ABSTRACT
Objective: To determine the incidence of thyroid nodules found
during extra-cranial carotid Doppler examination.
Methods: Between March 2005
and December 2007, a total number of 791 patients (354 females and 437 males) underwent
carotid Doppler examination for different causes. The study included thyroid
gland examination with gray scale and color Doppler. Patients with incidental
thyroid nodules were referred to endocrinology out-patient clinic for further
evaluation. Patients were divided according to age group and prevalence per
decade.
Results: Incidental thyroid nodules were
found in 98 (12.3%) patient. Bilateral nodules were found in 61 and unilateral
in 37 patients. Nodules equal or larger than one cm were found in 89 patients.
Fifty eight nodules were solid, 24 were cystic and 16 showed mixed
echogenesity. Fine needle aspiration biopsy was performed in 87 patients, and results
showed 79 (91%) benign and 8 (9%) malignant nodules. Most malignant nodules
were papillary carcinomas. Younger age groups (<55 yrs) were reported to
have a higher rate of thyroid nodules (18.3% vs.7.3%, RR: 2.51) (95%CI:
1.68-3.75; P=0.0000028).
Conclusion: Incidental thyroid nodules
are a common finding during carotid Doppler ultrasound examination and some of
these nodules may represent clinically significant pathology. Younger age
constitutes a group of people with higher risk for thyroid nodules.
Key words: Carotid
Doppler, Thyroid cancer, Thyroid nodule, Thyroid ultrasound
JRMS September 2010; 17(3): 29-32
Introduction
Sonographic examinations of
thyroid nodules is performed for evaluation of thyroid glands that seem
abnormal on palpation and is indicated for case detection of malignancy in
certain high risk situations.(1)
Thyroid nodules are common and
frequently benign. Ultrasound (US)
will detect incidental thyroid nodules in about 30-50% of population,(2-4) and thyroid nodules are present in 50-60%
of population at autopsy.(5-7)
Thyroid cancer constitutes 1%
of all cancers and 0.5% of cancer deaths.(8)
There is a recent increase in prevalence of incidental thyroid
nodules due to increase in US resolution, and now it is common to detect
non-palpable nodules (less than one cm in diameter).(9) Incidental
nodules are usually discovered during imaging studies for a various reasons
such as neck and chest computed tomography and carotid Doppler examination. In
a previous study by Khulaifat et al. the prevalence of incidental thyroid
nodules detected
by US in Jordanian population was 32.1% which is in agreement with international data (10-41%).(3,10)
|
Table
I. Prevalence of thyroid nodules per patients’
age groups
|
Age group (No. of patients)
|
No. of patients with
nodules (%)
|
|
27-35
(123)
|
18 (18.3 )
|
|
35-45
(117)
|
20 (20.4 )
|
|
45-55
(126)
|
29 (29.5)
|
|
55-65
(191)
|
18 (18.3)
|
|
65-71
(234)
|
13 (13.2)
|
|
≤55
years (366)
|
67(18.3)*
|
|
>
55 years (425)
|
31(7.3)
|
* p=0.0000028
≤55 years vs. > 55 yrs. Odd ration =2.85; 95% Confidence Interval
1.77-4.59 and a Relative Risk of 2.51; 95% CI;
1.68-3.75.
|
|
Table II. Ultrasonic features of
thyroid nodules
|
Nodule
consistency
|
No. (%)
|
|
Mixed
|
16 (16.3)
|
|
Solid
|
58 (59.1)
|
|
Cystic
|
24 (24.4)
|
|
TableIII.
Fine Needle
Aspirate Biopsy results
|
Cytology Results
|
No. (%)
|
|
Benign colloid nodule
|
60 (68.9)
|
|
Benign thyroid cyst
|
18 (20.6)
|
|
Papillary carcinoma
|
6 ( 6.8 )
|
|
Follicular carcinoma
|
2 ( 2.2 )
|
|
Lymphocytic thyroiditis
|
1 (1.1 )
|
|
Fine needle aspiration biopsy
(FNAB) is considered to be the most useful test for diagnosis of thyroid nodule
because of its high sensitivity and specificity.(5,11) Although
most of FNAB are diagnostic, 5-20% of biopsies are inadequate and insufficient
for diagnosis and require repeated aspiration.(12)
The aim of this study was to determine
the incidence of incidental thyroid nodules found during carotid Doppler
examination at King Hussein Medical Centre (KHMC).
Methods
This is a prospective study
performed at KHMC between March 2005 and December 2007, on a total of 791
patients (437 males and 354 females, age range: 25-79 years and mean age: 51.4
years) who underwent Doppler examination of their extra-cranial carotid systems
in the Radiology Department for various reasons such as tinnitus, stroke
evaluation and preoperative assessment prior to coronary bypass surgery. Examination
was performed by an experienced radiologist.
Ultrasound examination was
carried out using HDI 5000 ultrasound machine (ATL; Philips Medical Systems, Bothell, WA)
with a CL 10-5 MHz linear array transducer. Following carotid system examination,
incidental thyroid nodules were documented and evaluated for their location,
number, size, consistency (solid, cystic or mixed), vascularity and the
presence or absence of calcification. All incidental thyroid nodules ≥1 mm in
diameter were documented. All patients with known thyroid disease or history of
malignancy elsewhere were excluded from this study.
Patients with incidental
nodules were evaluated and followed up at the endocrinology outpatient clinic. Follow-up
ultrasound and FNAB were recommended to patients with suspicious nodules (Fig. 1).
Informed verbal consent was
obtained from all patients. Patients were divided into two groups according to
age (≤55 years or older than 55) and rates of thyroid nodules per age decades
were reported.
Statistical analysis involved
calculation of the mean, standard deviation, percentages, Odd ratio (OR) and
Relative Risks (RR) using EPinfo 6 program.
A P value <0.05 was considered as significant.
Results
At least one incidental
thyroid nodule was demonstrated in 98 (12.3%) of the 791 patients referred for
carotid Doppler examination. The mean age for these patients was 58.14 and their
age ranged between 27 and 71 years, 64 (65%) were females and 34 (35%) were
males.
Patients were categorized into five age groups as
shown in Table I. The higher number of thyroid nodules was found in the 45-55
age group followed by the 35-45 age group. The older age group (>55 years,
n=425) showed the lowest rate of incidental nodules of 7.3% vs. 18.3% in those ≤55
years (Odds ratio =2.85; 95% Confidence Interval 1.77-4.59 and a Relative Risk
of 2.51; 95% CI; 1.68-3.75.p=0.0000028).
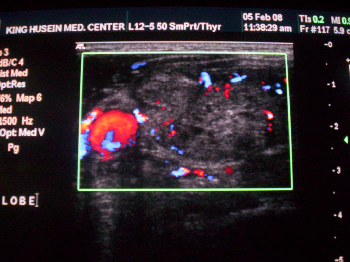
Fig.1. Large right thyroid solid nodule with spots of calcification and abundant vascularity. FNAB revealed papillary tumor
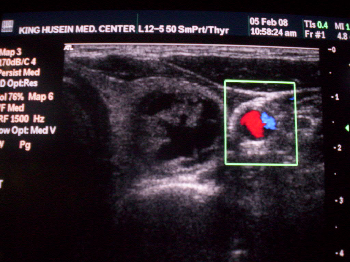
Fig. 2. Carotid
Doppler examination showing incidental left thyroid nodule of mixed
echogenesity. FNAB revealed benign colloid nodule
Thyroid nodules were bilateral
in 61 (62%) and unilateral in 37 (38%) patients. Eighty nine (91%) patients had
nodules equal to or larger than one cm, while nine (9%) had nodules less than one
cm. Nodules were solid in 58 (59%), cystic in 24 (24%) and 16 (16%) showed
mixed consistency (Table II).
US guided FNAB was performed
in 87 patients and repeated in 17 (19.5%) due to inadequate specimens. Table III
shows the results of these biopsies. Both solid and cystic lesions were
biopsied. No major complications were present. Minor complication included
local discomfort and subcutaneous hematoma.
Seventy nine (90.8%) patients
had benign nodules (Fig. 2) and eight (9.2%) had malignant nodules (Fig. 1). Malignant
and suspicious FNAB were scheduled for surgery and received the standard
surgical, radioactive iodine ablative and appropriate medical treatment as per
international guidelines.(1)
Malignant nodules were
papillary carcinoma in six patients (75%) and follicular carcinoma in two (25%)
(Fig.1). Most benign nodules were colloid lesions (Fig.2). One patient had lymphocytic
thyroiditis and 18 had simple thyroid cysts. Five patients with malignancy were
above 55 years (16.13%) vs. 4.5% of those below 55 years with thyroid nodules
who had FNAB (p=0.0322).
Discussion
Although the incidental
thyroid nodules are common findings on ultrasound examinations and
cross-section imaging, the incidence of incidental thyroid nodules found during
carotid Doppler is relatively unknown in our part of the
world. Five percent of the populations have palpable thyroid nodules and an additional
30-40% has non palpable nodules that can be found by imagining studies. Thyroid cancer is found in only 8% of
palpable nodules thus the appropriate interpretation of incidentally discovered
thyroid nodules found on imaging studies obtained for other indications is
important.(1-4)
Imaging of head and neck by
ultrasound, MRI, and CT scan for different causes other than thyroid
examination will reveal these incidental nodules, and with the ongoing
technical improvement of ultrasound machines, the incidence of discovered
nodules will increase.(13,14)
In this study we identified eight
new cases of thyroid malignancy which represent 9.2% of patients with incidental
nodules. The relatively high malignancy rate in this study compared with
national thyroid cancer prevalence is explained by selection of highly
suspicious nodules on ultrasound findings and older subjects in this study;
however this result is still in agreement with regional and international data.(15,16)
There is no optimal strategy
for treatment of the so called thyroid “incidentaloma”, and the management of these
nodules present a significant challenge to both endocrinologists and surgeons as
many recommendations on how to further investigate and approach these nodules
are available.(15,17)
In our view, incidental
thyroid nodules found during carotid Doppler or other head and neck imaging
should be reported and appropriately evaluated since they may affect patient
outcome. A special attention should be paid for younger age groups as they
constitute a higher risk for development of thyroid nodules with higher chance
of malignancy on long term depending on their longevity. The older group has
significantly higher rates of malignancy. We recommend routine thyroid view
during carotid Doppler especially in elderly patients.
Conclusion
Incidental
thyroid nodules found during carotid Doppler examination are common and should not
be overlooked since they may represent clinically significant pathology and
harbor malignancy. Appropriate workup should be considered for patients with
nodules especially when these nodules are larger than one cm in diameter or
look suspicious on ultrasound examination.
References
1. Dean DS,
Fatourechi V. Imaging the thyroid nodules. Endocrinology Update Mayo Clinic 2007; 2(4): 1-2
2. Tamsel S, Demirpolat G, Erdogan M, et al. Power Doppler US pattern of
vascularity and spectral Doppler US parameters in predicting malignancy in
thyroid nodules. Clinical Radiology 2007; 62:245-251.
3. Frates M, Benson C, Charboneau J, et al. Management of thyroid nodules
detected at US: Society of radiologists in ultrasound consensus conference
statement. Radiology 2005; 237:794-800.
4. Shabani Samghabadi M, Rahmani M, Saberi H, et al. Sonography and color Doppler
in the evaluation of cold thyroid nodules. Iran J Radiol 2004;
December: 13-16.
5. Natale F, Tedesco M, Mocerino R, et al. Feasibility, accuracy and
clinical relevance of a rapid thyroid evaluation during
carotid Duplex ultrasonography in
hypertensive patients. J Clin Hypertens 2007; 9:518-521.
6. Reading C, Charboneau J, Hay E, et al. Sonography of thyroid nodules.
A “classic pattern” diagnostic approach. Ultrasound Quarterly 2005;
21:157-165.
7. Rago T, Vitti
P, Chiovato L, et al. Role of conventional ultrasonography and color
flow-Doppler sonography in predicting malignancy in “cold” thyroid nodule. European
Journal of Endocrinology 1998; 138:41-46.
8. Hegedüs L. The thyroid nodule. N Eng J
Med 2004; 351:1764-71.
9. Cappelli C, Castellano M, Cumetti D, et al. The predictive value of
ultrasound findings in the management of thyroid nodules. Q J Med 2007;
100:29-35.
10. Khulaifat S,
Malkawi O, Haddad FH. Thyroid incidentalomas at King Hussein
Medical Center.
Jordan
Medical Journal 2001; 35(2): 145-147
11. Alexander E, Heering J, Benson C, et al. Assessment of nondiagnostic
ultrasound-guided fine needle aspirations of thyroid nodules. J Clin
Endocrinol Metab 2002; 87: 4924-4927.
12. Shetty S,
Maher M, Hahn P, et al. Significance of incidental thyroid lesions detected on
CT: Correlation among CT, sonography, and pathology. AJR 2006;
187:1349-1356.
13. Scissions R,
Hoskins M, Gillis J. Incidence of visualized thyroid abnormalities during
carotid Duplex evaluation. JDMS 2006; 22:161-164.
14. Liebeskind A, Sikora A, Komisar A, et al. Rates of malignancy in
incidentally discovered thyroid nodules evaluated with sonography and fine-needle
aspiration. J Ultrasound Med 2005; 24:629-634.
15. Steele S, Martin M, Mullenix P, et al. The significance of incidental
thyroid abnormalities identified during carotid Duplex ultrasonography. Arch
Surg 2005; 140:981-985.
16. National
Cancer Registry: Incidence of cancer in Jordan
2003.
17. Mitchell J,
Parangi S. The thyroid incidentaloma: An increasingly frequent consequence of
radiologic imaging. Semin
Ultrasound CT MRI 2005; 26:37-46.