 births during the year.
Serum calcium levels were measured, and their demographic and corresponding data, including gestational age, sex, APGAR score at first minute, birth weight, early hypocalcemia, and late hypocalcemia were obtained.
Hypocalcemia may be defined as a serum Ca below as 7.5 mg/dL and ionized Ca below 4.4 mg/dL(or 1.1 mmol/L) if birth weight is over 1,500 g and below 7 mg/dL and ionized Ca below 3.6 mg/dL (0.9 mmol/L) if birth weight is under 1,500 g. (4)
In the study, those with hypocalcemia were detected, and the findings were statistically analyzed.
All patients underwent the following tests: full blood count, calcium, phosphorus, alkaline phosphatase, albumin, magnesium, Arterial blood gas, and blood culture.
Results
Of
the 94 neonates, 57 (60.64%) were
male, and 37 (39.46%) were female,
as shown in figure (1). The mean birth weight was 2388±1383.
Figure (1).
Of
all mothers, 66 cases (70.2%) delivered their infants through Cesarean Section
(CS), and 28 (29.8%) had gone through normal vaginal delivery (NVD).
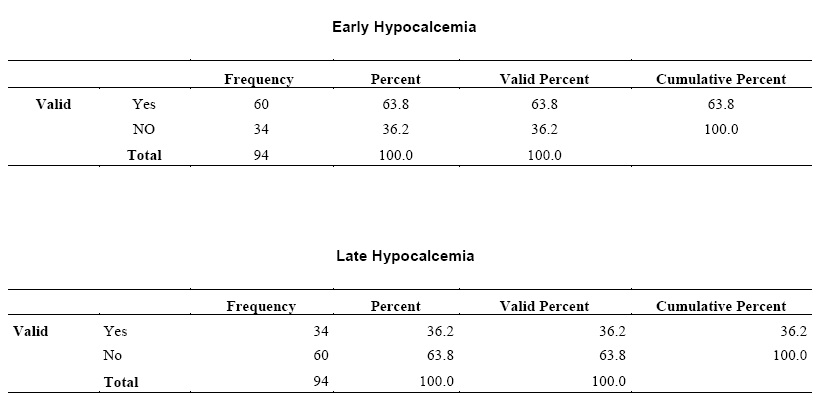
Sixty
cases (63.8%) had early hypocalcemia, while 34 (36.2%) had late hypocalcemia,
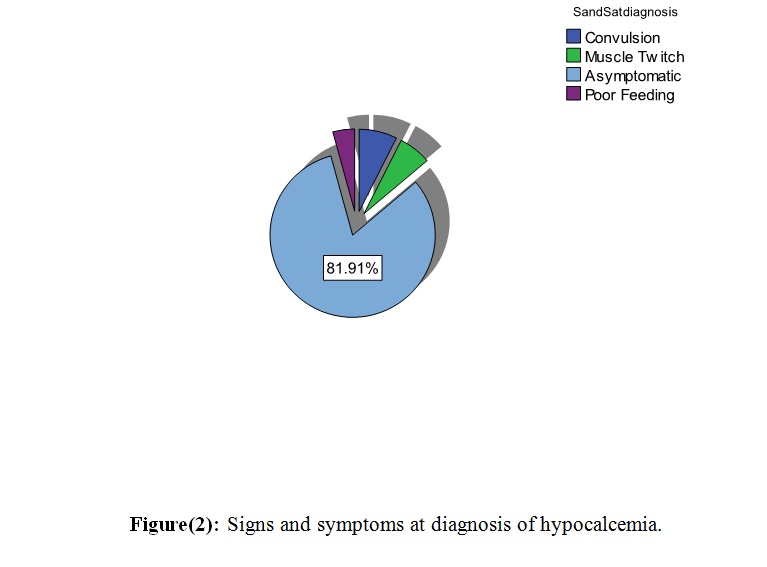
as shown in table I. Seven cases (7.4%)
presented with convulsion, six (6.4%)
presented with muscle twitch and four (4.3%)
with poor feeding, and 77 were (81.9%)
asymptomatic, as shown in figure (2).
|
Table I:
Frequency of early and late neonatal hypocalcemia
|
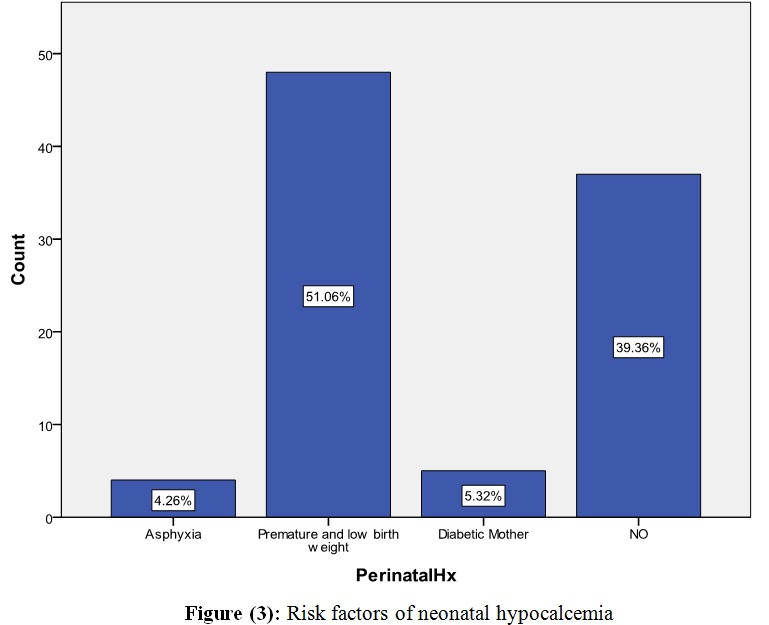
Four neonates (4.26%) had neonatal
asphyxia, 47 were premature and had low birth weight (51.06%), and 5 had diabetic
mothers (5.32%), as shown in Figure (3).
There was a statistically
significant prevalence of early or late hypocalcemia among
neonates who had a low first minute Apgar score (≤ 5)
(P = 0.02, P = 0.03).
Also, there were significant relationships between the frequency
of hypocalcemia and preterm infants (P = 0.004).
However,
no significant relationship was found between neonatal gender and type of
delivery and frequency of hypocalcemia.
Discussion
Our objective in this study was to determine the
frequency of early and late neonatal hypocalcemia and the most common risk
factors in the development of neonatal hypocalcemia as early detection and management
of hypocalcemia in neonates can prevent subsequent severe complications.
The results of this research showed that approximately 63.8%
of the neonates developed early
hypocalcemia, while 36.2% developed late hypocalcemia. In
a research conducted in Tehran, Iran, the frequency of
hypocalcemia in infants was 63% for early hypocalcemia and 37% for late hypocalcemia, which
is comparable to the findings of this research. (11)
In another study in 2018 in Amritsar, India,
it was reported that 55% had early hypocalcemia and 45% had late hypocalcemia. (12)
According to the results of our
study, most neonatal hypocalcemia (81.9%) were without
clinical signs, and the rest (18.1%) were symptomatic. In
reference to textbooks, most neonatal hypocalcemia has been confirmed to be asymptomatic,(13,14)
but no statistic has been presented in this respect. Seizures
were the most common symptom in early and late hypocalcemia, and
this result is in agreement with a study conducted at the Seoul National University Bundang Hospital. (15)
Cakir et al. also reported that neonatal hypocalcemia might present
different symptoms such as hypotonia, poor feeding, stridor, and jitteriness,
yet the most alarming symptom was seizure activity. (16)
Based
on our results, early and late hypocalcemia were more frequent in premature
infants, neonates with a one-minute Apgar score of five or less, birth asphyxia,
low birth weight, and infants of diabetic mothers. In
accordance with our results, Khalesi et al. confirmed that premature infants, those with low birth weight, birth asphyxia, infants
of diabetic mothers, and those with low
first minute Apgar scores (< 5) had
lower serum Calcium. (11)
We think it is possible to prevent problems such as
prematurity, low birth weight, and birth asphyxia and consequent hypocalcemia
of infants with better care during pregnancy and before delivery. Paying close
attention to these problems and timely recognition of hypocalcemia and
appropriate management will prevent the undesirable consequences of this disease.
On the other hand, there was no statistical association between
serum calcium levels and gender or type of delivery.
This result is in agreement with the studies of Khalesi et al. (11)
and Thomas
et al. (17)
Limitations
Our study had some
limitations. Firstly, we did not assess
other factors such as
vitamin D and parathyroid hormone levels,
though
the latter affects neonatal serum calcium levels. Also,
maternal
serum calcium and vitamin D were not assessed in this study. Thus, all the
factors associated with hypocalcemia could not be presented. Further studies
are needed to assess these factors.
Conclusions
The current study concludes that neonatal hypocalcemia,
especially early-onset hypocalcemia, is widely prevalent.
The current study also shows the importance of the
evaluation, early detection, and management of hypocalcemia in neonates in
preventing subsequent severe complications.
References
1. Abrams S and Tiosano D. Disorders
of Calcium, Phosphorus, and Magnesium Metabolism in the Neonate. In: FANAROFF
AND MARTIN ’ S NEONATAL-PERINATAL
MEDICINE Diseases of the Fetus and Infant. 10th editions. ; 2016:1460-1489.
2. Allgrove J. The parathyroid and
disorders of calcium metabolism. In: Clinical Pediatric Endocrinology.
Fifth Edit. ; 2005:254-279.
3. Greenstein B. Ben Greenstein
Diana Wood. In: The Endocrine System at a Glance. ; 1994:88-93.
4. Styne D. Disorders of Calcium
Metabolism and Bone. In: Pediatric Endocrinology Review. ; 2016:123-158.
5.Khosla S. HYPERCALCEMIA AND
HYPOCALCEMIA. In: HARRISON’s ENDOCRINOLOGY. 4th edition. ; 2017:442-445.
6. Gomella T. Cunningham D. Eyal F. Calcium
Disorders (Hypocalcemia, Hypercalcemia). In: NEONATOLOGY Management,
Procedures, On-Call Problems, Diseases, and Drugs. 7th edition. ;
2013:576-581.
7. Sinha S. Miall L. Jardine L. Endocrine
and metabolic disorders. In: Essential Medicine Neonatal. Sixth edit. ;
2018:268-286.
8. Jain A, Agarwal R, Sankar MJ,
Deorari A, Paul VK. Hypocalcemia in the newborn. In: Indian Journal of
Pediatrics. ; 2010.
9 . Doyle D. Hypoparathyroidism. In: Nelson
Textbook of Pediatrics. Vol 286. 21st ed. ; 2021:11520-11532.
10. Abrams SA. Abnormalities of Serum Calcium
and Magnesium. In: MANUAL OF NEONATAL CARE. 6th Editio. ; 2008:297-303.
11. Khalesi N, Namiranian P,
Samavati S, Farahani Z. The Frequency of Early and Late Hypocalcemia Among
Hospitalized Newborns in An Iranian Hospital. Shiraz E-Medical J. 2015;16(6):16-18.
12. Aggarwal K, Sandhu S, Narang G
KG. Prevalence of Neonatal Hypocalcemia and its relation to
Supplementation. Int J Curr Res Biol Med. 2018;3(10):43-47.
13. Song BJ, Kim HS, Kim WD. Causes
and Clinical Features of Transient Hypocalcemia in Newborn: A Single-Center
Study. Neonatal Med. 2016;23(3):137.
14. Kelly A and Levine M.
Disorders of Bone and Mineral Metabolism. In: Pediatric Practice
Endocrinology. Second edition. ; 2010:191-256.
15. Teaema FH, Al Ansari K. Nineteen
Cases of Symptomatic Neonatal Hypocalcemia Secondary to Vitamin D Deficiency: A
2-Year Study. J Trop Pediatr. 2009.
16. Çakır U, Alan S, Erdeve Ö, et
al. Late neonatal hypocalcemic tetany as amanifestation of unrecognizedmaternal primary hyperparathyroidism. Turk J Pediatr. 2013:438-440.
17. Thomas TC, Smith JM, White PC,
Adhikari S. Transient Neonatal Hypocalcemia: Presentation and Outcomes. Pediatrics.
2012.