ABSTRACT
Background: Many studies had evaluated the association between obesity and vitamin B12 deficiency, with most having shown low vitamin B12 levels in obese and overweight people. Moreover, there is increasing evidence that susceptibility to vitamin B12 deficiency may change depending on gender and throughout life, with older males having the greatest risk. Obese patients are more prone to insulin resistance (IR); the correlation between low B12 in obese individuals and IR has been evaluated, with conflicting results. The treatment of obese individuals by bariatric surgery and other options may result in multiple nutritional deficiencies and a low baseline B12 level makes them more vulnerable to B12 deficiency.
Purpose: to investigate the relationship between vitamin B12 deficiency, body mass index and age in Jordanian adult patients.
Methods: A cross-sectional study of patients attending the Internal Medicine Outpatient clinics at Jordanian Royal Medical Services hospitals was conducted from June to December 2018. Patients living in different regions of Jordan and between the ages of 14 and 90 years were included. Height (cm), weight (kg) and body mass index (BMI) were recorded.
Result: The study enrolled 301 patients. The mean age was 52.19 years. Overall, 70.8% were in the adult group and 27.2% were in the senior adult group. The mean BMI was 29.41 (SD 5.74) and 36.9% were overweight, 25.2% were class 1 obese, 19.6% were of normal body weight, 11.3% were class 2 obese and 5.3% were class 3 obese. A significant positive correlation between BMI and age was observed (r=0.233; P<0.001). The mean B12 level was 278.82pmol/L. B12 deficiency was observed in 53.8% of patients. A significant negative correlation between BMI and serum B12 was observed (r =-0.123, P=0.032). There was no significant difference between males and females with regard to mean B12 level. A statistically insignificant negative correlation was observed between B12 level and age.
Conclusion: Lower vitamin B12 levels are associated with higher BMIs. No significant difference between males and females with regard to mean B12 level was reported. Further studies are recommended to provide more information about B12 deficiency and its association with BMI and other factors.
Keywords: vitamin B12, Deficiency, Jordan, obesity.
JRMS August 2020; 27(2): 10.12816/0055808
Introduction
Vitamin B12 is naturally found in animal products, including fish, meat, poultry, eggs and dairy products. The normal level of B12 in serum is considered by most laboratories to be 200 to 900 ng per mL (1). Individuals with low dietary meat or animal product intake, vegetarians and those with malabsorptive disorders are vulnerable to vitamin B12 deficiency (2).
Vitamin B12 deficiency is a worldwide problem (2), and is
common in the Jordanian population. El-Khateeb and colleagues conducted a study
of 5640 Jordanian subjects and reported that one third of Jordanian adults have
vitamin B12 deficiency (3). B12 deficiency can present with a spectrum of
diseases ranging from asymptomatic to serious haematological, neurological and
psychiatric complications, as well as a possible risk of irreversible
neurological damage (4). Another study, which was conducted on a total of 838
patients in a Jordanian hospital, showed that vitamin B12 deficiency is
associated with memory impairment (5).
Obesity is a chronic and complex disease and is defined as
an excess of body fat. It is associated with many medical problems, including
an increased risk of metabolic syndrome, diabetes mellitus (DM), cardiovascular
diseases, and mechanical disorders (6). The prevalence of obesity in Jordanian
adults has increased at an alarming rate (7). Because raised BMI is a major
risk factor for many diseases, studies are being conducted to look for health
risks predisposed by obesity. In 2006, Kimmos and colleagues found that there
are alterations in the absorption, metabolism and excretion of micronutrients
in obese and overweight persons (8).
Obesity
and vitamin B12 deficiency are common health problems encountered in healthcare
settings. Many studies have evaluated the association between obesity and
vitamin B12 deficiency, with some having shown low vitamin B12 levels in obese
and overweight people (9, 10, 11). Moreover; there is increasing evidence that
the susceptibility to vitamin B12 deficiency may change depending on gender and
throughout life, with older males having the greatest risk and highest
susceptibility (12, 13, 14). Based on the literature, we hypothesized that
there is a negative correlation between BMI and low serum B12 levels and conducted
a study with the purpose of investigating the relationship between vitamin
B12 deficiency and BMI, age, and gender among the Jordanian adult population.
Methods
A cross-sectional study was conducted of Jordanian adult
patients attending Internal Medicine outpatient clinics at Royal Medical
Services hospitals during the period from June to December 2018. Patients
living in different regions of Jordan and between the ages of 14 and 90 years
were included. Patients were excluded if they are vegetarian, using vitamin supplements,
if treated by metformin, or
corticosteroids, are pregnant, or are known to have DM or malabsorption
diseases. The socioeconomic status and it’s relation to vitamin B12 level was
not analyzed, as most patients refused to give information regarding their
income.
All
included patients signed a consent form after the aim of the study was
explained to them. Height (cm) and weight (kg) were recorded and body mass
index (BMI) was calculated using the following formula: kg/height (m2).
Blood samples were taken to determine vitamin B12 levels. According to the WHO
classification of obesity, patients were classified as mild thin (BMI of
17–18.5), normal (BMI of 18.5–25), overweight (BMI of 25–30), obese class 1
(BMI of 30–35), obese class 2 (BMI of 35–40), and obese class 3 (BMI of >40)
(21). The subjects were classified into three age groups: children and
adolescents (<19 years), adults (19–64 years) and senior adults (65 years
and above). Three descriptive cut-off points of vitamin B12 were used: normal
(>250pmol/L), low (150–249pmol/L), and acute deficiency (<149pmol/L)
(15).
Data
were analyzed using SPSS 16.0 (SPSS Inc., Chicago, IL, USA). Bivariate
correlation tests with Pearson's correlation coefficient were used to assess the
association between vitamin B12s level and BMI, with probability values of
p<0.05 being considered significant. The study was approved by the ethics
committee of the Royal Medical Services.
Results
The study enrolled 301 patients from different
regions of Jordan. The majority, 197 (65.4%), were female, and 104 (34.6%) were
male. Patients’ ages ranged from 14 to 88 years, with a mean age of 52.19
years. Overall, 213 (70.8%) patients were among the adult age group (19–64
years), 82 (27.2%) patients were in the senior adult age group (>65 years)
and 6 (2%) were younger than 19 years. Table II
The mean BMI was 29.41 (SD 5.74). Overall, 111(36.9%)
patients were overweight, 76 (25.2%) patients were class 1 obese, 59 (19.6%)
were of normal body weight, 34 (11.3%) were class 2 obese, 16 (5.3%) were class
3 obese and 5 (1.7%) patients were mild thin. Female patients fell within the
overweight and obesity categories more often than male patients, with a mean
BMI of 28.24 and 30.03 for males and females, respectively. In addition, in the
adult age group, there were 48 females versus 28 males who were overweight, and
71 females versus 23 males who were obese (class 1, 2 and 3). In the senior
adult group, 18 males versus 16 females were overweight, and 11 males versus 21
females were obese (class 1, 2 and 3) (table III). The correlation between BMI
and age showed a significant positive correlation (r =0.233; P<0.001),
reflecting an increase in BMI with increasing age (Table I).
|
Table I: Correlations between age, B12 levels
and BMI
|
|
|
Age
|
B12 level
|
BMI group
|
|
Age
|
Pearson Correlation
|
1
|
-0.051-
|
.233**0
|
|
Sig. (2-tailed)
|
|
.3820
|
.0000
|
|
N
|
301
|
301
|
301
|
|
Vitamin B12 level
|
Pearson Correlation
|
-0.051-
|
1
|
-0.123*
|
|
Sig. (2-tailed)
|
0.382
|
|
.0320
|
|
N
|
301
|
301
|
301
|
|
BMI group
|
Pearson Correlation
|
0.233**
|
-0.123*
|
1
|
|
Sig. (2-tailed)
|
.00000
|
0.032
|
|
|
N
|
301
|
301
|
301
|
|
**. Correlation is
significant at the 0.01 level (2-tailed).
|
|
|
*. Correlation is
significant at the 0.05 level (2-tailed).
|
|
Table II: Mean B12 level, BMI and age
|
|
|
Age
|
BMI
|
B12 level
|
|
Mean
|
52.19
|
29.4137
|
278.8256
|
|
Std. Deviation
|
17.785
|
5.74594
|
169.05770
|
|
Minimum
|
14
|
16.10
|
.000
|
|
Maximum
|
88
|
51.36
|
1402.00
|
Table III: Number of subjects in
each BMI category correlated to age and sex
|
|
Obesity category and number of
subjects
|
|
Age group and Sex
|
Class 1 obese
|
Class 2 obese
|
Class 3 obese
|
Mild thin
|
Normal BMI
|
Over weight
|
|
Children
& adolescent (<19yrs)
|
Males
|
0
|
0
|
0
|
0
|
1
|
0
|
|
Females
|
0
|
0
|
0
|
1
|
3
|
1
|
|
Adult (19–64yrs)
|
Males
|
18
|
5
|
0
|
1
|
12
|
28
|
|
Females
|
37
|
21
|
13
|
2
|
28
|
48
|
|
Senior adult
(>65yrs)
|
Males
|
10
|
1
|
0
|
1
|
9
|
18
|
|
Females
|
11
|
7
|
3
|
0
|
6
|
16
|
The mean level of serum B12 was 278.82 pmol/L (SD:169.05)
among all subjects (Table I). B12 deficiency was observed in more than half of
patients; in total, 130 (43.2%) patients had low B12 levels (150–249pmol/L), 32
(10.6%) patients had acute deficiency (<149pmol/L) and 138 (45.8%) had
normal B12 levels (>250pmol/L) (Figure 1). Among all of the age groups, the
mean levels of vitamin B12 were: 281.7 pmol/L, 265.7 pmol/L, and 354.8 pmol/L
in the adult group, senior adult group, and children and adolescents group,
respectively (Figure 2). There were significantly lower B12 levels among obese and
overweight individuals compared to normal weight subjects (Figure 3). A
significant and negative correlation between BMI and serum B12 was observed (r
=-0.123, P=0.032) (Table I), and higher BMI remained an independent predictor
of lower serum B12 upon correlation analysis. On the other hand, there was no
significant difference observed between males and females in mean B12 level
(Table IV), as there was a statistically insignificant negative correlation
between B12 level and age (r=-0.051; P>0.05) (Table 1). The mean B12 levels
for male and female patients of the different BMI groups are shown in Table IV.
|
|
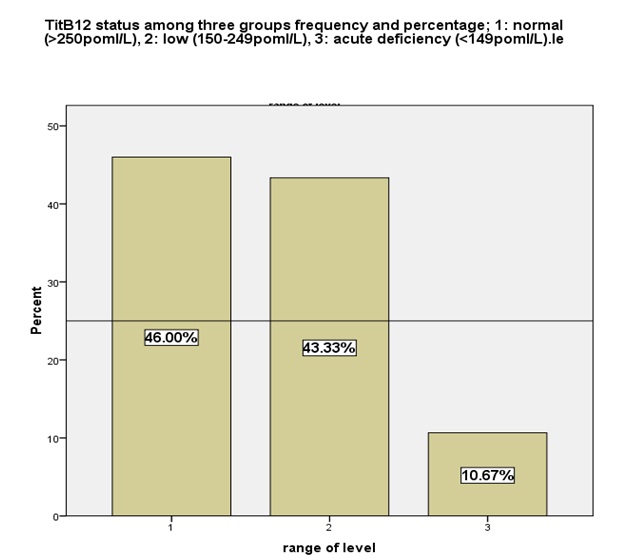
Figure 1: The percentage of each descriptive cut-off
point of B12
status: 1 - normal (>250pmol/L), 2 - low
(150- 249pmol/L), 3 – acute deficiency (<149pmol/L).
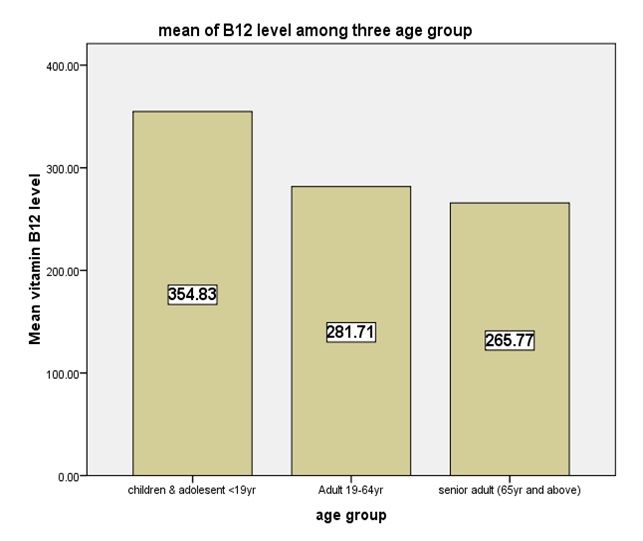
Figure 2: The mean B12 levels of the three age groups
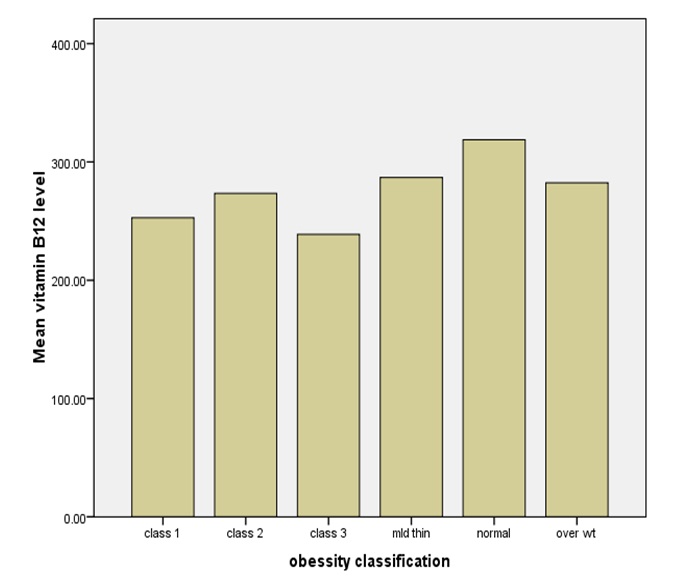
Figure 3:The mean B12 levels among differentcategories
Table IV: the mean of B12 level
for different BMI groups among male and female subjects
|
|
BMI
category
|
|
|
Obese Class 1
|
Obese Class 2
|
Obese Class 3
|
Mild thin
|
normal
|
overweight
|
|
Mean
B12
|
Sex
|
Males
|
231.70
|
281.50
|
-
|
196.50
|
329.90
|
285.36
|
|
|
Females
|
265.21
|
271.70
|
238.84
|
347.00
|
312.20
|
280.32
|
Discussion
The association of B12 deficiency and
obesity has been evaluated in several studies worldwide, as well as among the
Jordanian population. A study carried out on Turkish women found that B12 level
was negatively correlated with BMI (15). In 2018, a cross-sectional study
enrolled 2403 healthy Indian school adolescents and found that B12 deficiency
is associated with high BMI; more than half (51.2%) of obese adolescents were
vitamin B12-deficient (11). Abu-Samak and colleagues enrolled 120 Jordanian
young adults in a study in 2008 which showed lower levels of B12 in overweight
but not obese youths (10). These results may explain some of the findings of
our study, which demonstrated that low levels of serum vitamin B12 were more
prevalent among both obese and overweight adults, than in those who have a
normal body weight, with the lowest mean B12 level observed in obese class 3
individuals.
The
maintenance of an optimal status of vitamin B12 is not only dependent on
adequate dietary intake, but more critically on effective absorption, which
diminishes with age (16). The results of our study showed an insignificant
negative correlation of B12 level and age, as well as a significant positive
correlation between BMI and age i.e. BMI increases with age. Figure 2 shows
that the mean B12 level was higher in the adult age group than in the senior
adult group. Loikas et al. and Sánchez
et al. showed a high prevalence of
B12 deficiency among older adults (12, 14). These findings become interesting
when correlated with the fact that aging is associated with increased risks to
different diseases, and the presence of vitamin B12 deficiency may complicate the
health condition further, or be complicated and unmasked by the treatments of
such diseases; e.g. DM diagnoses increase with increasing age, and metformin,
which is commonly used for DM management, can cause B12 malabsorption (17)
which may deteriorate the neurological complications associated with DM, such
as diabetic neuropathy.
Obesity
is well-known to induce insulin resistance (IR) and increase the risk of DM.
Dursun et al. conducted a study of 110 children aged 10–16 years and found that
vitamin B12 levels were significantly lower in obese children with IR (18).
Accordingly, in addition to screening for IR and other co-morbidities in obese
patients, vitamin B12 levels might also need to be investigated, especially
before starting metformin therapy for obesity-induced IR. Furthermore, the
presence of low levels of vitamin B12 among obese and overweight patients
warrants investigation of the effects of B12 on insulin sensitivity. As a
result of insufficiency in the synthesis of methionine by inducing the leakage
of cellular folate, B12 deficiency increases stress in the endoplasmic
reticulum by causing a deficiency of the oxidation of free fatty acids; because
B12 is a cofactor in the conversion of methylmalonic acid to succinylcholine,
methylmalonic acid accumulates in B12 deficiency, and can cause lipogenesis and
insulin resistance (18).
Generally,
treatment approaches for obesity include lifestyle modifications, medical
treatments with drugs suppressing appetite or decreasing intestinal absorption,
and surgical interventions such as bariatric surgery. Obesity treatment can
lead to multiple nutritional deficiencies, especially with bariatric surgery
(19). The presence of low B12 levels in obese patients may make them more
vulnerable to B12 deficiency following bariatric surgery and other treatment
options, leading to unfavorable results. Therefore, we suggest evaluation of
obese patients for B12 deficiency, especially those intending to lose weight by
any of the different approaches, and to offer B12 supplements for those with
low or deficient levels before introducing obesity management, even if
asymptomatic.
Although our study and
others had shown lower levels of B12 with increasing BMI, some studies had
shown the opposite or found no correlation between B12 levels and BMI. El-Qudah
and colleagues conducted a study of 84 Jordanian healthy adults and found that
the concentration of B12 appears to increase as BMI increases (1). Another
study, which enrolled 100 patients to investigate the relationship between
obesity and serum Vitamin B12, folic acid and vitamin D concentrations in obese
adults, did not find any significant correlation between B12 levels and
obesity (20).
These contradicting results
might be related to the number of subjects included, as small samples might not
reflect the association properly, necessitating larger studies to be
conducted. Moreover, methylmalonic acid
and homocysteine levels, which are more sensitive to B12 deficiency, were not
evaluated in our study; and given the number of subjects we evaluated, we
recommend additional studies involving larger cohorts to assess the relation
between BMI and B12, along with other serum parameters, and to assess the
possible role of B12 deficiency in inducing IR observed in obese patients.
Conclusion
Lower vitamin B12 levels were associated
with overweight and obesity, with the lowest mean B12 level observed in obesity
class 3. No significant difference between males and females was found for mean
B12 level, and a statistically insignificant negative correlation between B12
level and age was observed. The evaluation of obese and older patients for B12
deficiency, especially those intending to lose weight, needs to be considered.
Further studies are recommended to provide more information about B12
deficiency and its association with BMI and other factors.
References
1. El-Qudah JM, Dababneh BF, Al-Qudah MM, et al. Serum vitamin B12 levels related to weight status among healthy Jordanian students. Laboratory Medicine[Internet].2013;44:34–39. https://doi.org/10.1309/LMG2E7PEDHET5QVI
2. Nagao T, Hirokawa M. Diagnosis and treatment of macrocytic anemias in adults. Journal of General and Family Medicine [Internet]. 2017;18(5): 200–204. doi: 10.1002/jgf2.31
3. El-Khateeb M, Khader Y, Batieha A, Jaddou H, Hyassat D, Belbisi A, Ajlouni K: Vitamin B12 deficiency in Jordan: A population-based study. Ann Nutr Metab [Internet]. 2014;64: 101–105. doi: 10.1159/000355440
4. Ralapanawa DM, Jayawickreme KP, Ekanayake EM, Jayalath WA. B12 deficiency with neurological manifestations in the absence of anaemia. BMC Res Notes [Internet]. 2015;8: 458 DOI 10.1186/s13104-015-1437-9
5. Barghouti FF, Younes LJ, Halaseh TT, Said SM. High frequency of low serum levels of vitamin B12 among patients attending Jordan University Hospital. East Mediterr Health J [Internet]. 2009;15: 853–860.
6. Baltaci D, Kutlucan A, Turker Y, et al. Association of vitamin B12 with obesity, overweight, insulin resistance and metabolic syndrome, and body fat composition; primary care-based study. Med Glas (Zenica) [Internet]. 2012;10(2): 203–210
7. Khader Y, Batieha A, Ajlouni H, El-Khateeb M, Ajlouni K. Obesity in Jordan: Prevalence, associated factors, comorbidities, and change in prevalence over ten years. Metab Syndr Relat Disord [Internent]. 2008 Jun;6(2): 113–20. doi: 10.1089/met.2007.0030.
8. Kimmons JE, Blanck HM, Tohill BC, Zhang J, Khan LK. Associations between body mass index and the prevalence of low micronutrient levels among US adults. Med Gen Med [Internet]. 2006;8(4): 59.
9. AlKhawtani D, Abulmeaty M. Assessment of Vitamin B12 status in patients with morbid obesity. Medcrave Journal [Internet]. 2017;6(6): 205–207. DOI: 10.15406/aowmc.2017.06.00181
10. Abu -Samak M, Khuzaie R, Abu-Hasheesh M, Fawzi M, Jaradeh, M. Relationship of vitamin B12 deficiency with overweight in male Jordanian youth. Science Alert [Internet]. 2008;8(17): 3060–3063.
11. Chakraborty S, Chopra M, Mani K, Giri A K, Banerjee P, et al., Prevalence of vitamin B12 deficiency in healthy Indian school‐going adolescents from rural and urban localities and its relationship with various anthropometric indices: a cross-sectional study. Journal of Nutrition and Dietetics [Internet]. 2018;31(4): 513–522
12. Sánchez H, Albala C, Herlramp F E, Verdugo R, Lavados M, Castillo JL, Lera L, Uauy R. Prevalence of vitamin B-12 deficiency in older adults. Rev Med Chil [Internet]. 2010 Jan;138(1): 44–52. doi: /S0034-98872010000100006
13. Stover P. Vitamin B12 and older adults. Curr Opin Clin Nutr Metab Care[Internet].2010Jan;13(1):24–27. doi: 10.1097/MCO.0b013e328333d157.
14. Loikas S, Koskinen P, Irjala K, Löppönen M, Isoaho R, Kivelä S, Pelliniemi T. Vitamin B12 deficiency in the aged: a population-based study. Age and Ageing [internet], 2007 Mar;36(2): 177–183.
15. Baltaci D, Deler MH, Turker Y, Ermis F, Iliev D, Velioglu U, et al. Evaluation of serum vitamin B12 level and related nutritional status among apparently healthy obese female individuals. [Internet]. 2017 Jan;20(1): 99–105. doi: 10.4103/1119-3077.181401.
16. Hughes C F, Ward M, Hoey L, McNulty H. Vitamin B12 and ageing: current issues and interaction with folate. Annals of Clinical Biochemistry [internet]. 2013;50(4): 315–329. doi.org/10.1177/0004563212473279.
17. Reinstatler L, Ping Qi Y, Williamson R, Garn J, Oakley G. Association of biochemical B12 deficiency with metformin therapy and vitamin B12 supplements. Diabetes Care [internet]. 2012 Feb;35(2): 327–333.https://doi.org/10.2337/dc11-1582
18. Dursun E, Obese children and B12 deficiency. Haydarpasa Numune Med J [internet]. 2019;59(1): 84–87.doi: 10.14744/hnhj.2018.19970
19. de Andrade S, França M M, Carvalho M, Pessoa de Araújo M. Serum vitamin B12, iron and folic acid deficiencies in obese individuals submitted to different bariatric technique. ABCD, arq. bras. Cir [internet]. 2016;29(1): 62–66.
20. Fidan C, Yagan, Gülcin G. Olcum, Duygu K, Haci B. Tugtekin. The relationship between obesity and serum Vitamin B12, folic acid, vitamin D concentrations in obese adults: a retrospective study. Endocrine Abstract [internet]. 2016;4(1): 183. DOI: 10.1530/endoabs.41.EP183.
21. World Health Organization. Obesity: Prevention and Management of the World Epidemic. Technical Report No. 916. Geneva: World Health Organization; 2003a.